

Abstract
Background: Influence of local recurrence (LR) on prognosis after a local excision (LE) for rectal cancer is unclear. Patients and Methods: A total of 152 patients were retrospectively assigned to one of three groups: Groups 1 and 2: complete and incomplete resection respectively, for low-risk carcinoma; group 3: high-risk carcinoma. We evaluated LR, distant metastasis (DM), overall survival, and cancer-specific survival (CSS). Results: LR rates were 10.4%, 43% and 29% for groups 1-3, respectively (p=0.002). In all three groups, DM incidence was low in patients without LR, but high in patients with LR (p<0.0001). Prior LR was an important risk factor for DM (hazard ratio: 14.1, 95% confidence interval=4.3-45.8, p<0.0001). DM significantly reduced CSS. Conclusion: There is a strong association between LR and DM independently in the cause of LR. Avoiding LE for high-risk carcinoma and complete LE of low-risk carcinoma are essential to reduce LR and DM.
- Early rectal cancer
- local excision
- local recurrence
- distant metastasis
- oncological outcome
It is not clear how local recurrence (LR) of early rectal cancer influences prognosis after a local excision (LE). Although salvage surgery is possible for most patients, survival is poor (1). Certain studies recorded a high incidence of distant metastasis (DM) in cases of LR, that worsened the prognosis (1-3). However, studies that compared LE and radical surgery for treating pT1 carcinomas found no difference in overall survival, despite higher LR rates after LE (4-7).
Due to the lower surgical risk compared to radical surgery, LE is preferred for treating elderly patients with high comorbidity (8-10). In follow-up, mortality from unrelated causes dominates cancer-related deaths; consequently, the effect of treatment cannot be clearly evaluated solely by overall survival determinations (6, 10). Additionally, patients with early rectal cancer can survive many years, thus long-term studies are required to assess the influence of LR on prognosis by determining cancer-related death. Existing studies on cancer-specific survival (CSS) after LE of rectal cancer have provided inconclusive results (5, 7, 8, 12, 13).
Since 1985, we have been using LE as treatment for patients with early rectal carcinoma (14). The aim of the present study was to clarify the frequency of LR and DM and the overall survival (OS) and CSS after LE of rectal cancer dependent on tumor characteristics i.e. low- and high-risk carcinoma (15) and completeness of local excision. We hypothesized that independently from the cause of LR, the incidence of DM would be higher in patients with LR than in those without LR. We also hypothesized that a high risk of DM would reduce the final cure rate after LE of early rectal cancer.
Patients and Methods
This retrospective study included all patients (n=213) treated with LE for rectal carcinoma from September 1985 to December 2007 identified in a prospectively maintained database at the Department of General and Abdominal Surgery of the University Medical Center Mainz, Germany. Patients were excluded when they had undergone non-curative resection (n=1), had synchronous colorectal cancer (n=4), or synchronous DM (n=1), had undergone neoadjuvant chemoradiotherapy (n=4), or had undergone immediate radical surgery after LE (n=51). A total of 152 patients with adenocarcinoma treated with LE alone were enrolled in the study.
LE was performed according to the technique described by Buess et al. (16) or Parks (17). In all cases, the planned treatment was a full-thickness, en bloc excision of the tumor and the underlying muscular wall of the rectum, with a 1-cm margin of normal tissue.
After discharge from the hospital, the patients were followed-up at the Oncology Department of the hospital with regular visits, according to a standardized program, until the fifth postoperative year. In 2011, the follow-up data for all patients were updated by contacting the patients and their families, treating physicians and hospitals to determine the vital status, the presence/absence of disease, the results of visits, the date and treatment of tumor recurrence, and the date and cause of death. Death certificates were ordered for all deceased patients and by combining with follow-up data it was clarified whether rectal cancer recurrence was present at the time of death.
The pathological features were recorded based on the original pathology report. We recorded the type of resection and the size of the tumor. The lateral and deep resection margins were classified as free of cancer (R0), with microscopic involvement (R1), or determination not possible (RX). The minimal distance was the minimum distance of the tumor from the lateral or deep resection margin, and we distinguished between ≤1 mm and >1 mm distances (18-20). Tumor grade (G1-G4, or GX when grading was not stated) and tumor infiltration (pT1-3) were determined according to current TNM guidelines (21). Lymphovascular invasion was present (L1), absent (L0), or not stated (LX). In patients with pT1 disease, we retrospectively performed blinded determinations of submucosal infiltration (22).
Patients were allocated to one of three risk/treatment groups: low-risk carcinoma (pT1, G1/2, L0, LX) with R0 resection; low-risk carcinoma with incomplete resection (≤1 mm minimal distance); and high-risk carcinoma (pT1, G3/4, GX or L1, pT2, pT3).
Local or distant failure (LR or DM, respectively) was determined according to the site of the first relapse. LR was defined as clinical, radiological, or histological evidence of a recurrent tumor in the rectum or inner pelvis, irrespective of DM. DM was defined as radiological evidence of tumor spread, with or without LR. In the case of simultaneous (within 4 weeks) local and distant relapse, the patient was added to both groups (LR and DM). OS was defined as the time from LE to death, irrespective of cause. CSS was defined as the time from LE to death due to rectal cancer. Deaths due to rectal cancer were defined as a tumor recurrence existing at the time of death irrespective of cause of death or mortality after surgery for recurrence; all other causes of death were not considered cancer-related (23). Recurrence-free survival was defined as the time from LE to LR or DM. When both LR and DM occurred, the earlier event date was recorded. When neither LR nor DM occurred, patients were censored on the date the study ended (December 31, 2011. All patients provided their informed consent for data collection and evaluation.
Statistical analysis. Patients' characteristics are described with percentages, medians, or mean values. p-Values for comparisons between sub-groups were assessed with the Chi-square test or Fisher's exact test, as appropriate.
The Kaplan–Meier method was used to estimate the risk of LR, DM, and death over time. Survival times were compared between groups with the log-rank test (univariate analysis). Cox regression was used to assess, simultaneously, multiple influences on DM. p-Values were unadjusted and are presented in the text and the tables. Confidence intervals were evaluated at 95% (95% CI). All statistical analyses were performed with the R environment for statistical computing, version 3.1.2 (24).
Results
Out of 152 patients with rectal cancer 133 (87.5%) underwent transanal endoscopic microsurgery (TEM) and 19 (12.5%) LE according to Parks. A total of 96 (63.2%) had R0-resected low-risk carcinoma, 14 (9.2%) had incompletely resected low-risk carcinoma (≤1 mm), and 42 (27.6%) had high-risk rectal cancer (Table I). The median follow-up considering the whole patient cohort was 8.7 (range=0.1-25.1) years and the median follow-up for patients alive at the end of the study (n=65) was 12.7 (range=3.6-25.0) years. For the living patients, follow-up was longer than 5 years in 63/65 (97%) and longer than 10 years in 42/65 (65%). Death occurred in 87/152 (57.2%) patients: 19 (22%) from rectal cancer, 10 (11%) from a second malignancy (not counted as rectal cancer related deaths), 53 (60%) from other causes, and 5 (6%) from unknown causes.
Local recurrence and DM. Patients with completely resected, low-risk carcinomas had a LR rate of 10.4% (10/96). The median time to LR was 1.4 years. The 5- and 10-year probabilities of LR were 8.7% (95% CI=2.8-14.3%) and 12.0% (95% CI=4.6-8.9%), respectively (Kaplan–Meier). DMs were observed in 7/96 (7%) patients. The median time to DM was longer (4.5 years) than the median time to LR. The 5- and 10-year probabilities of DM were 4.7% (95% CI=0.1-9.1%) and 9.2% (95% CI=2.4-15.5%), respectively. Among the 96 patients in the low-risk group, two (2%) had DM without LR. Among the 10 patients with LR, five (50%) had DM (p<0.0001). Among the five patients with both, DM was synchronous with LR in two, and were metachronous in three.
Among 14 patients with incompletely resected low-risk carcinoma (pT1, G1/2, L0/X), LR occurred in six (43%) after a median time of 2.5 years. The 5- and 10-year probabilities of LR were 35.7% (95% CI=5.0-56.5%) and 44.9% (95% CI=9.7-66.4%), respectively (Kaplan–Meier). DMs occurred in 3/14 (21%) patients, after a median of 1.7 years. Out of the six patients with LR, three (50%) had DM. Out of the eight patients without LR, none had DM (p=0.05) (Table II). Both the 5- and 10-year probabilities of DM were 15.4% (95% CI=0-32.9%). In this group, DM and LR appeared simultaneously in two patients, and DM appeared later than LR in one.
Among the 42 patients with high-risk carcinoma, one (2%) lacked clarity in the LR determination. The remaining patients had an LR rate of 29% (12/41). The median time to local recurrence was 1.1 years. Both the 5- and 10-year probabilities of LR were 33.3% (95% CI=15.7-47.2) (Kaplan–Meier). DMs were observed in 5/41 (12%) patients. Table II shows the results of the sub-group analysis. The time to DM (median=3.2 years) was longer than the time to LR. The 5- and 10-year probabilities of DM were 12.4% (95% CI=1-23.2%) and 15.9% (95% CI=2-27.9%), respectively. DM appeared without LR in 2/29 (7%) patients, and both DM and LR occurred in 3/12 (25%) patients (p=0.1; Table II). In the latter group, DM and LR were synchronous in two patients, and DM occurred after LR in one.
Characteristics of 152 patients with rectal carcinoma treated with local excision alone in this study.
The three patient groups had significantly different LR rates (p=0.002), but similar DM rates (p=0.399).
Among the entire evaluable cohort, 28/151 (18.5%) had LR and 15/151 (9.9%) had DM. Among those without LR, 4/123 (3.2%) had DM; among those with LR, 11/28 (39%) had DM (p<0.0001). In 6/11 patients, DM occurred simultaneously with LR; in 5/11 patients, DM occurred after LR.
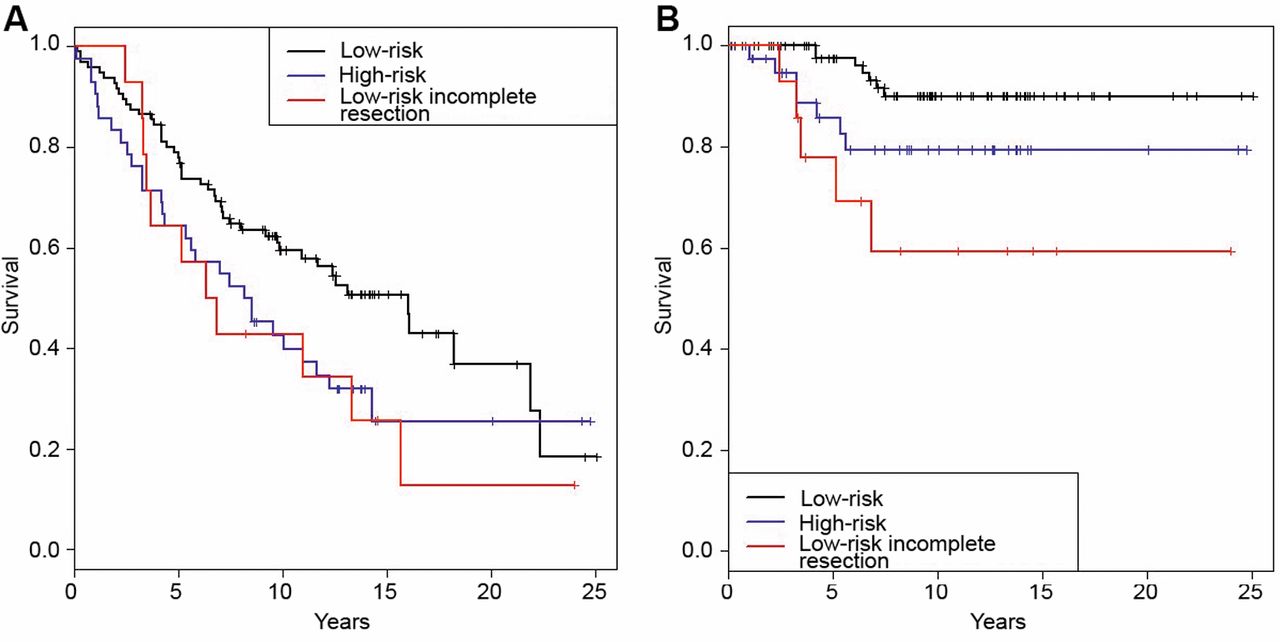
Survival. The median OS times were 16.0 years for patients with low-risk R0 resected carcinoma, 6.6 years for those with incompletely resected low-risk carcinoma, and 8.4 years for those with high-risk carcinomas. The three groups had similar 5- and 10-year overall survival rates (p=0.058; Figure 1A).
CSS significantly differed between the groups. The 5- and 10-year CSS rates, respectively, were 97.5% (95% CI=94.1-100%) and 90.0% (95% CI=83.2-97.4%) in the low-risk group (R0); 77.9% (95% CI=58.7-100%) and 59.4% (95% CI=36.9-95.5%) in the incompletely resected low-risk carcinoma group; and 85.7% (95% CI=75.6-96.0%) and 79.3% (95% CI= 63.9-89.3%) in the high-risk cancer group (p=0.0047 for the comparison of all three groups, p<0.001 for the comparison of the low-risk group vs. the incompletely resected low-risk group; Figure 1B).
Local recurrence (LR) and distant metastasis (DM) in patients with incompletely resected (≤1 mm) low-risk or high-risk rectal carcinoma after local excision alone.
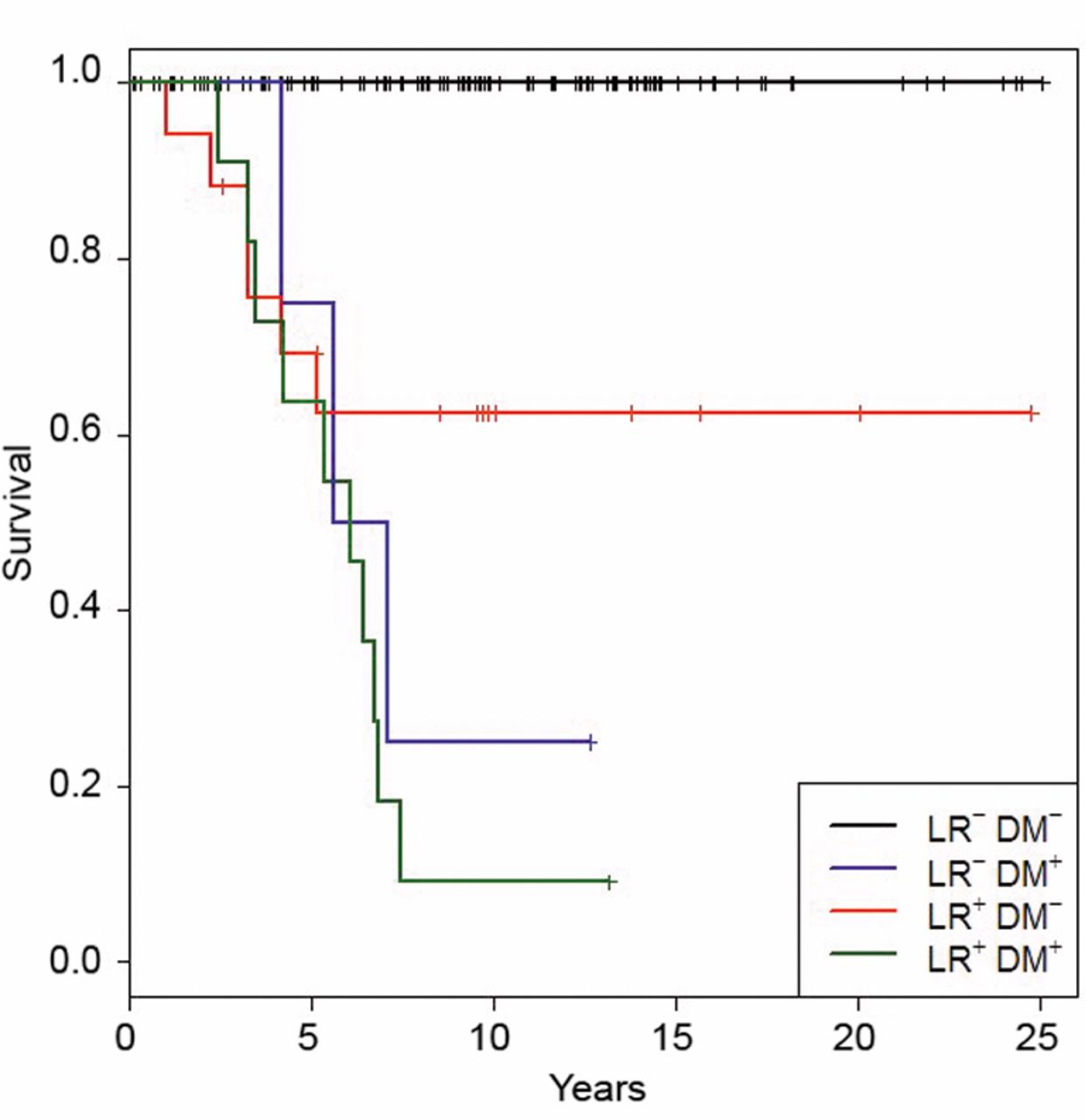
Influence of LR and DM on prognosis. To investigate the influence of LR and DM on prognosis, we analyzed the whole cohort, due to the small number of events for each group. The median OS time was 13.3 years for patients with neither LR nor DM; 8.6 years for patients with LR only; 6.4 years for patients with DM only; and 6.1 years for patients with LR and DM. The differences between the groups were significant (p=0.00575).
The 5- and 10-year CSS rates, respectively, were 69.3% (95% CI= 50.1-95.6%) and 62.4% (95% CI= 42.5-91.6%) in patients with LR but without DM; 75.0% (95% CI=42.6-100) and 25.0% (95% CI=45.8-100%) in patients with DM but without LR; and only 63.6% (95% CI=40.7-99.5%) and 9.1% (95% CI=1.4-58.9%) in patients with both LR and DM. The differences between the groups were significant (p≤0.0001; Figure 2).
Cox regression analysis. After adjusting for age, we found that prior LR was an important risk factor for developing DM (Cox regression hazard ratio=14.1, 95% CI=4.3-45.9; p<0.0001).
Discussion
The results confirmed that LR rates after LE of rectal carcinoma were different in patients with high- and low-risk carcinomas (11, 25). However, among patients with LR, the incidence of DM was high in all groups, independent of the pathology of the primary tumor and cause of LR. The causes of LR in the three groups are different and relate to the aggressive tumor biology of high-risk carcinoma, the incomplete resection of low-risk tumors, or are unknown in patients with completely resected low-risk carcinoma. A total of 11/15 DMs occurred simultaneously or later than LR, and in two groups, the median interval to DM was longer than the time to LR, similar to the observations of Ptok et al. (26). These points suggest a causal association between the development of LR and DM, although our results do not provide definitive proof of this.
The finding of higher DM rates among patients with LR than among those without LR was consistent with results after radical surgery (27) and with results of other follow-up studies on LE for rectal cancer (4, 5, 7, 11, 18, 28-31).
DM significantly reduced the prognosis of patients. The 10-year CCS was 62.4% among patients with LR but without DM, and 9% for patients with both LR and DM. In both the low- and high-risk carcinoma groups, about half the patients with LR underwent salvage surgery (R0); out of these, 25% developed DM, with or without LR (data not shown). This finding was consistent with previous studies on salvage surgery for LR, where high rates of DM were found in follow-up, and the presence of DM worsened the outcome (1-3). Thus, compared to radical surgery, LE treatment of rectal cancer is complicated by both a higher LR rate (32) and a high risk of DM associated with LR. This association reduces the chance of a cure with salvage surgery; consequently, the good prognosis expected at the beginning of therapy, particularly in cases of low-risk carcinoma, may only be achieved in half of the patients with LR, at best.
Our results suggest that reducing LR will concomitantly reduce the risk of DM and improve the prognosis after LE for rectal cancer. An important point is patient selection. The unfavorable results in patients with high-risk carcinoma (Table II) does not justify LE alone as treatment. Another point is completeness of LE to ensure safe lateral and deep resection margins. TEM seems to be superior to other forms of LE (18). We found an insignificant trend for lower LR rates after TEM than after the Parks resection (data not shown). A standardized pathological assessment of a resected specimen is necessary to provide better evaluation of the completeness of LE. In cases of incompletely resected, low-risk carcinoma, an immediate repeat LE should be performed to reduce the risk of LR. In cases of LR after LE, extended staging should detect or exclude DM. Surgical therapy of LR should ensure complete local resection to avoid another LR. Most LRs after LE are more advanced than was the primary carcinoma (33); thus, a radical salvage procedure should be preferred to re-excision (34).

Overall (A) and cancer-specific (B) survival after local excision of low-risk R0 resected carcinoma, incompletely (≤1 mm) resected low-risk rectal carcinoma and high-risk rectal carcinoma.
This study has certain limitations. The study design was a retrospective analysis of prospectively collected data; it was a single-center study; the recruitment time was long; some pathological data were missing; and the small numbers of patients in the sub-groups limited the strength of the conclusions drawn. The strength of the study was the long-term follow-up data for almost all patients.
In conclusion, this study showed that the risk of DM significantly increased in cases of LR independently from the cause of LR. Unfavorable tumor characteristics and incomplete resections seemed to be the primary factors that influence the association between LR and DM. Avoiding LE for high-risk rectal carcinoma and performance of a locally complete LE of low-risk carcinoma are essential to reduce LR and consequent DM, and improve the final outcome after LE of early rectal carcinoma.
{kind=link}
{kind=link}
Influence of local recurrence (LR) and distant metastasis (DM) on cancer-specific survival (CSS) after local excision of rectal carcinoma. LR−: Without LR; LR+: with LR; DM−: without DM; DM+: with DM.
- Received November 21, 2015.
- Revision received December 21, 2015.
- Accepted December 23, 2015.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved