

Abstract
Background/Aim: Based on a radiobiological assumption of a low alpha/beta (α/β) ratio for prostate cancer, hypofractionated radiotherapy has increasingly gained traction in the clinical practice and recent guidelines have confirmed the non-inferiority of this approach. Nevertheless, the largest studies that have used hypofractionation so far, employed image-guided radiation therapy/intensity modulated radiation therapy (IGRT/IMRT) facilities that might have overcome the radiobiological advantages, which remain to be fully confirmed. The aim of this trial was to evaluate the feasibility of a hypofractionated schedule delivered with 3D-Conformal Radiotherapy to prostate and seminal vesicles in combination with hormonal therapy. Patients and Methods: The study included 97 consecutive patients with localized prostate cancer (PCa), irrespective of risk class, treated with a schedule of 62 Gy in 20 fractions over 5 weeks (4 fractions of 3.1 Gy each per week). According to National Comprehensive Cancer Network (NCCN) prognostic classification, patients were divided into a favourable group (19%), intermediate group (41%) and unfavourable group (40%). Early and late toxicities were scored using the radiation toxicity grading/European Organisation for Research and Treatment of Cancer (RTOG/EORTC) criteria. Additionally, the international prostate symptom index (IPSS) for benign prostate hypertrophy was used to evaluate obstructive urinary symptoms. Biochemical outcome was reported according to the Phoenix definition for biochemical failure. Hormonal therapy (HT) was administrated in 92% of patients. Results: After a median follow-up of 39 months (range=25-52), maximum ≥G2 late genitourinary (GU) and gastrointestinal (GI) toxicities occurred in 8% and 11% patients, respectively. The corresponding figures for acute toxicities were 24% and 15%. Patients with higher IPSS score before enrolment had significantly worse urinary function after treatment. Only 2% of patients died from PCa. Biochemical non-evidence of disease (bNED) was 83% for all patients. Conclusion: Our study confirms that 3D conformal radiotherapy (3DCRT) remains a safe and effective method to deliver a dose-escalated hypofractionated regimen for PCa patients in all risk classes with acceptable toxicity rates and optimal biochemical control.
- 3D conformal radiotherapy
- hypofractionated
- prostate cancer
- toxicity
Moderately hypofractionated radiotherapy (2.4 to 4 Gy per fraction over 4-6 weeks) has been tested in randomized trials reporting similar efficacy and toxicity as conventionally fractionated radiotherapy and considered an alternative to the standard approach in recent guidelines (National Comprehensive Cancer Network (NCCN), 2014) (1). Nevertheless, most of the contemporary series of hypofractionated radiotherapy employed image-guided intensity-modulated radiation therapy (IMRT), thus integrating to the biological advantages of the low alpha/beta (α/β) ratio of prostate cancer (PCa) the physical sparing obtained by an advanced form of radiotherapy. This leads to a better avoidance of the surrounding tissues in conjunction with a greater accuracy coming from the daily patient repositioning and correction for the inter- and intra-fraction organ movements. Therefore, it remains questionable whether the optimal results of the latest trials can be solely attributed to a different fractionated schedule or, rather, to the use of cutting-edge radiation techniques. Given the potential advantages in terms of patient convenience and health economics, we believed that hypofractionated radiotherapy (HFRT) for PCa should not represent a privilege of high-technology areas but can become part of the daily practice in those Centers still equipped with 3D conformal techniques.
In 2009, we initiated a phase II hypofractionation study for PCa consisting of 20 × 3.1 Gy=62 Gy delivered over a 5-week period at 4 fractions a week by means of 3D Conformal Radiotherapy (3DCRT) in combination with hormonal therapy. Primary end-points of the study were acute and late gastrointestinal (GI) and genitourinary (GU) toxicities.
Patients and Methods
Trial outline and eligibility. Patients with organ confined PCa in any risk class were enrolled in this phase II trial if the following selection criteria were met: histologically proven prostate adenocarcinoma; World Health Organization performance status ≤ 2; no evidence of distant metastases; no previous pelvic radiotherapy; no evidence of bowel inflammatory disease; no contraindications for hormonal therapy; no previous malignant tumours, apart from skin cancer (except melanoma) and previous transurethral resection of the prostate (TUR-P). All patients were divided according to NCCN (1) prognostic classification in 3 risk groups based on T stage, Gleason score and prostate-specific antigen (PSA): favourable group, 19 patients (19%); intermediate group, 40 patients (41%); and unfavourable group, 38 patients (40%). The Gleason score was ≤ 6 in 42% of patients, 7 in 30% and ≥ 8 in 28%. Hormonal therapy (HT) was prescribed in neo-adjuvant (88%), concomitant (90%) and adjuvant (86%) setting in the majority of patients (92%) for a total of ≤6 months (low-intermediate risk) or >6 months (high risk). The administration of a short-term HT in a substantial proportion of low risk patients aimed at obtaining a cytoreductive effect and lowering the incidence of GU toxicity in patients with obstructive symptoms at baseline. The choice of hormonal treatment was left to the physician and consisted in the administration of total androgenic deprivation in 61%, peripheral antiandrogens in 31% and gonadotropin-releasing hormone (GnRH) agonists in 8%. The Ethical Committee approved of the study protocol and written informed consent was required for participation Baseline tumour and patients' characteristics are summarized in Table I.
Radiotherapy plan. The simulation and treatment procedures used have been extensively reported in our previous work (2). Briefly, all patients received hypofractionated 3DCRT with external beam fraction dose of 310 cGy, 4 fractions/week until to a total dose of 62 Gy, corresponding to a total dose of 80 Gy (for an α/β estimate of 1.5 Gy) and 70 Gy (for an α/βestimate of 3 Gy) in a conventional schedule. The optimization was driven with the aim of delivering the prescribed dose to at least 95% of the planning target volume (PTV) according to International Commission on Radiation Units (ICRU) 50/62 guidelines. The following constraints were considered appropriate for organs-at-risk (OARs): the mean percentage of rectal volume receiving 38 Gy (rV38): <50%; the mean percentage of rectal volume receiving 54 Gy (rV54): <30%; the mean percentage of bladder receiving 38 Gy (vV38): <70%; the mean percentage of bladder volume receiving 54 Gy (vV54): <50%; Femoral heads: <42 Gy. The treatment was performed according to the Memorial Sloan Kettering Cancer Center (MSKCC)(3) set-up with a 3DCRT technique with photons from Linear Accelerator 6-15 MVs, 6 fields, Multileaf collimator (MLC). Daily portal imaging, matched with digitally reconstructed radiographs (DRRs), was used to check the accuracy of treatment set-up. A slight delay in the overall treatment time was obtained introducing a planned break on Wednesdays in order to avoid a weekly dose accumulation that might hamper mucosal recovery.
Tumor and patients' characteristcs.
End-points. The primary end-points of the study were acute and late GI and GU toxicities. Secondary end-points of the study were biochemical control, local control, distant control and disease-free survival. Patients were evaluated prior to radiation, weekly during treatment and at 3-months interval during the first 2 years of follow-up and every six months thereafter. GI and GU toxicity monitoring were assessed by radiation toxicity grading (RTOG) and European Organisation for Research and Treatment of Cancer (EORTC) score (4). Any increase in grade from baseline was considered toxicity related to treatment and calculated for the acute (90 days from the start of RT) and late phase (beyond 90 days). The international prostate symptom index (IPSS) for benign prostate hypertrophy was used to evaluate obstructive urinary symptoms (reported by patients) (5). Evaluation of incontinence was incorporated in the GU toxicity following the Common Criteria Toxicity (6). Assessment of tumor response relied upon biochemical recurrence and defined as the value of Nadir of PSA +2 according to the Phoenix criteria (7). Distant metastases (DM) were defined as radiological evidence of macroscopic disease in sites other than the prostate gland. Death of any cause was considered for overall survival (OS). Patients were censored at the time of the specific event.
Dose-volume characteristics.
Acute and late toxicities.
Results
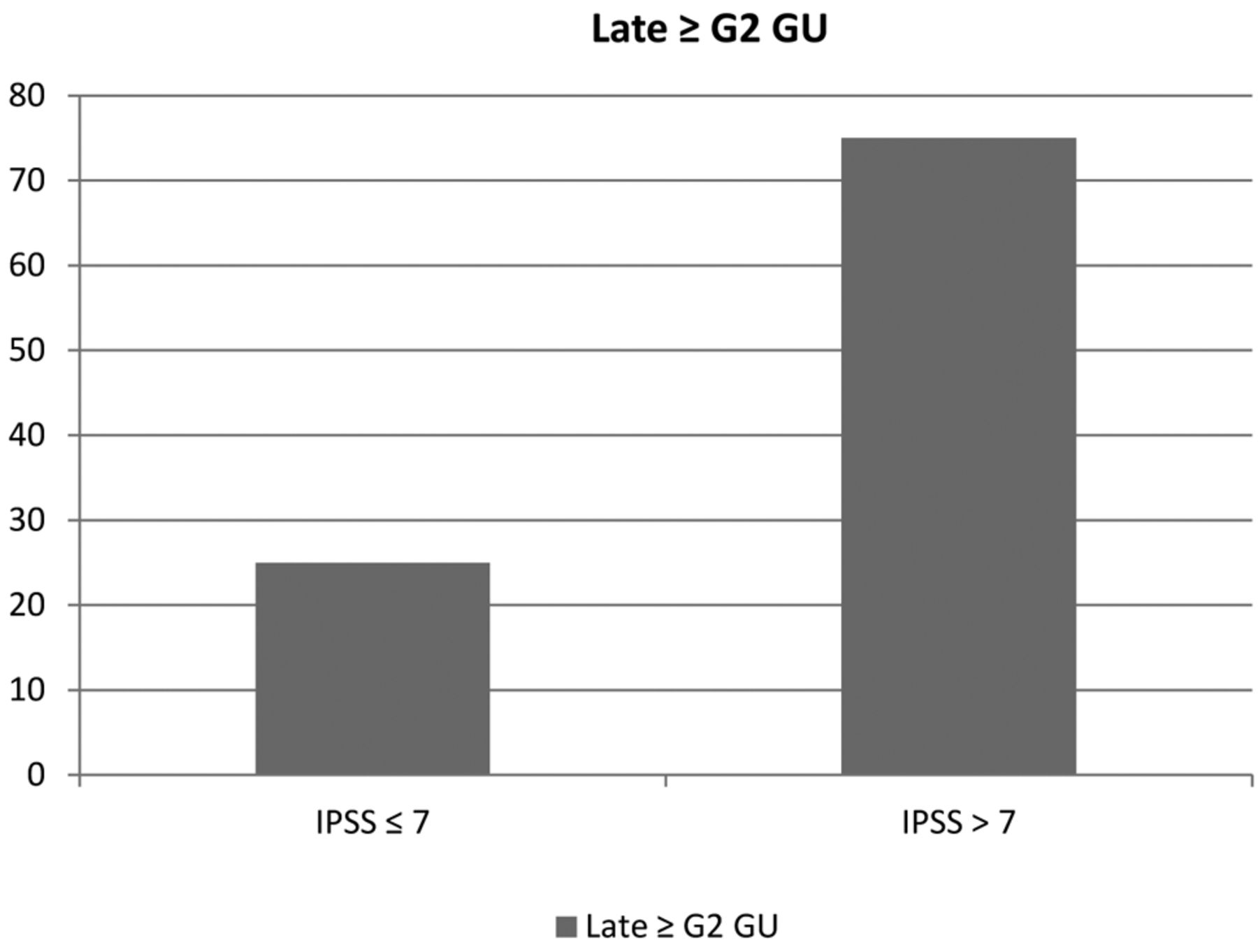
This report included 97 consecutive PCa patients treated between September 2009 and December 2011 with a median follow-up of 39 months (range=25-52). The median age was 72 years (range=53-82). All patients completed the treatment and underwent the scheduled follow-up, except two that were lost at last follow-up. The median overall treatment time was 38 days (range=30-49). Details on dose-volume characteristics are summarized in Table II. At the time of analysis the overall survival was 95%. The biochemical non-evidence of disease (bNED) was 83%. Among patients who are alive with progressive disease, evidence of distant metastases was found only in 4%. A summary of the analysis of patterns of disease progression is provided in Figure 1. No occurrence of Grade 4 acute and late toxicity was reported. Maximum detected acute ≥G2 GU and GI complications were 25% and 15%, respectively. Among the three patients who developed a G3 acute GU toxicity, two had previously undergone a TUR-P within the last 6 weeks before treatment. Maximum detected late ≥G2 GU and GI complications were 8% (G3=3%) and 11% (G3=1%), respectively. Acute and late GI and GU treatment-related toxicities are summarized in Table III. Evaluation of erectile dysfunction was impaired by the concomitant use of HT and, therefore, affordable conclusions are not allowed. No case of >G2 incontinence was documented. A number of patients, 18.5% (half of them being already incontinent before RT) and 3%, experienced a G1 and G2 incontinence, respectively. Patients with higher IPSS score before enrolment had significantly worse urinary function after treatment (Figure 2). Median initially IPSS of patients with G3 late toxicity was 17.

Analysis of patterns of disease progression.

{kind=link}
{kind=link}
Correlation between pretreatment IPSS and ≥G2 late-GU reactions. IPSS, international prostate symptom index; GU, genitourinary.
Randomized trials on hypofractionated RT for PCa.
Discussion
The path for hypofractionation for PCa has been long and dates back to the 1960's (8), in England, although it was basically sustained by economic matters rather than radiobiological issues. Still, in that pre-PSA era, patients treated with a short-course schedule of 36 Gy in 6 fractions to the prostate had optimal response in terms of OS and surprisingly low morbidity, taking into account that obsolete techniques were employed. Afterwards, hypofractionation was abandoned for many years. Since the end of the 1990s, dose–response analysis of prostate cancer patients treated both with external beam RT and brachytherapy has led to the assumption that the α/β ratio of PCa is lower than for most other tumors. In the last decade, values between 1 and 3 Gy have been proposed (9-17), far lower than the typical value ascribed to the adjacent OARs, such as rectum and bladder. Therefore, delivering the same equivalent 2-Gy dose (EQD2) to the prostate using a larger than conventional (2 Gy) fraction size would not affect late side-effects and would have a sparing effect on early-responding normal tissues. This has opened the way to the endorsement of a hypofractionated regimen for PCa to improve the therapeutic ratio. Indeed, fewer but larger than conventional fraction sizes for a lesser total dose make for two suitable different approaches in the clinical practice: i) normal tissue de-escalation of total dose, while keeping constant the predicted tumor control; ii) tumor dose escalation, maintaining constant the predicted normal tissues late effects (18). Meanwhile, tremendous advancements in treatment planning and delivery have pushed clinicians to implement it in the daily workflow (19-20). Therefore, despite such a strong radiobiological rationale, the majority of the latest clinical trials implementing hypofractionation have employed advanced radiation techniques, such as image-guided IMRT, thus making the potential benefits of hypofractionation less certain. Among the five published randomized trials (Table IV), two of them (21, 22) have actually used a 3D conformal technique but the total dose delivered was less than 76–80 Gy, now considered a standard-of-care, in both trials. Moreover, no attempt has been made to make the study arms isoeffective, likely due to the fact that they were designed and performed before the reports suggesting a low α/β for prostate cancer. Owing to these limitations, the results carried in these latter trials warrant a particular caution on their interpretation and cannot provide any conclusive evidence with regard to a potential role for hypofractionation in the contemporary era. Only one trial (23-24) adopted a 3D conformal technique and found no statistically significant differences between hypofractionation and conventional fractionation in the actuarial freedom from all types of failure, after a median follow-up of 70 months, in a selected population of high-risk PCa patients. As in the Italian trial, we used a methodology employing 3D rather than IMRT and adopted the same schedule, but including also low- and intermediate-risk PCa patients. In our experience, the benefit of a dose escalated-hypofractionated radiation course appears to span all risk categories: after a median follow-up of 39 months, biochemical control rates appear optimal (100%, 88% and 80% for low-, intermediate- and high-risk patients, respectively) and 83% of patients are alive without disease. Despite using a 3D conformal technique, the incidence of both late rectal and urinary complications ≥G2 was 11% and 8%, respectively, not exceeding the toxicity rates reported in the hypofractionated arms of randomized trials employing intensity modulated radiation therapy (25-26) and significantly lower than those reported in the experimental arm of the 3D conformal Phase III dose-escalation studies delivering an equivalent total dose in the range of 78-80 Gy at 2 Gy/fraction (27-29). In comparison with results from recent “high-tech” randomized trials (30-31), acute Grade ≥ 2 toxicity was higher but still acceptable and developed in 24% (GU) and 15% (GI) of 97 patients, respectively. It is likely that the 1-week prolongation of the overall treatment time planned in our schedule (20 fractions in5 weeks, 4 fractions/week) was not enough to allow for mucosa cell repopulation. However, recovery from this toxicity, mainly consisting in rectal tenesmus or dysuria, occurred quickly. Interestingly, as already documented in the randomized trial by Pollack et al. (26), also in our series, baseline IPSS score was significantly associated with ≥2 GU late reactions suggesting a potential increased risk of toxicity in patients with pretreatment-compromised urinary function. The present study has some limitations, mainly inherent to the length of follow-up that might not be long enough to address late toxicity (especially GU), as well as to draw conclusions on endpoints, such as PCa-specific or overall mortality, typically requiring more than a decade of patient monitoring (but that were not considered as primary endpoints in our analysis). Notwithstanding these biases, the strength of the present study is the fact that it is among the few (23-24) where a methodology employing 3D rather than IMRT has been used, which certainly looks more attractive in the context of expecting hypofractionation to radiobiologically improve the therapeutic ratio. Hence, cutting-edge techniques in radiotherapy that can take advantage of robust radiobiological bases and can be safely delivered on 3D conformal basis, should not be considered mandatory to pursue hypofractionation.
Conclusion
The present study confirms that HFRT is a viable treatment option for localized PCa with acceptable toxicity rates and optimal biochemical control. The clinical benefits of the dose escalated-hypofractionated approach used in our study should not be withheld from PCa patients treated in Centers where only 3D technology is available. Prospective trials in the developing countries, typically not yet equipped with advanced radiation technologies, are encouraged to confirm the efficacy of a similar schedule in this setting.
- Received February 5, 2015.
- Revision received February 12, 2015.
- Accepted February 16, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved