

Abstract
Iceland has a total population of 300,000 inhabitants. All patients consulting for symptoms of the lower digestive tract during a four-year period (2003-2006) were subjected to a colonoscopic examination; all polyps were endoscopically removed. Out of the total 3,037 colorectal adenomas (CRAs), 308 (10.2%) were traditional serrated adenomas (TSAs). TSAs were divided according the predominant histological phenotype (>50%) into those with ectopic crypt formations (ECF), and those with unlocked serrations (US). ECF-TSA accounted for 5.9% (178/3037) and US-TSA for 4.3% (130/3037). The majority of patients with ECF-TSA and US-TSA were ≥60 years of age (74.1% and 76.2%, respectively). Notwithstanding, when patients having advanced adenomas (with high-grade dysplasia, with or without intramucosal carcinoma) were listed by age, those with ECF-TSA were significantly younger than those with US-TSA (p<0.05). ECF-TSA were more frequently left-sided (71.8%), whereas US-TSA were more frequently right-sided (60.0%). Invasive carcinoma evolved more frequently in ECF-TSA (7.8%) and in US-TSA (7.7%) than in tubular adenomas and in villous/tubulovillous adenonas (0.1% and 4.4%, respectively). Comparative studies indicated that the incidence rates/year of ECF-TSA and US-TSA were significantly higher in Iceland than in Sweden or in Italy (p<0.05). Genetic and putative epigenetic (environmental) factor(s) might account for the high incidence rate/year of ECF-TSA and US-TSA in this country.
- Colorectal adenomas
- traditional serrated adenomas
- incidence rate
- invasive carcinoma
- nationwide survey
- Iceland
Colorectal carcinoma (CRC), the third most commonly diagnosed type of cancer in Europe and the USA (1), usually evolves from conventional adenomas via the adenoma–carcinoma sequence (2). Conventional adenomas exhibit tubular, tubulo-villous or villous structures, either with low-grade or high-grade dysplasia, increased cell proliferation and progressive accumulation of mutations of V-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog (KRAS) and chromosomal instability (2). Progression from conventional adenomas to carcinoma evolves via the adenomatous polyposis coli (APC) pathway. In this paradigm, hyperplastic polyps were considered innocuous. However, the detection of right-sided interval carcinomas following a negative colonoscopic examination has suggested the possibility of an alternative pathway of carcinogenesis for hyperplastic polyps (3).
In 1990, Longacre and Fenoglio-Preiser described an adenoma phenotype characterized by dysplastic epithelium lining serrated crypts with unlocked serrations (US) (4). It was called serrated adenoma. Subsequently, Jass postulated that the traditional adenoma–carcinoma sequence might not apply to sporadic colorectal cancer with microsatellite instability-high (MSI-H), in which >30% of the microsatellite marker panel is mutated, and that the serrated-carcinoma pathway comprising hyperplastic polyps, mixed polyps and serrated adenomas, could be the missing link of colonic carcinogenesis (3). More recently, Snover et al. coined the term traditional serrated adenoma (TSA) (5) and Torlacovic et al. described a TSA with tubulovillous architecture having multiple tiny ectopic crypt formations (ECF) (6), previously reported by Haramis in adenomas of the intestine of mice (7).
The purpose of the present work was to assess in the population of Iceland, the frequency of TSA having ECF (ECF-TSA) or US (US-TSA), including progression to invasive carcinoma. Possible differences in the biological attributes of ECF-TSA and of US-TSA were also explored.
Materials and Methods
This study was approved by the Ethical Committee of Iceland (VSNb2004090031). The present nationwide survey was carried out on all patients consulting for symptoms of the lower digestive tract in the entire population of Iceland (300,000 inhabitants) during a four-year period. Consulting patients were subjected to a colonoscopic examination. Between January 2003 and December 2006, a total of 19,424 endoscopic examinations (13,572 colonoscopies and 5,852 sigmoidoscopies) were performed in Iceland (mean=4856 endoscopies per year). All detected colorectal polyps were removed and re-submitted to histological evaluation to the three pathology laboratories existing in Iceland: Landspitali University Hospital, Reykjavik, Reykjavik Private Clinic, or Akureyri District Hospital. Filed hematoxylin and eosin (H&E)-stained sections from colorectal adenomas (CRA) were reviewed by one of us (CAR). Sections from three ECF-TSA and from three US-TSA were histochemically stained with PAS-Alcian Blue, pH 2.5 to visualize sulfated and carboxylated acid mucopolysaccharides and sulfated and carboxylated sialomucins; with Ki67 (batch MIB1) to assess the distribution of DNA synthetizing dysplastic cells; and for p53 to detect p53 up-regulation. Hyperplastic polyps and sessile serrated adenoma/polyp (8) were not included in this survey.
TSA were divided according the predominant histological phenotype (>50%). Lesions showing garlands of ECFs, that is microtubules (9-11) distributed sideways and within villous-like outgrowths, were classified as ECF-TSA. The ECFs were lined with slightly pseudostratified epithelium having dysplastic goblet cells, often with eosinophilic cytoplasm (Figure 1). Some ECF-TSA exhibited ECF configurations exclusively, while others in addition exhibited villous/villotubular configurations in the remnant adenomatous tissue. Lesions with dysplastic crypts furnished with saw-tooth-like structural changes due to unlocked epithelial folds were classified as US-TSA (Figure 2). Dysplastic cells were initially found in the lower part of the crypts (12). In larger US-TSAs, the dysplastic epithelium reached the luminal aspect of the elongated crypts. Dysplasia in ECF-TSA and in US-TSA was classified into low-grade dysplasia (LGD) and high-grade dysplasia (HGD) (9-11, 13). ECF-TSA and US-TSA exhibiting HGD without or with intramucosal carcinoma were recorded as advanced TSA. TSA with neoplastic cells penetrating through the muscularis mucosa and invading into the submucosal tissues or beyond were classified as TSA with invasive carcinoma. The microtubular pattern was often retained in invasive carcinoma evolving from ECF-TSA (11) and the serrated pattern was often retained in invasive carcinoma evolving from US-TSA (13, 14).
The incidence rate was defined as the number of new cases per population at risk in a given time period.
Statistical analysis. The non-parametric Wilcoxon test and the chi-squared test were performed. Statistical significance was defined as p<0.05.
Results
In 2008, we reviewed colorectal adenomas diagnosed during a 4-year period in Iceland (15): 4.3% (130/3037) were US-TSA. In that publication, ECF-TSA were separately recorded but reported together with villous adenoma/tubulovillous adenoma (TV/TVA). This was done for comparative studies with large series of CRAs from other countries in which only TAs, TVAs and VAs were included (15). It was assumed that the in those series, ECF-TSAs were incorporated with TVAs and VAs, as ECF-TSA also exhibits villous outgrowths.

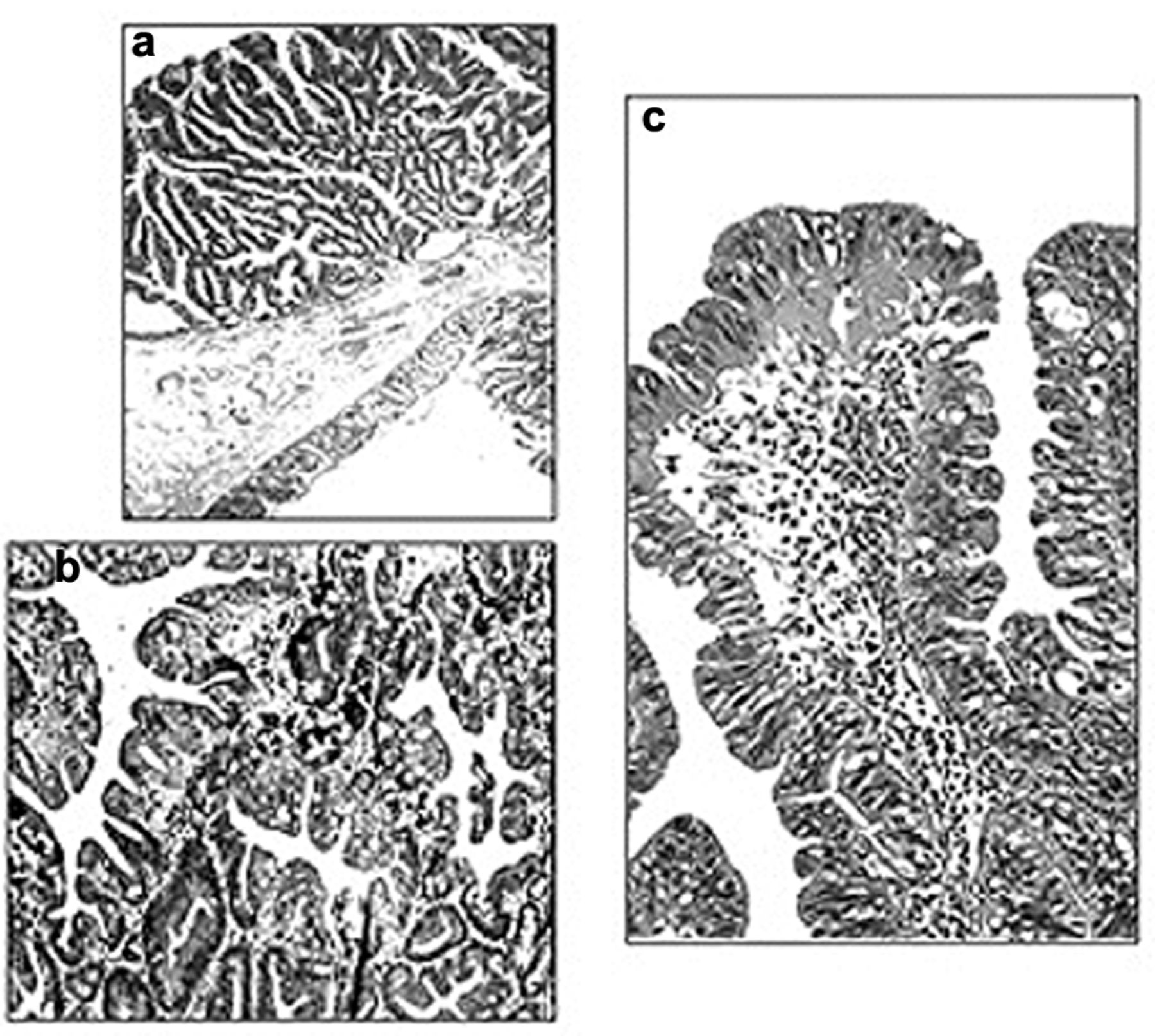
Traditional serrated adenoma with ectopic crypt formations (ECF-TSA phenotype). Note microtubules distributed sideways and within villous-like outgrowths (Hematoxylin and eosin; a and b: ×10, c and d: ×20).
The present updated classification of CRAs in Iceland consists of 2,022 TA, 707 TVA/VA, 130 US-TSA and 178 ECF-TSA. The results in Table I show that ECF-TSA accounted for 5.9% (178/3037) of all CRAs investigated. Of these, LGD was found in 48.9% (87/178), HGD in 43.3% (77/178), and invasive carcinoma in 7.9% (14/178). US-TSA accounted for 4.3% (130/3037) of all CRAs investigated. Of these, LGD was found in 49.2% (64/130), HGD in 59.2% (77/130), and invasive carcinoma in 7.7% (10/130).
Gender. Males accounted for 52.8% of the patients with ECF-TSA and US-TSA for 51.5%.
Age. Out of the patients with ECF-TSA, 74.1% were 60 years or older, as well as 76.2% of those with US-TSA. Patients with advanced ECF-TSA were younger than those with US-TSA (p<0.05). Invasive carcinoma was more frequently found in younger patients with a ECF-TSA than in those with US-TSA, but the difference was non-significant (p<0.7).
Localization. The localization was retrieved from the records in 177 out of the 178 ECF-TSA. The majority of the ECF-TSA [127/177 (71.8%)] were located in the left colorectum and the remaining 28.2% (50/177) in the right colon (up to the splenic flexure). The rectum accounted for 55.1% (70/127) of the left-sided ECF-TSAs. On the other hand, only 40.0% (52/130) of the US-TSAs were located in the left colon and rectum, and the majority (78/130, 60.0%) in the right colon (up to the splenic flexure). The frequency of left-sided adenomas was significantly higher for ECF-TSA than for US-TSA (p<0.05).
Traditional serrated adenoma with dysplastic crypts lining unlocked serrated crypts (US-TSA phenotype) (Hematoxylin and eosin; a: ×4, b and c: ×10).
Discussion
In the present nationwide survey in Iceland, two predominant histological phenotypes of colorectal TSA were found: ECF-TSA and US-TSA. This is in accordance with the findings of Kim et al. showing that only 79% of TSAs had ECFs (16), with those of Wiland et al. showing that only 62% of the TSAs had ECFs (17), and those of O'Brien et al. who postulated that ECFs were related to villous morphology/architecture rather than to serrated (18). Hence, in agreement with those authors, we found that the presence of ECF is not a requirement for defining TSA.
Males accounted for 52.8% of the patients with ECF-TSA, suggesting that these lesions were not influenced by endocrine factors inherent to the gender of the patients. On the other hand, ECF-TSAs and US-TSAs were age-dependent neoplasias as the majority of the patients (74.1% and 76.2%, respectively) were 60 years of age or older. When the age of the patients with advanced TSA was stratified, patients with ECF-TSA were significantly younger than those with US-TSA. A similar trend was found for patients with ECF-TSA carying an invasive carcinoma. Another difference was that ECF-TSAs were predominantly left-sided, whereas US-TSAs were predominantly right-sided. Histochemical staining showed that the cells that lined the microtubules in ECF-TSAs were sialomucin-secreting dysplastic goblet cells (Figure 3). On the other hand, the dysplastic cells that lined the unlocked serrations in US-TSA showed either no sialomucin-secretion or occasional sialomucin-secretion in the luminal aspect of the cytoplasm in some dysplastic cells (Figure 4). Ki-67 immunostains have shown that cell proliferation initially occurred in the dysplastic microtubules in ECF-TSA whereas it initially occurred at the base of the dysplastic crypts in US-TSA with unlocked serrations (10, 12).

Traditional serrated adenoma with ectopic crypt formations (ECF-TSA phenotype) showing alcian-blue positive mucin-producing dysplastic goblet cells (Periodic acid–Schiff-Alcian-blue pH 2.5; a: ×4, b: ×10, and c: ×20).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Traditional serrated adenoma with unlocked serrated crypts (US-TSA phenotype). Note absence of Alcian-blue staining in the upper left panel (a), and occasional Alcian-blue positive mucin-producing dysplastic cells in the luminal aspect of the cytoplasm in some dysplastic cells in b, c and d. (Periodic acid–Schiff-Alcian-blue pH 2.5; a and b: ×10, c and d: ×20).
The frequency [n (%)] of tubular adenomas (TA), tubulo-villous and villous adenomas (TVA/VA) and of traditional serrated adenomas (TSA), either with ectopic crypt formations (ECF-TSA), or with unlocked serrations (US-TSA), in Iceland (2003-2006).
Comparison of the incidence rate of traditional serrated adenomas (TSA), either with ectopic crypt formations (ECF-TSA) or with unlocked serrations (US-TSA), between Iceland, Florence, and Stockholm. Incidence rate is defined as the number of new cases per population at risk in a given time period. Note: The entire population in Iceland, and the catchment population areas of the Florence University Hospital, Italy, and the Karolinska University Hospital, Stockholm, Sweden, are about 300,000 inhabitants each.
The reported frequency of TSA in the literature has been based on the presence of ECF and of unlocked serrations. In this work, we applied the predominant histological phenotype. Importantly, nine TSAs having ECF structures were not included in the Tables as such, but as US-TSA, since the latter was the predominant histological phenotype.
In 1997, we reported four serrated adenomas exhibiting dysplastic microtubules arranged in a sequential fashion within and lengthwise villous-like outgrowths; they were called villomicroglandular adenomas (19). In the 2000 version of the World Health Organization (WHO) Classification of Tumors of the Digestive System, villomicroglandular adenomas were re-baptized as microtubular adenomas (20). In the 2010 version of the WHO, microtubular adenomas were called TSA with ECF (21).
In Iceland, the entire population is 300,000 inhabitants. Coincidentally, the catchment population-size of the University Hospital in Florence (9), and of the Karolinska University Hospital, Stockholm (10) is about 300,000 inhabitants. Similarities in size populations and the fact that the same observer (CAR) reviewed the materials in the three surveys would endorse a bona fide comparison between the frequencies of TSA in these three disparate geographical regions. In Iceland, ECF-TSA accounted for 5.9% and US-TSA for 4.3%, in Stockholm 0.9% (27/3135) were ECF-TSA, and 6% (202/3135) US-TSA (10, 11), and in Florence, 0.9% (14/1552) were ECF-TSA and 7% (102/1552) were US-TSA (10). The frequency of ECF-TSA in Iceland was significantly higher than in Stockholm and in Florence (p<0.05). Table II also shows that the frequency of ECF-TSA/year was significantly higher in Iceland than in Stockholm and Florence (p<0.05). Moreover, the incidence rate/year of ECF-TSA was significantly higher in Iceland than in Stockholm and in Florence (p<0.05) (Tabel I). However, the frequency of ECF-TSA with invasive carcinoma was significantly higher (p<0.05) in Iceland and in Stockholm (7.8% and 11.8%, respectively) than in Italy (0.7%), whereas the frequency of invasive carcinoma in US-TSA was similarly high in Iceland and in Italy (7.8% and 6.9%, respectively). The cause(s) for the fastidious propensity of TSAs (ECF and US) to progress to invasive carcinoma in different geographical locations remains elusive. It should be mentioned that not only the severity of cellular dysplasia but also the ornamental configurations might play a particular role in the aggressiviness of TSAs. This assumption is not surprising, considering that it has repeatedly been demonstrated that the presence of villous configurations in CRA increases the risk of progression to invasive carcinoma (22-24).
In conclusion, due to distinctive morphological, histochemical and immunohistochemical attributes, a predominant left-sided location and the absence of unlocked serrations, ECF-TSA in Iceland seems to be a distinctive colorectal histological phenotype, at variance with US-TSA. More importantly, ECF-TSA and US-TSA are lesions prone to evolve into invasive carcinoma. More epidemiological studies and molecular research (25) will be necessary to unravel the riddle of the high frequency and aggressive behavior of these lesions in Iceland.
Acknowledgements
Thanks are due to Anna Lara Axelsottir, Sigridur Sveindottir, Sigrún Edda Sigurjonsdottir at Landspitali, University Hospital, Reykjavik, Thuridur Nikulasdottir and Thuridur Unnarsdottir at the Reykjavik Private Clinic, Hildur Halldórdottir at District Hospital Akureyri, for invaluable laboratory help and to Mrs Inger Kristina Rubio for double-checking data and secretarial work.
This study was supported by a grant from the Karolinska University Hospital, Stockholm. Sweden.
- Received April 5, 2015.
- Revision received April 5, 2015.
- Accepted May 5, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved