

Abstract
Background/Aim: Carbonic anhydrase IX (CA9) catalyses the interconversion of carbon dioxide to carbonic acid and bicarbonate and is considered a putative biomarker of tumour hypoxia. We set out to evaluate the prognostic significance of CA9 in prostate cancer. Patients and Methods: Plasma samples were assessed from 68 men with high-risk localised prostate cancer treated with radical prostatectomy (RP) or radiotherapy (RT), and 20 men with castration-resistant prostate cancer (CRPC) treated with docetaxel chemotherapy between 2010 and 2012 at the Princess Margaret Cancer Centre, Canada. Results: Of the 68 patients with high-risk localised prostate cancer, 57 underwent RP and 11 underwent RT. Baseline CA9 was not associated with recurrence or prostate-specific antigen in either group (p=0.98 and 0.20, respectively). CA9 levels before chemotherapy correlated with overall survival (r=−0.37; two-sided p=0.11). Conclusion: Baseline CA9 in men with CRPC may portend a more aggressive prostate cancer phenotype with poorer survival.
- Prostate cancer
- CA9
- CAIX
- biomarker
Carbonic anhydrases are a family of metalloenzymes that catalyse the reversible conversion of carbon dioxide (CO2) to carbonic acid by adding water. Carbonic anhydrase IX (CA9) is a transmembrane glycoprotein that possesses an extracellular catalytic domain and is an important component of the pH-regulating machinery that is activated in response to chronic hypoxia, acidosis and oncogenic alterations (1). Its function is to hydrate pericellular CO2 and produce bicarbonate ions, which are then influxed by cell membrane transporters and consumed by neutralising low intracellular pH (a result of cellular metabolism). CA9 is normally expressed in upper gastrointestinal and gastrointestinal-associated tissues (2), and not normally expressed in human prostate tissue (3).
Hypoxia is a hallmark of many solid malignancies, due to a mismatch between oxygen demand and compromised supply from small and poorly formed microvasculature (4, 5). Amongst other effects, reduced oxygen availability leads tumour cells to reprogram their metabolism to the glycolytic pathway – the ‘Warburg effect’. Glycolysis increases the production of acidic metabolites such as lactate, resulting in a low intracellular pH, and is much less efficient at producing adenosine triphosphate (ATP). As ATP levels decline, cellular functions cannot be maintained, leading to cell death via necrosis or apoptosis (6). By neutralising cellular pH, expression and activation of CA9 demonstrates an effective adaptive cellular response to hypoxia, required for tumour cell survival (7).
Hypoxia in malignancy has been associated with poor prognosis and worse response to treatment, leading to interest in evaluating CA9 as a surrogate biomarker for prognosis and predicting response to anticancer treatment (8). CA9 expression in prostate cancer-associated fibroblasts has been shown to drive epithelial–mesenchymal transition in vitro and in vivo, suggesting that it might play a role in high-risk disease metastasising (9). High serum CA9 levels are also associated with poorer survival in clear cell renal cancer (10, 11) and high-risk, early-stage cervical cancer (12).
To our knowledge, an association between serum CA9 levels and risk of disease recurrence in high-risk localised prostate cancer (HRLPC), nor CA9 levels and survival in metastatic castration-resistant prostate cancer (CRPC) have been previously evaluated in men with prostate cancer.
Patients and Methods
Patient samples. Plasma samples were prospectively collected from consenting patients with newly-diagnosed HRLPC or metastatic CRPC attending clinic at the Princess Margaret Hospital (University Health Network; University of Toronto, Canada). Written informed consent for blood collection for research purposes was obtained from all patients on local Research Ethics Board-approved protocols. Specimens were collected from 68 men with HRLPC (57 and 11 treated with radical prostatectomy and radiotherapy, respectively) and 20 men with metastatic CRPC. High-risk disease was defined by the D'Amico criteria (13, 14) defined as clinical stage T3-T4N0M0 or Gleason score of 8-10 or prostate-specific antigen (PSA) >20 ng/ml.
Eleven patients with HRLPC were treated with pelvic and prostatic intensity modulated radiotherapy (pelvic dose of 46 Gy and total prostate dose 74 Gy) plus androgen deprivation therapy (e.g., luteinizing hormone releasing hormone-agonist injections given as concurrent and adjuvant therapy for a total period of three years) and 57 patients with HRLPC underwent radical prostatectomy with lymph node sampling or lymphadenectomy. Twenty patients with metastatic CRPC were treated with docetaxel chemotherapy at 75 mg/m2 every 3 weeks with prednisone (15). Control plasma CA9 samples were collected from healthy volunteers.
Plasma PSA levels were determined at baseline for each group of patients before treatment. Patients with HRLPC were then followed-up clinically for biochemical recurrence. Biochemical recurrence was defined as a serum PSA value above <0.05 ng/ml. Patients with CRPC were followed-up for survival.
Evaluation of CA9. Plasma CA9 levels were determined by enzyme-linked immunosorbent assay (ELISA) using the Oncogene Science kit manufactured by WILEX Inc. (Cambridge, MA, USA). Evaluation was carried out as per the instructions on the kit. CA9 levels were determined for each group of patients before and after treatment. The limit of detection was 2.5 pg/ml and the limit of quantification was 5 pg/ml.
Statistical analyses. Logistic regression was used to evaluate the association of CA9, and PSA levels with biochemical recurrence in patients with HRLPC, and Spearman's correlation coefficients were calculated for correlation between CA9 and PSA.
Wilcoxon signed-rank test was applied to investigate the pre- vs. post-treatment differences in CA9 and PSA values in CRPC. Spearman's correlation was used to calculate the correlation between time to death and PSA, CA9 or change in PSA or CA9. The Kaplan–Meier method was used for survival analysis. Differences in survival estimates between the patients was dichotomized by serum CA9 level according to the median value (155 pg/ml) using a two-sided log-rank test. The software program utilised was IBM SPSS Statistics for Macintosh, Version 22.0 (IBM Corp., Armonk, NY, USA). For all analyses, p≤0.05 was interpreted as being significant.
Results
Localised disease. A total of 68 men with HRLPC were evaluated for biochemical recurrence after local treatment. Baseline PSA and CA9 levels are reported in Table I. The baseline CA9 range was 60-1061 pg/ml for men with biochemical recurrence, and 38-1293 pg/ml for those without recurrence. Baseline CA9 and PSA were not associated with biochemical recurrence (p=0.98 and p=0.28, respectively). We found no significant correlation between PSA and CA9 in these patients (p=0.20).
CRPC. Twenty patients with CRPC were evaluated, and had a median age of 72 years. Their median follow-up was 14.1 months, and death of 17 (85%) patients was confirmed at the end of follow-up. The median baseline PSA was 155 (range=21-5838) ng/ml. PSA response ≥30% was achieved in 65% of patients, and 40% had a PSA response ≥50%. Change in PSA due to chemotherapy was statistically significant (p=0.02).
High-risk localised prostate cancer.
The median CA9 level before chemotherapy was 148 (range=38-1086) pg/ml and after chemotherapy was 116 (range=21-893) pg/ml. Twelve patients (60%) had a decrease in CA9 in response to chemotherapy. Change in CA9 due to chemotherapy was not statistically significant (p=0.24). There was no significant correlation between CA9 and PSA in CRPC (p=0.51).
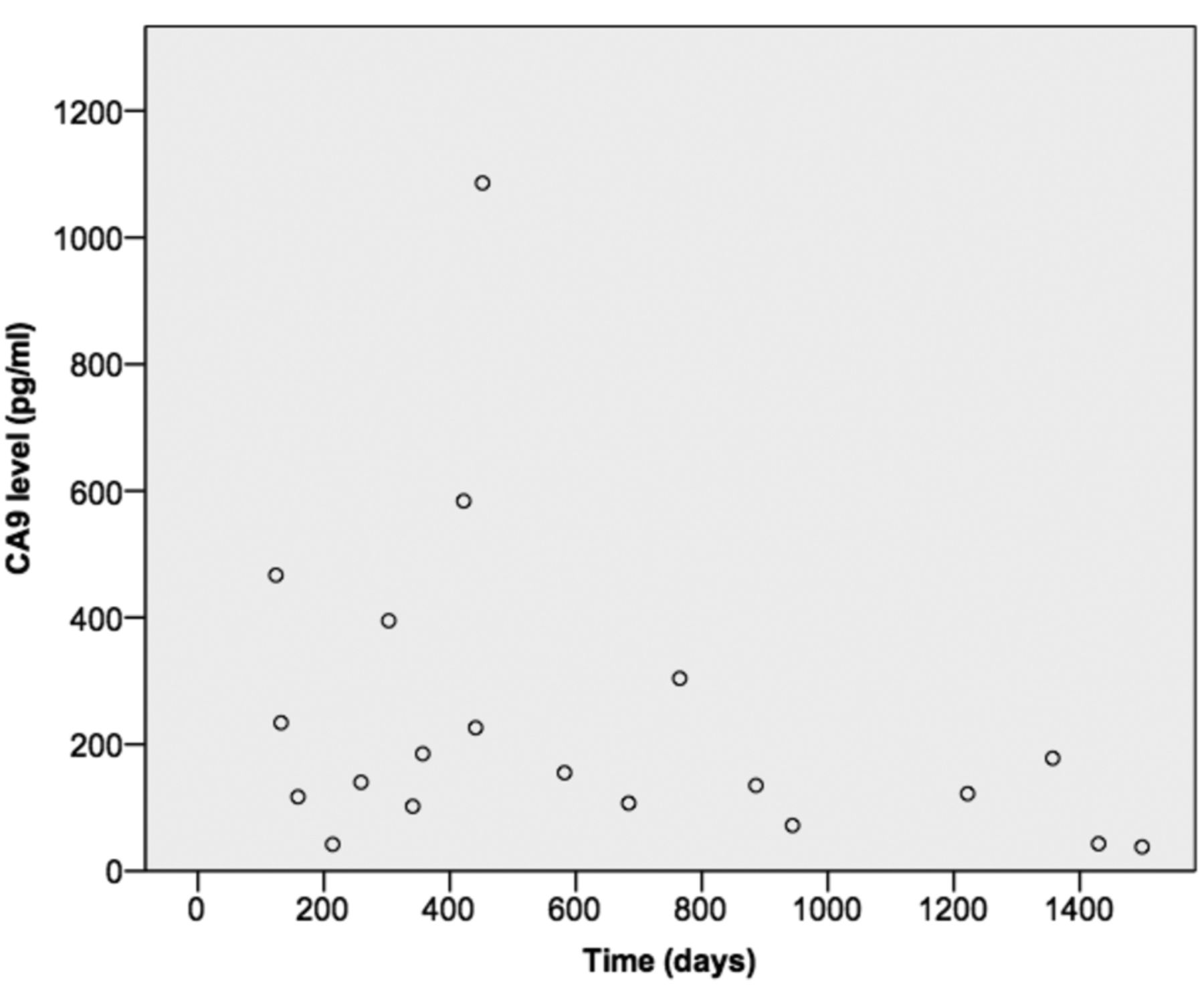
Baseline CA9 level correlated with overall survival (r=−0.37), and this approached statistical significance (two-sided p=0.11) (Figure 1). Kaplan–Meier survival analysis according to baseline CA9 level demonstrated a difference after dichotomizing by the median CA9 level (148 pg/ml) and approached statistical significance (two-sided p=0.135). There was no significant relationship between baseline PSA level and survival (p=0.34). The Kaplan–Meier survival plots according to baseline CA9 and PSA response ≥50% have similar p-values, and are reported (Figure 2 and 3, respectively). We found no significant relationship between CA9 response ≥50% and survival (p=0.85).
Discussion
The association between CA9 and tissue hypoxia provides a biological rationale for reduced efficacy of radiotherapy in the setting of elevated serum CA9. However, unlike the suggested role of baseline serum CA9 in determining risk of disease recurrence in renal cell cancer (16, 17) and vulvar cancer preoperatively (18), our findings suggest that baseline serum CA9 in HRLPC is not associated with disease recurrence after definitive local therapy. We also found that baseline PSA in HRLPC was not associated with disease recurrence, even though there is published evidence demonstrating an association in patients with high-risk prostate cancer (19, 20).

Relationship between pre-chemotherapy carbonic anhydrase IX (CA9) level and survival. Spearman's correlation coefficient (ρ)=−0.37 (p=0.11).
These conclusions are limited by a relatively small sample size. Furthermore, our sample population had HRLPC, in which the risk of disease recurrence is 70.6% overall, compared with low- and intermediate-risk disease. As a result, any utility of serum CA9 in predicting the likelihood of disease recurrence may be masked by the high recurrence rate. In contrast to our results, Milosevic and colleagues directly measured oxygen levels in clinically localised prostate tumours before radiotherapy and found that hypoxia was an independent predictor of early biochemical relapse and local recurrence in the prostate gland, particularly in patients with bulky tumours (21). In fact, oxygen is a known potent radiosensitizer, increasing the effectiveness of radiation by forming DNA-damaging free radicals. We also recognize that most patients with HRLPC were treated with radical prostatectomy (84%) and therefore our results may simply reflect the lack of utility of CA9 in predicting the likelihood of disease recurrence after radical prostatectomy for HRLPC.
Intratumoural hypoxia has been shown to alter cell-cycle checkpoints and down-regulate DNA-repair genes in prostate cancer cells, thereby driving genetic instability and tumor aggression (22-24). In this small cohort, baseline serum CA9 levels correlated negatively with survival in men with CRPC, and the level approached statistical significance. Furthermore, Kaplan–Meier analysis, the standard measure of association with survival, trended toward statistical significance after dichotomizing based on the median baseline serum CA9 level. Biologically, it makes sense that tumours demonstrating higher levels of CA9 (i.e. tissue hypoxia) would be less likely to respond to chemotherapy due to reduced tumour perfusion and therefore impaired delivery of docetaxel. In this small sample, we believe our findings do not discount the hypothesis that tumour hypoxia, as measured by serum CA9, portends a more aggressive prostate cancer phenotype with poorer survival. We are not aware of any published data identifying a relationship between survival and serum CA9 levels in CRPC.

Survival and baseline CA9 level.

{kind=link}
{kind=link}
{kind=link}
Survival and prostate-specific antigen (PSA) response.
More data evaluating the relationship between hypoxia, CA9 and outcomes in prostate cancer are needed before recommending its use as a biomarker in CRPC. Our data indicates that further research, in particular in the metastatic setting, is warranted. Furthermore, we anticipate that prospective identification of tumours with a high hypoxic load will allow for investigation of targeted agents that exploit this feature (25, 26).
Acknowledgements
The Authors wish to acknowledge Dr. Eitan Amir, who contributed to this article by consulting on the statistical analysis component. The assistance of the Prostate Cancer program at the Princess Margaret Cancer Foundation and the Stanley Tessis fund is acknowledged in making this research possible.
Footnotes
Conflicts of Interest
None.
- Received June 21, 2016.
- Revision received July 13, 2016.
- Accepted July 15, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved