

Abstract
Background: Although secretory phospholipase A2 (sPLA2) has been shown to be involved in various biological processes, its specific roles in sub-types of cancer development remain to be elucidated. Materials and Methods: We examined the expression of sPLA2 group III (GIII) in 142 patients with colorectal cancer using immunohistochemistry, and its correlation with clinicopathological features and outcomes. In addition, we examined the co-expression of sPLA2GIII and sPLA2GX using serial tissue sections to clarify the roles of both proteins in colorectal carcinogenesis. Results: In 66 cases, diffuse staining of sPLA2GIII was seen; this was defined as the group with high expression. High expression was associated with a significantly higher rate of lymph node metastasis (p=0.02) and poorer survival (p=0.03) compared with low expression. Patients with low sPLA2GIII and high sPLA2GX expression had a significantly higher survival rate than those with high sPLA2GIII and low sPLA2GX expression (p=0.038). Conclusion: sPLA2GIII expression may be used as a risk factor for lymph node metastasis and a prognostic marker in colorectal cancer. In addition, sPLA2GIII and sPLA2GX may play opposing roles in colorectal carcinogenesis.
- Phospholipase A2
- colorectal cancer
- immunohistochemistry
- lymph node metastasis
Colorectal cancer (CRC) is the third most common cancer in men and the second most common cancer in women, and is responsible for approximately 610,000 deaths annually worldwide (1). Despite surgical resection and combined chemotherapy, approximately 20% of patients with CRC develop distant metastases (2). The identification of new prognostic markers for distant metastasis may lead to improved treatment strategies and better outcomes for patients.
Phospholipase A2 (PLA2) is a key regulatory enzyme in arachidonic acid metabolism, catalyzing the hydrolysis of sn-2 fatty acyl ester bonds of phosphoglycerides, and releasing free fatty acids and lysophospholipids (3). One of the fatty acids released from membrane stores by PLA2 activity is arachidonic acid, a critical precursor in the biosynthesis of diverse eicosanoids, including prostaglandins, thromboxanes, and leukotrienes via the cyclo-oxygenase (COX)-1 and COX2 pathways (4). These lipid mediators are known to play a role in initiation and progression of CRC through cell proliferation, migration, and angiogenesis (5-9). In addition, COX2 modulates tumor growth by altering vascular endothelial growth factor expression (10). As a result, PLA2 is thought to play an important role in CRC. The PLA2 family of proteins includes calcium-independent PLA2 (iPLA2), high molecular weight cytosolic PLA2 (cPLA2), and low-molecular weight secretory PLA2 (sPLA2). sPLA2 proteins are calcium-dependent, secreted enzymes, containing a His/Asp catalytic dyad. To date, 11 sPLA2s (IB, IIA, IIC, IID, IIE, IIF, III, V, X, XIIA, and XIIB) have been identified in mammals (11-13).
Recently, various physiological functions of sPLA2s have been reported (14-27). The role of sPLA2GIII has been examined in several types of cancer (28-35). In stage II CRC, the expression of sPLA2GIIA was reported to be significantly correlated with disease recurrence (36). In addition, we demonstrated that the expression of sPLA2GX was inversely associated with hematogenous metastasis in CRC (37).
sPLA2GIII has the most unique structural property among mammalian sPLA2s, with prostaglandin E2-generating function in various cell types. sPLA2GIII is found in microvascular endothelial cells, and in uterine, breast, and colonic tumor cells (9). Therefore, sPLA2GIII was suggested as a good candidate biomarker for CRC (38). However, detailed analysis of sPLA2GIII expression has not been carried out thus far, and the association between sPLA2GIII expression and prognosis in CRC remains to be elucidated.
Clinicopathological features in colorectal cancer.
Therefore, in the present study, we analyzed the expression pattern of sPLA2GIII in CRC, and its correlation with clinicopathological factors and outcomes. Furthermore, we examined the co-expression of sPLA2GIII and sPLA2GX using immunohistochemical (IHC) analysis of serial tissue sections, and analyzed the roles of both proteins in CRC carcinogenesis.
Materials and Methods
Patients and samples. One hundred and forty-two patients with CRC who were treated with curative resection and lymph node dissection at the University of Tokyo Hospital between January 1991 and December 1993 were enrolled in this study. There were 85 men and 57 women, with an age range of 38-90 years (mean=62±11 years). Patients with inflammatory bowel disease and familial adenomatous polyposis were excluded from this study. None of the patients had received preoperative chemotherapy or radiation therapy. All clinical and histopathological data regarding the patients and their tumors were collected from medical records. Clinicopathological features were analyzed using the Union for International Cancer Control (UICC) histological criteria, as defined in the seventh edition of the TNM Classification of Malignant Tumors (39). Patient follow-up to evaluate tumor recurrence was carried out for 5 years; serum carcinoembryonic antigen level was measured every months, computed tomography (CT) was performed every 6 months, and colonoscopy was performed every 12 months. The median observation period was 9.2 years. Patient consent was obtained for the use of clinical samples for research purposes, and approval for the study was obtained from the Ethics Committee of the University of Tokyo Hospital (2391-(1)).
PLA2 group III expression in colorectal cancer by clinicopathological features.

Immunohistochemical staining for Phospholipase A2 Group III (PLA2GIII) in human colorectal cancer tissues. Diffuse (A) and focal (B) staining of tumor cells (original magnification, ×100).
Surgically resected specimens were immediately fixed in 10% buffered formalin, and cross-sections of entire cancerous lesions were embedded in paraffin. Conventional pathological diagnosis of the primary lesion and dissected lymph nodes was performed using hematoxylin and eosin (HE)-stained sections.
sPLA2GIII and sPLA2GX IHC staining. IHC analysis was carried out using three 3 μm serial sections. One of the three sections was used for HE staining, and the other sections were used for IHC analysis with antibodies to sPLA2GIII and sPLA2GX. Rabbit polyclonal antibodies to sPLA2GIII and sPLA2GX were generated by immunization of a rabbit with the appropriate polypeptide at the Tokyo Metropolitan Institute of Medical Science, Tokyo, Japan. The specificity and immunoreactivity of the antibodies were verified by immunoblotting with sPLA2-transfected cells (9). The sPLA2GIII and sPLA2GX antibodies were used at dilutions of 1:150 and 1:100, respectively.
The streptavidin-biotin immunoperoxidase method using a Histofine SAB-PO(R) kit was utilized (Nichirei, Tokyo, Japan). The sections were deparaffinized with xylene and dehydrated with 98% ethanol, placed in 0.01 M sodium citrate buffer (pH 6.0), and heated in an autoclave for 15 min. After washing twice in phosphate-buffered saline (PBS), endogenous peroxidase activity was inhibited by incubation with 0.3% hydrogen peroxide in methanol for 20 min. The sections were incubated with anti-sPLA2GIII and anti-sPLA2GX overnight at 4°C, and secondary biotinylated goat anti-rabbit immunoglobulin was applied after washing in PBS. Color development was carried out using diaminobenzidine solution. Sections were then lightly counterstained with a mixture of Mayer's and Lillie-Mayer's hematoxylin, and mounted. For negative controls, the antibody was replaced with PBS.
Evaluation of immunostaining. Staining was independently evaluated by two observers who had received training in pathological diagnosis (S.K. and M.H.), and who were blinded to the clinical findings. Discrepancies between their findings were resolved by discussion. To evaluate protein expression regardless of intensity, results were graded as follows: none, not detected; focal, focally expressed; and diffuse, diffusely expressed. In the statistical analysis, none and focal were considered to be low expression, and diffuse was considered to be high expression.
Statistical analysis. The statistical significance of differences was evaluated using the chi-square, Fisher's exact, or non-paired Student's t-test, as appropriate. Overall survival was analyzed using the Kaplan-Meier method and log-rank comparison test. All statistical calculations were carried out using JMP Pro 11.0.0 statistical software (SAS Institute, Cary, NJ, USA). An association was considered significant when the p-value was less than 0.05.
Results
sPLA2GIII and sPLA2GX expression. Clinical features of the 142 patients are shown in Table I. The staining patterns of sPLA2GIII and sPLA2GX in cancerous lesions are illustrated in Figure 1. The normal colonic mucosa adjacent to cancerous lesions was almost absent for sPLA2GIII, and ranged from none to weak for sPLA2GX. In the tumoral lesions, the expression of sPLA2GIII and sPLA2GX was predominantly observed in the cytoplasm of neoplastic cells, with enhanced staining intensity compared to the normal mucosa. The stromal tissue showed no sPLA2GIII or sPLA2GX expression. IHC analysis of sPLA2GIII expression revealed that 66 (46.5%), 61 (43.0%), and 15 (10.6%) tumors stained diffusely, focally, and negatively, respectively. Therefore, the numbers of tumors with low and high expression of sPLA2GIII were 76 (53.5%) and 66 (46.5%), respectively. On the contrary, analysis of sPLA2GX expression revealed that 90 (63.4%), 51 (35.9%), and 1 (0.7%) tumor showed diffuse, focal, and negative staining. The numbers of tumors with low and high sPLA2GX expression were 52 (36.6%) and 90 (63.4%), respectively.
PLA2 group III expression in left-sided colorectal cancer and clinicopathological features.
Correlation of sPLA2GIII and sPLA2GX expression with clinicopathological features. Age, sex, tumor size, tumor location, histological type, and tumor stage had no significant relationship with the expression of either sPLA2GIII or sPLA2GX. The high expression of sPLA2GIII was associated with a significantly higher rate of lymph node metastasis than the low expression (35/66 vs. 26/76; p=0.02) (Table II). When the cases were restricted to those with left-sided CRC (100 cases), high sPLA2GIII expression was also associated with a significantly higher rate of lymph node metastasis than low expression (24/48 vs. 16/52; p=0.049) (Table III). However, there was no correlation between sPLA2GIII expression and hematogenous metastasis or TNM stage. In contrast, statistical analysis revealed an inverse relationship between sPLA2GX expression and hematogenous metastasis (6/52 vs. 1/90; p=0.006), and TNM stage (p=0.03)(Table IV).
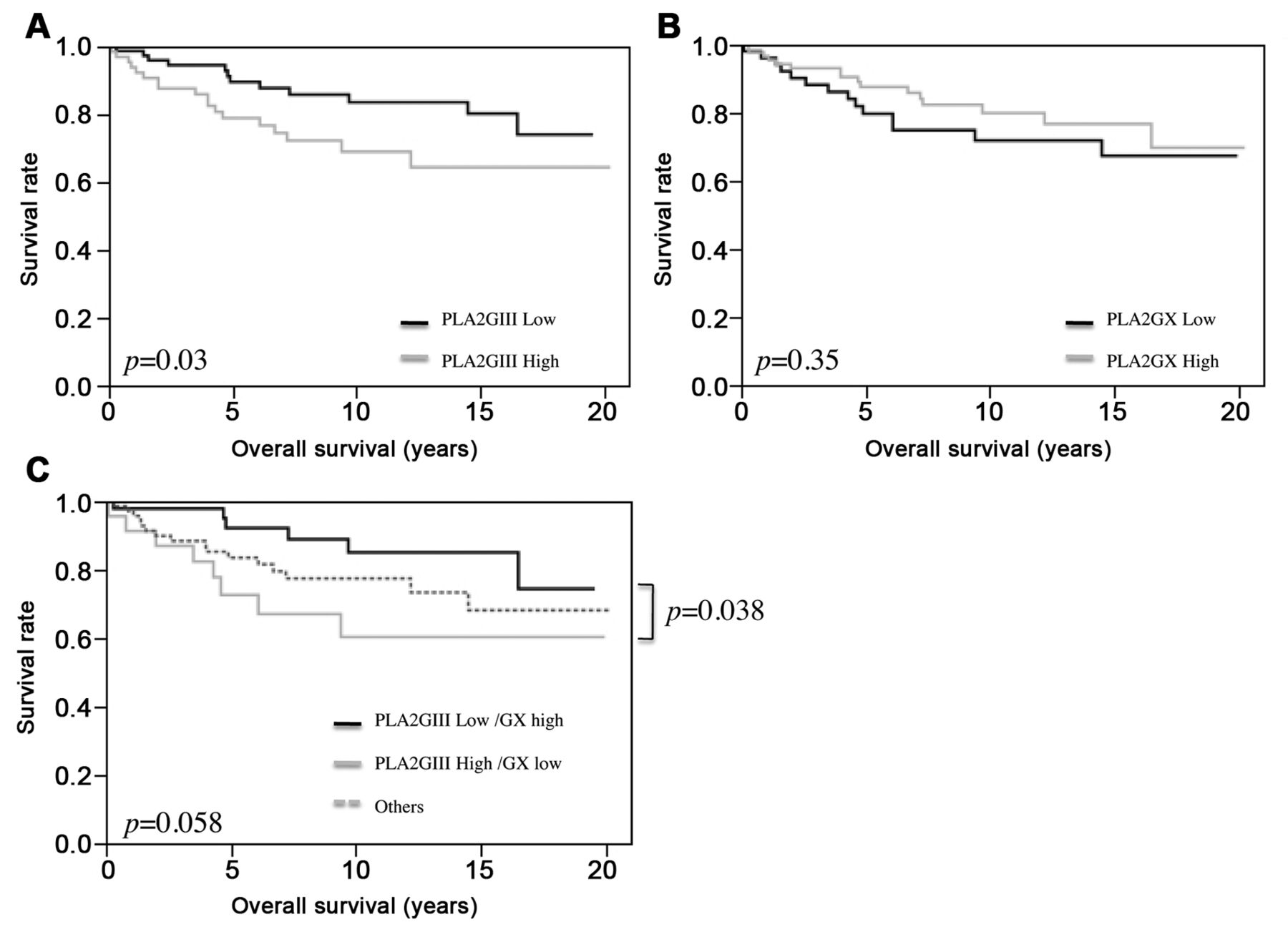
Analysis of overall survival associated with sPLA2GIII and sPLA2GX expression in colorectal cancer. Patients with low sPLA2GIII expression had a significantly higher overall survival rate than those with high expression (p=0.03) (Figure 2A), whereas no statistically significant association was found between sPLA2GX expression and patient outcome (p=0.35) (Figure 2B). To confirm the relevance of the opposing associations of the expression of the two proteins with prognosis, we divided the patients into three sub-groups according to their sPLA2GIII and sPLA2GX expression: sPLA2GIII high/sPLA2GX low, sPLA2GIII low/sPLA2GX high, and others including those with both high and those both low. The sub-group with sPLA2GIII low/sPLA2GX high expression tended to have a longer overall survival, but statistical significance was not reached (p=0.059) (Figure 2C). However, analysis of overall survival between the subgroup with low sPLA2GIII and high sPLA2GX expression and the subgroup with high sPLA2GIII and low sPLA2GX expression found that low sPLA2GIII and high sPLA2GX expression was associated with a significantly higher survival rate than the latter (p=0.038). Multivariate analysis of significant prognostic factors from univariate analysis was performed (Table V). On multivariate analysis, sPLA2GIII expression was not found to be an independent risk factor for overall survival.
PLA2 Group X overexpression in colorectal cancers and clinicopathological features

{kind=link}
{kind=link}
Association of PLA2GIII (A) and PLA2GX (B) expression alone and combined (C) in colorectal cancer in relation to overall survival (OS).
Discussion
In the present study, we demonstrated that high sPLA2GIII expression was significantly associated with lymph node metastasis and poorer prognosis in patients with CRC. Recently, the physiological functions of sPLA2s have been elucidated by examination of genetically manipulated mice (14, 15) with airway diseases (16, 17), arthritis (18), myocardial ischemia (19, 20), atherosclerosis (21), obesity (22), microbial defense (23), alopecia (24), reproduction (25), pain (26), and steatohepatitis (27). However, the roles of sPLA2, and in particular, those of their sub-types, have not been fully examined in tumor biology. To our knowledge, this is the first report of the prognostic significance of sPLA2GIII expression in patients with CRC.
We found that the normal mucosa adjacent to cancerous lesions was not stained using sPLA2GIII IHC, however, the cytoplasm of tumor cells was focally or diffusely stained. These results are in accordance with those of a previously reported study by Mounier et al., in which the expression of sPLA2GIII was significantly increased by up to 40-fold in tumoral tissue compared with that in normal mucosa at both the mRNA and protein levels (38). In addition, the high expression of sPLA2GIII that we found in 66 (46.5%) cases was significantly correlated with lymph node metastasis and poorer prognosis. High sPLA2 expression has been reported to correlate with prognosis in various types of cancer; overexpression of sPLA2GIIA was reported to be closely associated with malignant potential in breast and prostatic (31, 34), and Graff et al. showed that sPLA2GIIA expression was inversely related to 5-year survival in prostatic cancer (33). A significant difference was also found in both disease-free and disease-specific survival between patients with stage II CRC negative for sPLA2GIIA (longer survival) and those positive for sPLA2GIIA (36). These results are consistent with our findings of sPLA2GIII in CRC, suggesting that sPLA2GIII may play an important role in lymph node metastasis. In contrast, statistical analysis showed that sPLA2GX expression was inversely correlated with hematogenous metastasis and tumor grade. These results are consistent with those of our previous study (37). Therefore, in order to carry out additional analysis, we divided the patients into three sub-groups according to sPLA2GIII and sPLA2GX expression status, and evaluated the overall survival in the three groups. Although significant differences were not detected among the three subgroups, an analysis of two subgroups demonstrated that the subgroup with low sPLA2GIII and high sPLA2GX expression had a significantly higher survival rate than that with high sPLA2GIII and low sPLA2GX expression, indicating that the expressions of sPLA2GIII and sPLA2GX might have opposing associations with prognosis in CRC. To the best of our knowledge, this is the first study showing IHC expression of sPLA2GIII and sPLA2GX in CRC, and its association with tumor metastasis and poor prognosis.
Univariate and multivariate analyses of prognostic valuables for overall survival in colorectal cancer.
However, caution is required when interpreting our data. The study is limited by the small number of patients examined, and the retrospective nature of the study. Further prospective large-scale studies with long-term follow-up are needed.
In this study, we also evaluated the clinicopathological factors with regard to tumor location, by defining CRC as right- or left-sided. In CRC progression, two forms of genomic instability have been identified: microsatellite instability and chromosomal instability, and right- and left-sided colonic cancer exhibit different molecular profiles (40). Microsatellite instability and a methylator phenotype are prevalent in right-side tumors, and sporadic chromosomal instability tends to occur in left-side tumors (41, 42). In our previous study, we demonstrated that the rate of lymph node metastasis was significantly lower in left-sided CRC, correlating with sPLA2GX expression (37). In this study, we found no significant association of sPLA2GIII expression and tumor location. This result is consistent with the study by Mounier et al. that detected sPLA2G3 expression in both right- and left-sided adenocarcinoma (38). Additionally, in left-sided CRC, the rate of lymph node metastasis was significantly higher in the group with highs PLA2GIII expression than in the low-expression group (p=0.049), but no significant differences in overall survival were found (data not shown). These results are consistent with our suggestion that the expression of sPLA2GIII and sPLA2GX might have opposing associations with CRC prognosis.
In conclusion, we demonstrate that high sPLA2GIII expression significantly correlates with lymph node metastasis and a poorer prognosis. Our results also suggest that sPLA2GIII and sPLA2GX might play opposing roles in CRC carcinogenesis. Therefore, sPLA2GIII expression, in addition to sPLA2GX expression, might be useful prognostic markers for CRC, and further investigation of the role of sPLA2GIII expression in CRC is warranted.
- Received January 27, 2015.
- Revision received February 7, 2015.
- Accepted February 10, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved