

Abstract
Background: The efficacy of platinum- and ifosfamide-based chemotherapy regimens as salvage treatment in metastatic breast cancer (MBC) has not yet been sufficiently evaluated. Patients and Methods: Patients with MBC treated with cisplatin plus ifosfamide with (PEI) and without (PI) etoposide in our clinic between 04/2005 and 04/2014 were retrospectively analyzed. Results: A total of 20 patients (median four prior chemotherapies) treated with PEI/PI were identified, out of whom 18 were evaluable for objective response. Treatment with PEI/PI resulted in one complete remission, nine partial remissions and two cases of stable disease. The median (range) progression-free survival was 4 (0-18) months and median overall survival from therapy initiation was 8.5 (0-50) months. PEI/PI therapy caused grade 3/4 toxicities (mainly hematological) in 80% of patients. Conclusion: PEI/PI is an adequate salvage treatment for patients with MBC but cannot be generally recommended due to toxicity. However, comparison with platinum monotherapy trials suggests that PEI/PI might be a more effective treatment for patients with triple-negative breast cancer.
- Metastatic breast cancer
- chemotherapy
- platinum
- etoposide
- ifosfamide
According to the International Agency for Research on Cancer, breast cancer is the most common cancer in women worldwide, representing approximately 25% of all malignant tumors in females (1). To date, patients developing metastatic breast cancer (MBC) still have a very limited prognosis (2). However, especially due to new treatment options and the increase of targeted and individualized therapy selection, the median overall survival (OS) of patients with MBC appears to have improved over the past decades (3, 4). To this day, chemotherapy remains the most effective treatment option in case of progressive metastatic disease with the rapid need for remission (5).
Depending on the therapies applied in the neo- and adjuvant setting, taxanes and anthracyclines represent the most effective first- and second-line chemotherapies in the context of MBC (6). However, the best possible therapy thereafter remains controversial (7, 8). Numerous other cytostatic substances, such as 5-fluorouracil, vinorelbine, gemcitabine, or halichondrin B analog eribulin, have been proven more or less effective for single-agent treatment of MBC (9-14). Platinum-based chemotherapies were also shown to be potent treatment options for this indication (15-19). However, taking into account the high number of patients affected, as well as the limited number of chemotherapy agents applicable to this entity, additional effective chemotherapeutic treatment options for MBC are needed.
Platinum- and ifosfamide-based therapy regimens are standard in the treatment of germ cell tumors, possessing high anti-tumor activity via induction of DNA crosslinks and strand breaks, as well as through the inhibition of DNA-repair mechanisms (20). Although they are not a standard therapy for MBC, they have been administered as salvage treatment in heavily-pre-treated patients with MBC at our clinic. Yet the efficacy of platinum- and ifosfamide-based chemotherapies in MBC is currently unknown. Thus, we carried out a retrospective analysis evaluating the therapeutic potential of this regime as salvage treatment for MBC.
Patient characteristics at initiation of cisplatin plus ifosfamide with/without etoposide (n=20).
Patients and Methods
All patients with MBC treated with cisplatin plus etoposide with ifosfamide (PEI) or cisplatin plus ifosfamide (PI) at our clinic between April 2005 and April 2014 were retrospectively analyzed. The patients received cisplatin (20 mg/m2, days 1-5) plus ifosfamide (1200 mg/m2, days 1-5), with etoposide (75 mg/m2, days 1-5), or without, in 21-day cycles over six treatment cycles or until disease progression.
A clinical database was established including the following information for each patient: age, Eastern Cooperative Oncology Group (ECOG) performance status, tumor characteristics, characteristics of metastasis, pretreatments and disease progression. The response to therapy was assessed by using the Response Evaluation Criteria in Solid Tumors (RECIST) (21). In the context of PEI/PI treatment, we additionally evaluated the number of chemotherapy cycles, total dose of cytostatics, dose reductions and chemotherapy-associated toxicities, which were subsequently valued in accordance with Common Terminology Criteria of Adverse Events version 4.03 (22). Survival times were measured from initiation of Cisplatin plus Ifosfamide with/without Etoposide. The survival curves were calculated via the Kaplan–Meier method with MedCalc version 12.5.0.0. (MedCalc Software bvba, Ostend, Belgium).
Results
Overall, 20 patients with MBC treated with PEI or PI were identified. Ten patients (50.0%) were treated according to the PEI protocol and 10 (50.0%) underwent PI therapy, receiving a median (range) treatment of 4.5 cycles (range=1-8) in total. The median age at first diagnosis of breast cancer was 41 (28-62) years. Twenty-five percent of patients presented with metastases at the time of initial diagnosis. Nine patients (45.0%) were identified as having triple-negative breast cancer (TNBC), whereas seven (35.0%) showed expression of hormone receptors. Patients' characteristics at treatment initiation are shown in Table I.
Response to cisplatin plus ifosfamide with/without etoposide (n=18).
Efficacy. Eighteen patients were evaluable for objective response as one patient discontinued the therapy due to progressive peripheral neuropathy after the first cycle, whereas another patient transferred to a different clinic where the treatment was not continued.
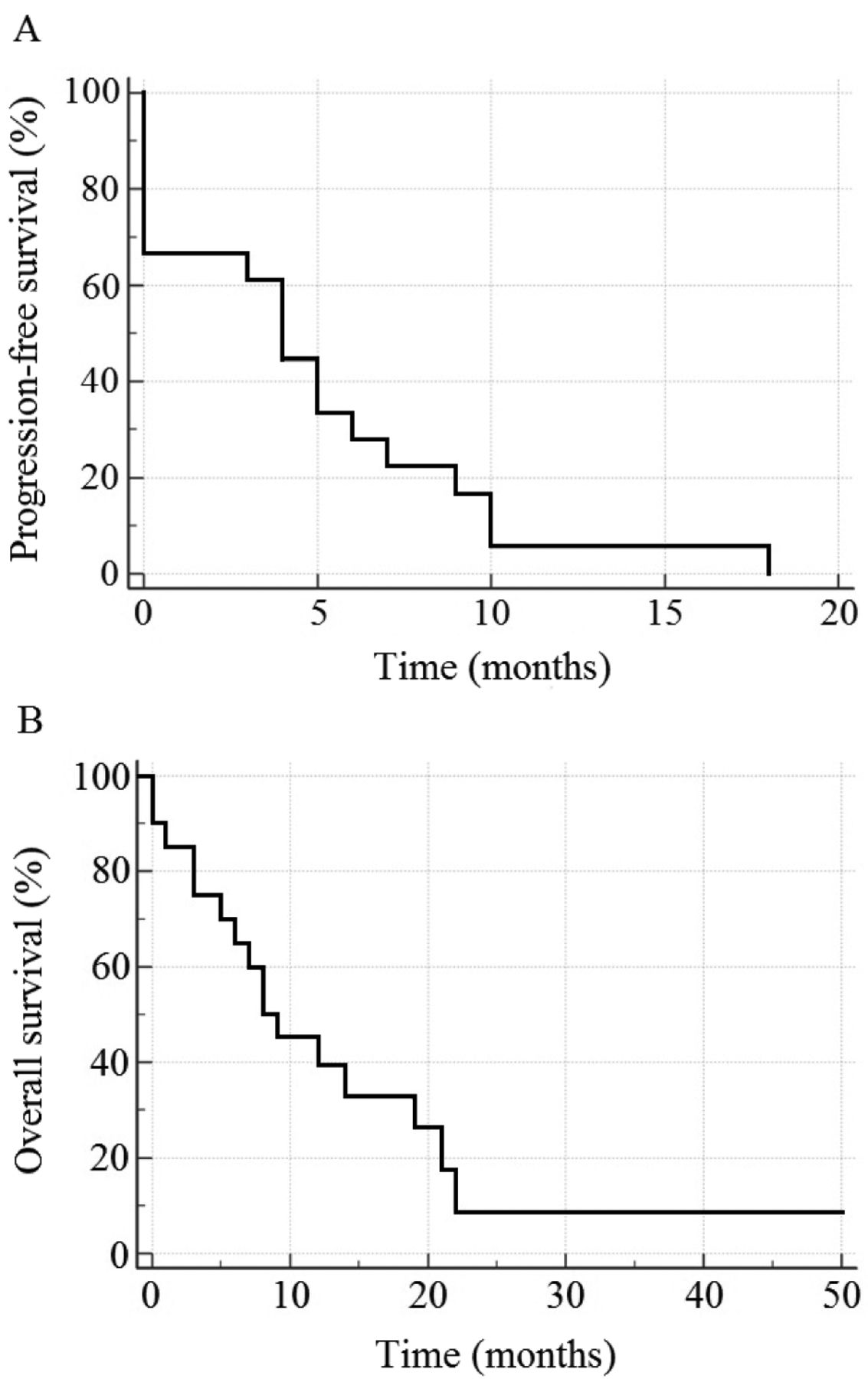
Response was evaluated after the second or third cycle of chemotherapy, or at clinical signs of progression. Results are summarized in Table II. The objective response rate (ORR) was 56.6% (62.5% in TNBC and 44.4% in non-TNBC patients), while the median progression-free survival (PFS) was 4 (0-18) months and the median overall survival (OS) from initiation of PEI/PI treatment was 8.5 (0-50) months (Figure 1). The PFS of patients with TNBC and non-TNBC was 4 months for both. OS of patients with TNBC was 8 months versus 11.5 months in patients with non-TNBC. With a median follow-up time of 6.5 (0-45) months, four patients (20.0%) were still alive by the end of observation period in April 2014.
Toxicity. The treatment with PI and PEI caused severe hematological toxicities (CTCAE grade 3/4) in 16 out of 20 patients (80.0%) and nausea/emesis (CTCAE grade 3/4), as the most common severe non-hematological toxicity, in three patients (15.0%). All registered chemotherapy-associated toxicities are listed in Table III.
In total, seven patients (35.0%) required additional hospitalization during chemotherapy (four due to febrile neutropenia, one due to febrile infection without neutropenia, and two for recurrent transfusion of either platelets or erythrocytes).
As mentioned above, one patient discontinued therapy due to peripheral neuropathy CTCAE grade 3. In two patients, treatment was terminated according to the patient's wish after the fourth and eighth cycle, having achieved a complete and a partial remission, respectively (one due to persistent nausea/emesis, one in order to have a hospitalization-free period).

{kind=link}
Progression-free survival (A) and Overall survival (B) of patients from initiation of cisplatin plus ifosfamide with/without etoposide.
Discussion
Despite improvements in chemotherapeutic treatment of MBC, there is still an urgent need for new chemotherapeutic options. In this context, we retrospectively evaluated the therapeutic potential of PEI/PI in heavily-pre-treated patients with MBC, finding initial tumor control (ORR) in more than 50% of patients. However, analysis also revealed only brief median PFS and overall survival, as well as severe treatment-induced toxicities.
Nevertheless, it has to be kept in mind that the data presented herein are based on the analysis of a small number of patients who were heavily-pre-treated and of whom 45% suffered from TNBC. To our knowledge, only two prior studies investigated the efficacy of a combination of platinum and ifosfamide in MBC, which was applied to 50% of patients of the present study (23, 24).
Cisplatin plus ifosfamide with/without etoposide-associated toxicities (n=20).
Halim and Wahba investigated the efficacy of PI in 40 patients with metastatic TNBC mainly as second-line treatment in a prospective phase II study, finding an ORR of 35%, whereas the median PFS and OS were 6 and 12 months, respectively (23). In addition, another large retrospective study performed by Staudacher et al. analyzed 143 patients with MBC (median of two prior palliative chemotherapies) treated with platinum-based chemotherapies, 70.2% of them receiving cisplatin and ifosfamide (24). Here the ORR was found to be 29%, while PFS and OS were 5 and 11 months, respectively.
It is noteworthy that both studies reported considerably lower initial tumor response rates than in the present investigation, while at least in the trial conducted by Halim and Wahba, the OS and PFS were notably longer. As a possible explanation for the higher ORR, 50% of our patients received the more intensive-therapy regimen PEI, whereas the lower median PFS and OS may have resulted from the more intensive pretreatment in the present cohort (median of four prior chemotherapies).
Interestingly, Staudacher et al. found patients with TNBC to have a higher ORR than those with non-TNBC (33.3% versus 22.0%), which did not translate into a difference concerning PFS and OS (5 and 11 months, respectively). This was interpreted by the authors as evidence for the efficacy of platinum-based chemotherapy especially in TNBC as these patients usually have a worse prognosis.
In the present study, we also found a higher ORR in TNBC than in non-TNBC (62.5% versus 44.4%). However, although our retrospective analysis showed similar PFS (4 months each) for patients with TNBC and those with non-TNBC, the OS of those with TNBC was considerably shorter (8 versus 11.5 months). We deduce that in the present study, the combination of platinum and ifosfamide could not offset the worse prognosis of the patients with TNBC. Thus our results contrast the findings by Staudacher et al., which may be explained by the small and heterogeneous cohort of the present analysis. Nevertheless, our results can be taken as evidence that PEI/PI is an effective treatment option also for patients with non-TBNC.
Taking together the data presented here, as well as the studies cited above, concerning the efficacy of platinum-based combination treatment with ifosfamide, it is noteworthy that the ORR in all three studies compared well or out-performed the results of carboplatin monotherapy in TNBC in the first- and second-line settings (25). Therefore, evaluation of platin-based combination treatment with ifosfamide would be of great interest in first-line treatment of TNBC, especially taking into consideration recent results from a phase III study reporting a PFS of 7.73 months for the combination of cisplatin with gemcitabin in patients with TNBC in first-line treatment (26).
However, several points have to be taken into consideration regarding PEI/PI chemotherapy in patients with MBC. Treatment causes severe hematological and non-hematological toxicities in the vast majority of patients, whereas although the initial response rate is high, the PFS and OS are relatively short. Moreover, PEI/PI is usually administered in an inpatient setting, taking on average five days, which is a considerable disadvantage regarding the quality of life, especially in patients treated with palliative intent. Thus, PEI/PI cannot be recommended as a standard therapy in pre-treated patients with MBC. Nevertheless, PEI or PI treatment is an intensive regimen that may provide an option for heavily-pre-treated patients with MBC with rapid need for remission. Thus, further prospective investigations are needed, in order to definitively evaluate the efficacy and toxicity of PEI/PI in patients with MBC.
Footnotes
* These Authors contributed equally to this study.
- Received April 21, 2015.
- Revision received May 27, 2015.
- Accepted May 29, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved