

Abstract
Background: Epidermal growth factor receptor (EGFR) analysis is the first molecular test introduced in the routine care of patients with non-small cell lung cancer (NSCLC). In the present study, we describe the prevalence of EGFR mutations and the adherence to testing and treatment guidelines in a population-based Swedish NSCLC cohort. Materials and Methods: Patients with NSCLC analyzed for EGFR mutations were identified and their characteristics and survival data were retrieved. We compared the study cohort to a matched lung cancer population. Results: The EGFR mutation frequency was 10%. Mutations were enriched in women and in adenocarcinoma cases. Out of patients with advanced-stage NSCLC with non-squamous histology, only 49% were referred for EGFR analysis. Out of the patients with EGFR mutation and advanced disease, only 38% received EGFR-tyrosine kinase inhibitor (TKI) in first-line therapy. Conclusion: The EGFR-mutated NSCLC population studied is similar to other Western populations. Surprisingly, a large proportion of patients were not referred for EGFR analysis. Out of the patients with EGFR mutation, fewer than 40% received EGFR-TKI as first-line treatment. Our results highlight the need for follow-up of treatment and diagnostic algorithms in routine healthcare.
- Non-small cell lung cancer
- EGFR
- mutation
- outcome
- population
- prevalence
With an estimation of approximately 1.6 million deaths and 1.8 million new cases per year, lung cancer is the leading cause of cancer-related death and represents the most common cancer type worldwide (1). Lung cancer is traditionally divided into small-cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC) that represents 80-85% of all lung cancer cases (2). NCSLC is a highly heterogeneous group consisting of three main histological types based on small biopsies: squamous cell carcinoma (SqCC), adenocarcinoma (AdC) and NSCLC-not otherwise specified (NSCLC-NOS) (3). In 1995, chemotherapy was shown to prolong survival compared to best supportive care as demonstrated in a meta-analysis (4). Treatment consisting of a platinum drug in combination with a third-generation cytotoxic drug became standard and was used to treat all types of NSCLC (5). However, since 2008, when Scagliotti et al. published a phase III study showing a marked difference in survival in response to chemotherapy treatment between patients with SqCC and those with non-SqCC, the focus on histology started to increase (6).
The treatment paradigm for NSCLC is rapidly changing from ‘one size fits all’ towards personalized treatment with targeted-therapies and histology-based decisions regarding choice of chemotherapy. It is likely that the increasing use of molecular pathology will help transform advanced NSCLC from a deadly disease to a malignancy where substantial regression and stable disease can be maintained for a long time (7-9). In order to maximize future patient outcomes, we need to learn from the implementation process of present biomarker assays for therapy decisions. In this respect, treatment with epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) in EGFR-mutated lung cancer serves as a model of the integrated clinical use of tumor histopathology, molecular genetic analysis, and drugs targeting an activated oncogene (10, 11).
The first EGFR-TKI drug, erlotinib, received fast-track Food and Drug Administration (FDA) approval in 2002 as the first targeted-drug to be used in lung cancer, and gefitinib was approved by the FDA as a second-line treatment in 2003 (12, 13). In Sweden, EGFR mutation analysis for NSCLC in clinical practice was started during 2009, when gefitinib was approved by the European Medicines Agency for first-line treatment of EGFR-mutated NSCLC (14). During 2010-2012, the clinical evidence, as well as selection criteria for EGFR mutation analysis, developed gradually. The first Swedish guideline regarding EGFR mutation testing in NSCLC was published in 2010 as regional guidelines recommending EGFR analysis for all patients with non-squamous NSCLC where medical treatment was an option. In 2011, the Swedish National Board of Health and Welfare published national guidelines adopting the recommendation of EGFR analysis for all patients with non-squamous NSCLC (15). Over the past years, discussions have been intense about how EGFR testing should be performed, on which patients, and how EGFR-TKI treatment should be administered. But very few hard data have been published, from a population-based perspective, on which patients were actually tested for EGFR mutations, whether the potential selection could be motivated by medical reasons, and how EGFR-TKI treatment is prescribed outside clinical studies.
The aim of the present study was to describe the frequency and spectrum of EGFR mutations in routine clinical practice in a defined Swedish patient cohort during 2010-2012. We also aimed to investigate how the EGFR analysis was implemented with regard to selection bias due to clinical, histological and sample parameters, and to follow-up the treatment of patients with EGFR mutations.
Materials and Methods
Patients. Patients with NSCLC that were tested for EGFR mutations during 2010-2012 were identified at the Unit of Molecular Pathology, Department of Pathology, Uppsala University Hospital. Only patients from the Uppsala Health Care Region (i.e. hospitals in Gävle, Falun, Västerås, Eskilstuna and Uppsala) were included in the study. Tumour histology and immunohistochemistry results (3) were reviewed and the cases were grouped as AdC, SqCC or NSCLC-NOS. Clinical data were collected from the National Lung Cancer Registry (NLCR), a clinical audit and research database that prospectively compiles information on diagnostic procedures, tumour histology, stage, performance status (PS) according to the World Health Organisation (WHO), smoking history, treatment and survival for all patients diagnosed with lung cancer in Sweden. In the analysis, the cases referred for EGFR analysis were compared to the total source population, i.e. all patients diagnosed with NSCLC at the same hospitals during the same time period.
To study how a positive EGFR mutation test changed the course of treatment with regard to EGFR-TKI treatment, we performed a follow-up of the medical charts at the respective hospitals. Information on treatment given in first-, second- and third-line therapy, tumour stage and time from diagnosis to death or last follow-up was collected. The study was reviewed and approved by a central ethic review board (Uppsala, Sweden, reference no. 2012/216).
Mutation analysis. The tumour histology and tumour cell content (viable tumour cells/total number of viable cells) were assessed on a routine hematoxylin and eosin stained slide. Three to ten sections of 10 μm, depending on biopsy size, were cut from the corresponding formalin-fixed paraffin-embedded (FFPE) tissue block for DNA extraction using the QIAamp DNA Mini kit (Qiagen, Hilden, Germany). If needed, manual microdissection was performed to enrich for tumour cells. From cytological samples, FFPE cell blocks were processed in a similar way, alternatively cells were scraped off air-dried smears. Hot-spot mutations in EGFR exon 18-21 were analysed by allele-specific Polymerase Chain Reaction (PCR) (Therascreen EGFR29 kit (DxS, Manchester, UK); and Therascreen EGFR RGQ PCR Kit (Qiagen, Hilden, Germany) and/or by PCR amplification and sequencing of EGFR exon 18-21 by standard dideoxy (Sanger) sequencing as a backup method (BigDye Terminator v1.1 and 3130×l Genetic Analyser; Applied Biosystems, Foster City, CA, USA). Detailed protocols and primer designs are available on request.
Statistics. Patient characteristics at diagnosis are presented using standard descriptive statistics. Overall survival was analysed with Kaplan–Meier product-limit estimates. Survival curves were compared using the log-rank test. Differences in observed frequencies were analysed using chi-square test. The follow-up time was calculated from the date of diagnosis to death or last follow-up (censored) until the end of 2013. Age was defined as age at diagnosis.
Results
EGFR-analyzed cohort and source population of NSCLC. The baseline characteristics of the EGFR-analyzed NSCLC cohort and the source population of all patients with NSCLC diagnosed in five regional Hospitals during 2010-2012 are shown in Table I. Out of the total number of EGFR-analyzed cases (n=653) 82% were AdC, 5.5% were SqCC, 12% were NSCLC-NOS; for 0.7% the histology was other than NSCLC or unknown. In the corresponding NSCLC population (n=1646), the reported tumor histology was 45% AdC, 21% SqCC, 18% NSCLC-NOS and 16% non-NSCLC, respectively. The cohort that underwent EGFR analysis was slightly younger, was more often never-smokers and had more often a better PS (i.e. 0-1) when compared to the total population of NSCLC in the registry. A trend towards enrichment of female gender was found in the EGFR-analyzed cohort. In total, 653 out of 1,646 cases (40%) of the entire NSCLC source population were subjected to an EGFR mutation test. The cohort of patients undergoing EGFR analysis fulfilling current guidelines (non-SqCC NSCLC) was 612, including early stages (IA-IIIA). The corresponding total number of cases in the registry was 1,035 during the study period in referring hospitals, resulting in an EGFR analysis coverage of 59%. The frequency of EGFR analysis with regard to histology was 72% and 26% for AdC and NSCLC-NOS, respectively.
Descriptive data showing the whole cohort tested for epidermal growth factor receptor (EGFR) mutation 2010-2012 and the corresponding cohort in the national lung cancer registry during the same time period.
Comparison between patients with stage IIIB-IV non-squamous non-small cell lung cancer that were and were not analysed for epidermal growth factor receptor (EGFR) mutation during the years 2011-2012
In order to evaluate the adoption of national guidelines published in 2010 regarding EGFR mutation analysis, we decided to limit the analysis to non-SqCC NSCLC stage IIIB-IV cases diagnosed in the five Hospitals during 2011-2012 (Table II). Out of these 433 patients, 213 were subjected to EGFR mutation analysis, i.e. 49%. In this comparison, age (slightly younger), histology (enrichment of AdC) and PS (enrichment of PS 0-1) differed significantly between the tested and non-tested patients. A trend was seen with regard to smoking status (p=0.07) of enrichment of never-smokers. However, even considering some degree of ‘positive’ clinical selection, the data cannot explain why ‘only’ 184 out of 319 patients with AdC (58%), 31 out of 56 never-smokers (55%), or 107 out of 168 patients with PS 0-1 (64%) were tested. Thus on the whole, having an EGFR mutation analysis performed or not for an EGFR-TKI therapy decision was not explained by clinical registry parameters.
EGFR mutation and clinical characteristics. The samples used for EGFR mutation analysis were retrieved by core needle biopsy in 46% of the cases, bronchoscopic biopsy in 29%, surgical specimens in 22%, cytology in 0.6% and an unknown method in 1.6%. Out of the performed analyzes, 90% were successful. For 2.8% of the samples, no reliable result was obtained. The remaining 7% of the samples were successfully analysed (with a negative result for mutation) but with some degree of uncertainty due to a borderline tumor cell content. When comparing core needle biopsy and bronchoscopic biopsy, the accuracy of the methods were similar, with an average tumor cell fraction of 29% vs. 28% and inconclusive analysis in 3.9% and 2.6%, respectively. The overall mean tumor cell fraction of the samples was 30% (range=5-85%).

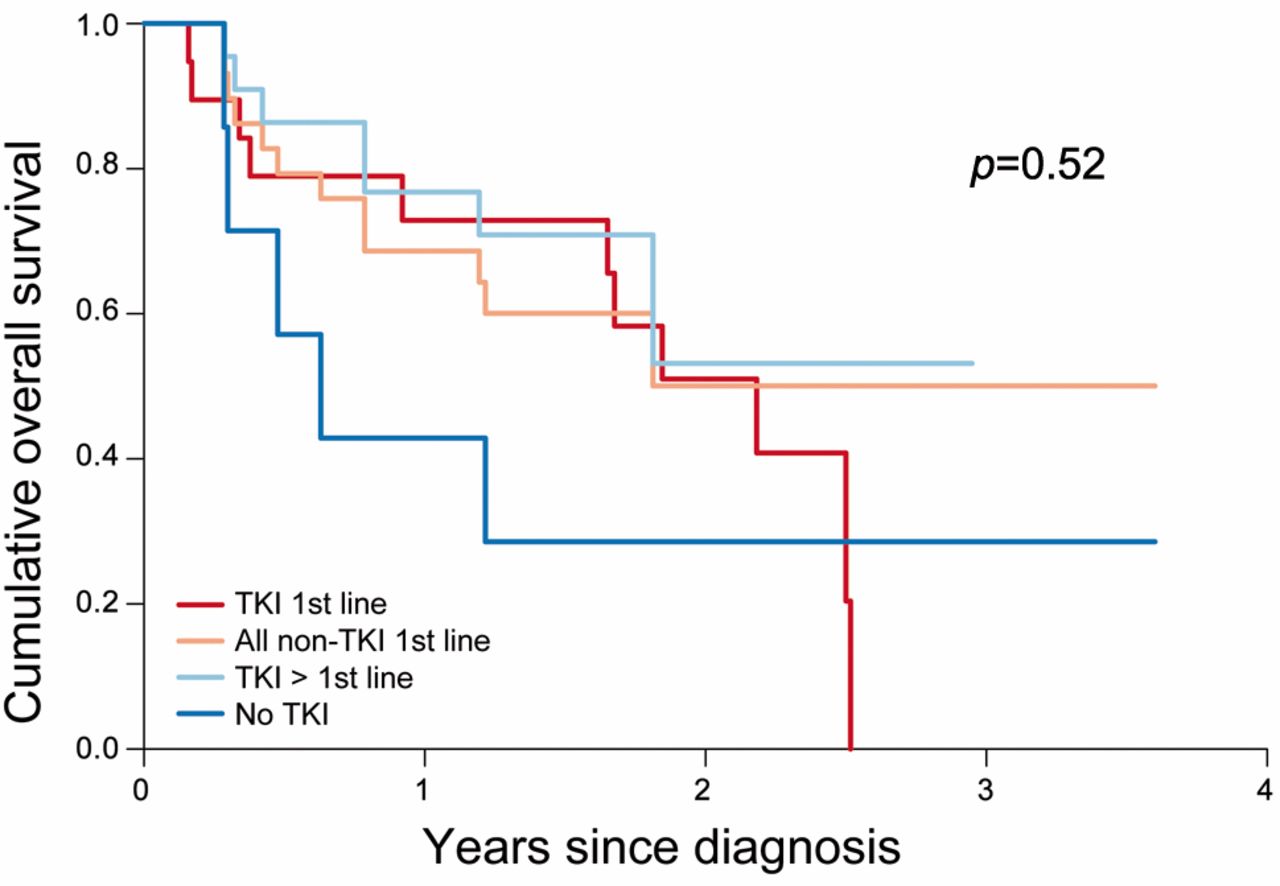
Cumulative overall survival of patients according to therapy: comparison of patients receiving EGFR-tyrosine kinase inhibitors in first-line therapy, in second- or later lines, all patients not receiving first-line tyrosine kinase inhibitors, and patients only receiving chemotherapy. (p=0.52).
The frequency of EGFR mutations in the analyzed cohort was 10.3% (65 out of 634, see Table III). As in other reported cohorts, the bulk of mutations represented deletions in exon 19 (n=37) and point mutations in codon 858 in exon 21 (n=17). A few additional mutations were found in exon 18 (G719X) (n=3), exon 20 insertions (n=3), exon 21 (L861Q) (n=4), and one double mutation (G719X and S768I). Of the EGFR-mutated cases, 94% (n=61) were found in AdC, 4.6% in NSCLC-NOS (n=3), and in one case, the histology was not assessable. The mutation frequency was 11.5% (61 in 530) in AdC and 3.9% (3 in 65) in NSCLC-NOS (Table III). EGFR mutations were considerably more common in women (15%, 52 out of 349) than in men (4.6%, 13 out of 285). A significant positive association between EGFR mutation and smoking status was present, however, no trend was seen with regard to stage or PS.
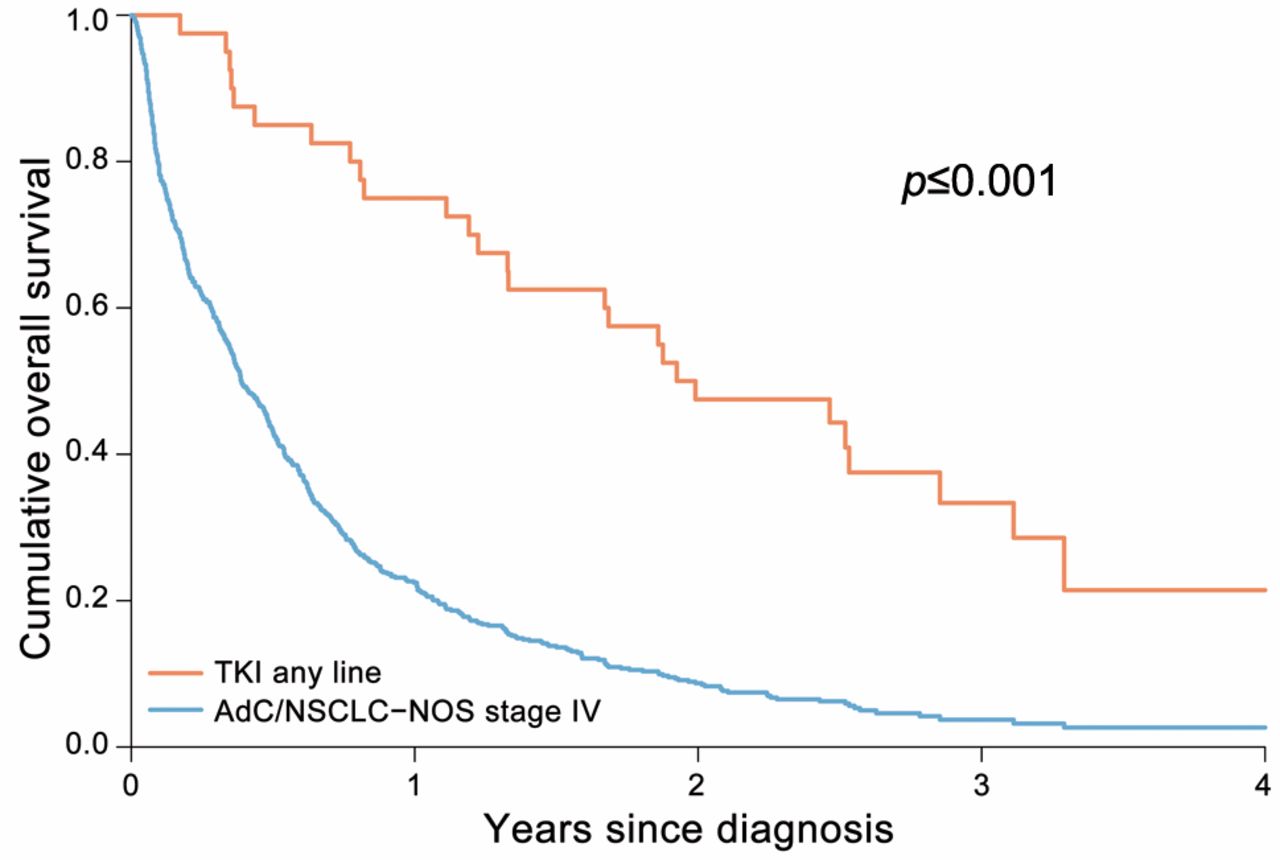
EGFR-TKI therapy. Of the EGFR-mutated cases, 50 were potentially eligible for first-line EGFR-TKI treatment (i.e. diagnosed with advanced-stage disease); 38% received first-line EGFR-TKI, 46% received EGFR-TKI in second or later lines, and 16% had not received EGFR-TKI at the time of follow-up. The overall survival did not differ significantly (p=0.52) between the groups that received EGFR-TKI in first-line, later lines, any line or had not received EGFR-TKI at the time of follow-up (Figure 1). A highly significant difference (p≤0.001) in survival was present for patients treated with EGFR-TKI when compared to all patients with stage IV non-SqCC NSCLC in the registry (Figure 2).

{kind=link}
{kind=link}
Cumulative overall survival of patients according to therapy: comparison of patients receiving EGFR-tyrosine kinase inhibitors in any line and the overall outcome for patients with stage IV disease at corresponding hospitals during the same time period in National Lung Cancer Registry.
Discussion
In the first follow-up on a Swedish NSCLC cohort, we report an EGFR mutation frequency of 10% in the tested NSCLC population. Our data are in line, although on the lower side, with previous reports from studies in other Western countries (16-21). From a northern European perspective, our mutation rates are comparable to a Norwegian cohort of surgical specimens (7.5%) (17), a German cohort tested in clinical routine practice (9.8%) (22), and a Danish cohort covering an unselected NSCLC population including all SqCC cases (5.4%) (23). As in these studies, we found that EGFR mutations were enriched in AdC (11.5%) compared to the NSCLC-NOS sub-group (4.6%) and were more common in women (15%) than in men (4.6%). Our data show an association between EGFR mutation and smoking status. No association was seen with regard to stage or PS in relation to EGFR mutation status.
To our knowledge, this is the first study to evaluate the coverage and selection mechanisms for EGFR analysis, in a defined population-based NSCLC patient material. We show that selection mechanisms limited access to a proper diagnostic workup for many patients, and for particular sub-groups of patients. Approximately 40% of the source population of NSCLC in the covered healthcare region was subjected to EGFR testing, and as expected, there was a strong selection with regard to tumor histology, with testing coverage of 72% in the AdC sub-group. In the NSCLC-NOS sub-group, the coverage was much lower, 26%. This can be partly explained by the diagnostic confusion on how to define AdC, SqCC and the NOS sub-groups based on small tumor biopsies. Even though previously reported frequencies of EGFR mutation in patients with NSCLC-NOS are lower than for AdC (16, 19), it is probable that patients with EGFR mutation in this group have been missed due to lack of adequate pathology guidelines. This highlights the importance of the revised lung adenocarcinoma classification published in 2011 (3) that resolved this issue. A concern raised by this study is that despite guidelines recommending up-front EGFR analysis for all advanced stage non-SqCC cases, only 49% of these patients were tested during 2011-2012.
Descriptive data showing characteristics of the patients harbouring epidermal growth factor receptor (EGFR)-sensitizing mutations and the EGFR-analyzed cohort without EGFR-sensitizing mutations. Only cases with conclusive EGFR analysis are included in this table (n=634).
Apart from poor coverage of the NSCLC-NOS group, our data indicate that clinical selection criteria suggested in the early years of EGFR-targeted therapy to some degree affected referral for molecular pathology, i.e. bias for younger patients, those with better PS and never smokers. However, the overall poor coverage with regard to molecular testing needs to be explained by other parameters. The large proportion of surgical specimens, core needle and bronchoscopic biopsies in the tested patient cohort, and the small number of cytological specimens, indicate that the availability of tissue for genetic testing, rather than clinical selection bias, was a limiting factor for EGFR testing. Another likely factor for this shortfall is the lack of clear routines and check-lists for molecular testing in pathology and clinical departments in the early days of targeted therapy of lung cancer.
While it is widely recognized that the most effective treatment should be used in first-line therapy (24-26), due to the loss of patients to second-line, we report that only 38% of the patients with activating EGFR mutation received EGFR-TKI as first-line treatment. This may, to some extent, be explained by the absence of written guidelines during a part of the first year of the study. The survival of the patients receiving EGFR-TKI as first-line treatment did not differ significantly from that of the group of patients receiving EGFR-TKI in later lines. This finding might be explained by the fact that patients not receiving EGFR-TKI in first-line therapy had a relatively good PS enabling chemotherapy to be administered. The relatively modest side effects of EGFR-TKI could also have enabled patients with poor PS to undergo first-line treatment that would not have been administered if chemotherapy were the only option. While the number of patients harbouring EGFR mutations who had not received EGFR-TKI in any line at the time of follow-up was relatively low, it is likely that a significant difference in overall survival would be present with larger cohorts and more mature data. The TKI-treated population, however, when compared to the corresponding patients with non-SqCC NSCLC in the NLCR had a highly significant prolongation of survival, which is in line with previous reports addressing this issue (27).
We conclude that the EGFR mutation prevalence and patient demographics in Sweden are similar to previously published data for Western populations. Surprisingly, despite guidelines regarding molecular analysis, a large proportion of patients with non-squamous histology were not referred for EGFR analysis. Of the patients with NSCLC harbouring EGFR mutation, fewer than 40% received EGFR-TKI as first-line treatment. The current hope that targeted-drugs can fundamentally improve survival of patients with lung cancer can only be realized if molecular testing and linked treatments are implemented broadly to affected patients in routine healthcare. Our study stresses the importance of evaluating the coverage and selection mechanisms for predictive mutation analysis and how targeted-therapy is put into clinical practice in population-based NSCLC patient cohorts.
Acknowledgements
The Authors would like to thank Dr. Sofia Dettman, Dr. Anna Öjdahl Bodén and Dr. Pierre Sobrino for their help with collection of data. Funding for this study was generously granted by Professor John Naeslunds Stipendiefond and Uppsala County Association Against Heart and Lung Diseases.
Footnotes
This article is freely accessible online.
- Received April 7, 2015.
- Revision received May 4, 2015.
- Accepted May 6, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved