

Abstract
Background/Aim: There exist various useful predictive models, such as the Cockcroft-Gault model, for estimating creatinine clearance (CLcr). However, the prediction of renal function is difficult in patients with cancer treated with cisplatin. Therefore, we attempted to construct a new model for predicting CLcr in such patients. Patients and Methods: Japanese patients with head and neck cancer who had received cisplatin-based chemotherapy were used as subjects. A multiple regression equation was constructed as a model for predicting CLcr values based on background and laboratory data. Results: A model for predicting CLcr, which included body surface area, serum creatinine and albumin, was constructed. The model exhibited good performance prior to cisplatin therapy. In addition, it performed better than previously reported models after cisplatin therapy. Conclusion: The predictive model constructed in the present study displayed excellent potential and was useful for estimating the renal function of patients treated with cisplatin therapy.
- Head and neck cancer
- serum albumin
- creatinine clearance
- renal function
- cisplatin
There exist a variety of methods for estimating renal function (1-3). Creatinine clearance (CLcr) based on 24-h urine collection is a reliable index of renal function. CLcr (ml/min) can be calculated from the serum creatinine concentration (Scr, mg/dl), the urinary creatinine concentration (Ucr, mg/dl), and the volume of urine (V, ml) using the following formula:
 However, 24 h CLcr is rarely used in the clinical setting because 24 h urine collection can have a negative impact on a patient's quality of life. Therefore, a variety of equations for predicting CLcr or the glomerular filtration rate (GFR) which are not based on urine collection have been devised (4-10).
However, 24 h CLcr is rarely used in the clinical setting because 24 h urine collection can have a negative impact on a patient's quality of life. Therefore, a variety of equations for predicting CLcr or the glomerular filtration rate (GFR) which are not based on urine collection have been devised (4-10).
Most patients with cancer receive chemotherapy or palliative care with opioids and non-steroidal anti-inflammatory drugs (11), and renal function is an important index for regulating the dosages of anticancer drugs and analgesics. Cisplatin is one of the most potent anticancer medications and is used to treat several types of solid tumors, such as head and neck cancer. Reduced renal function is a major adverse effect of cisplatin therapy. It is important to estimate the renal function of patients treated with cisplatin and to regulate the dose of cisplatin accordingly because cisplatin is eliminated into urine via the kidneys. However, our current knowledge regarding the estimation of renal function in patients receiving chemotherapy is limited. In a previous study, we showed that the CLcr values obtained using the predictive models that are currently employed in the clinical setting resulted in over- or underestimation in patients treated with cisplatin (12). Therefore, in the present study, we attempted to construct a model for predicting CLcr in patients treated with cisplatin.
Patients and Methods
Data acquisition. This study was approved by the Ethics Committee of the National Hospital Organization, Tokyo Medical Center, Japan (R10-071). A retrospective study was performed of the medical records of patients that received chemotherapy including cisplatin for head and neck cancer from March 2007 to June 2010 at the Department of Otorhinolaryngology, National Hospital Organization Tokyo Medical Center.
Patients' characteristics. Data that exhibited normal and non-normal distributions are expressed as the mean±S.D. and median (range) values, respectively.
Exclusion criteria. Patients for whom 24 h CLcr was not calculated based on the urine collection method or who exhibited Scr values of >2.4 mg/dl, 24 h CLcr values of >200 ml/min, or body mass index (BMI) values of >35 kg/m2 were excluded from all analyses. Patients for whom laboratory data for the period before or after cisplatin therapy were missing were excluded from the analysis of the changes in 24 h CLcr induced by the administration of cisplatin. In the analysis of the correlation between 24 h CLcr and predicted renal function, patients that lacked data for any of the parameters included in the various predictive equations were excluded.
Patients. Out of the 122 patients that were subjected to the aforementioned selection criteria, 50 were excluded according to the above criteria. The background data of the remaining 72 patients are shown in Table I. The first-line chemotherapy lasted for 21 to 50 days, except in three cases, in which it took 18, 89 and 141 days, respectively. The laboratory data used to estimate pre-cisplatin renal function was collected prior to the administration of cisplatin. The data used for these calculations were collected at ≤41 days prior to the administration of cisplatin. The estimation of post-cisplatin renal function was performed using laboratory data obtained ≤40 days after the end of the first-line chemotherapy.
Models for predicting creatinine clearance (CLcr, ml/min) and glomerular filtration rate (GFR, ml/min).
Survey items. Age, sex, height (cm), weight (BW, kg), body surface area (BSA, m2), BMI (kg/m2), Scr, blood urea nitrogen (BUN, mg/dl), serum albumin (Alb, g/dl), and 24 h CLcr (ml/min) were recorded as background parameters. The Scr level was determined using an enzymatic assay system (13). BSA was calculated using the DuBois equation (BSA=BW0.425×height0.725×0.007184). BW was converted to lean body weight (LBW) using the following formula if the patient's BW was heavier than their LBW:

In both the pre- and post-cisplatin groups, 24 h CLcr was calculated based on the equation described above, and various predictions of renal function were computed using the predictive functions described in Table II. All predicted CLcr and GFR values were corrected according to BSA, and the renal function values were multiplied by the patient's BSA divided by 1.73 m2 (the mean BSA for Japanese).
Therapeutic conditions. Four kinds of cisplatin-based regimens were used during the chemotherapy: (a) Cisplatin alone: cisplatin (80 mg/m2) was administered on day 1 every three weeks as part of concurrent chemoradiotherapy. (b) Cisplatin/5-fluorouracil (5-FU): cisplatin (70 mg/m2) was administered on day 1, 5-FU (700 mg/m2) was administered on days 1 to 4 every three or four weeks as part of concurrent chemoradiotherapy. Or cisplatin (80 mg/m2) was administered on day 1, and 5-FU (800 mg/m2) was administered on days 1 to 5 every four weeks. (c) Cisplatin-5-FU-docetaxel: cisplatin (75 mg/m2) and docetaxel (75 mg/m2) were administered on day 1, and 5-FU (750 mg/m2) was administered on days 1 to 5 every three weeks. (d) Cisplatin-tegafur-gimeracil-oteracil (S-1): cisplatin (25 mg/m2) was administered on days 8 to 11; S-1 (60 mg/m2) was administered on days 1 to 14 every four weeks.

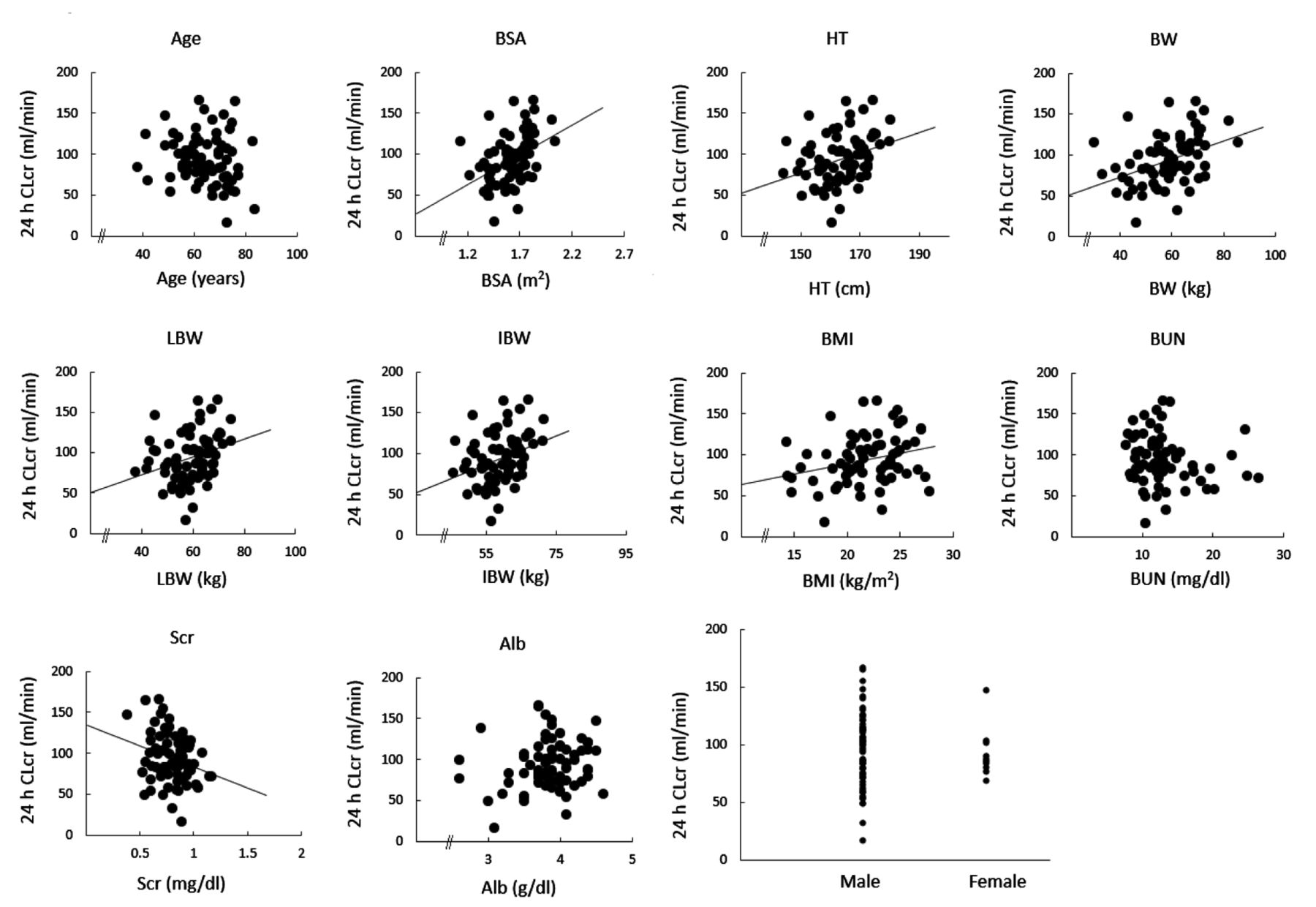
Relationships between patients' parameters and 24 h creatinine clearance (24 h CLcr, ml/min). HT: height (cm), BW: body weight (kg), LBW: lean body weight (kg), IBW: ideal body weight (kg), BSA: body surface area (m2), BMI: body mass index (kg/m2), Scr: serum creatinine level (mg/dl), BUN: blood urea nitrogen level (mg/dl), Alb: serum albumin level (g/dl), and gender (male/female), respectively. 24 h CLcr was calculated using the urine collection method. BSA, HT, BW, LBW, IBW, BMI, and Scr displayed significant correlations with 24 h CLcr (p<0.05).
All radiation therapy involved 70 Gy delivered in 35 fractions.
Statistical analysis. Statistical analyses were performed with Shapiro-Wilk W-test for normality and the Levene test for equality of variance, followed by Student's t-test or Pearson's product-moment correlation-coefficient analysis. All analyses were performed using JMP Pro®10.02 (SAS Institute Inc., Cary, North Carolina, USA). p-Values of less than 0.05 were considered to be statistically significant.
Construction of the predictive model. Multiple regression models for predicting 24 h CLcr from data obtained using the urine collection method (12) were prepared using the patients' background and laboratory data (Table I). Pearson's correlation coefficients were calculated for the relationship between 24 h CLcr and each parameter. A stepwise method was used to select the parameters for the multiple regression model. The internal correlations among the variables included in each model were assessed using the variance inflation factor (VIF), i.e., a VIF exceeding 10 indicates internal correlation. Furthermore, the normality and uniformity of residual plots were also checked using regression diagnostics.
Estimation of the predictive performance of each model. CLcr predictions were obtained for patients pre- and post-cisplatin using seven commonly used models as well as the model constructed in the present study (Table II). The determination coefficient (R2) and root-mean-square error (RMSE) were used to estimate the predictive performance of each model. R2 and RMSE were calculated from the least squares regression line and a line with a slope of 1 and an interept of 0, respectively. In the MDRD and the modified MDRD, which are models for predicting GFR, the 24 h CLcr values were corrected using a factor of 0.719 (14).
Characteristics of the multiple regression model (Model 1).
Results
Patients. One hundred and fourteen patients (98 males, 16 females) were included in the present study. Seventy-two patients who did not meet the exclusion criteria were extracted as subjects for the analyses (Table I). The first-line chemotherapy was administered for 21 to 49 days, except for three cases in which it was administered for 18, 89, and 141 days, respectively. The treatment interval between the first and second course was less than 45 days.
Construction of the predictive model. The patients' background and laboratory data (Figure 1 and Table I) were evaluated as explanatory variables using multiple regression analysis. As a result of variable selection with the stepwise method, a model including the three variables that exhibited correlations with 24 h CLcr, namely, BSA, Scr, and Alb, was constructed. Predicted CLcr=107 BSA−115 Scr+14.9 Alb−45.8 (Model 1) (n=72, R2=0.459, RMSE=22.7, p<0.0001) (Figure 2, Table III).
BSA and Scr exhibited significant positive and negative correlations with 24 h CLcr (R=0.426, p=0.0002 for BSA; R=−0.262, p=0.0262 for Scr), respectively. On the other hand, Alb was not significantly correlated with 24 h CLcr (p=0.138). No multicolinearity was observed among the explanatory variables included in the model. Similarly, regression diagnostics did not detect any abnormalities in Model 1.
Comparison of predictive performance. The mean 24 h CLcr values of the patients pre- and post-cisplatin were 93.6 and 78.8 ml/min, respectively. The patients' CLcr values post-cisplatin were well-predicted by Model 1 (n=30, R2=0.421, RMSE=18.8, p=0.0001), as were their pre-cisplatin CLcr values (Figure 2). The predictions obtained using Model 1 and the other examined models (Table II) are shown in Tables IV and V. All predictive models exhibited significant predictive performance (p<0.05). In the patients pre-cisplatin therapy, the minimum and maximum RMSE values were 22.7 (Model 1) and 46.1 (MDRD model), respectively. In the patients post-cisplatin therapy, the corresponding values were 17.3 (Orita model) and 45.6 (MDRD model), respectively. Model 1 also displayed strong performance in the post-cisplatin group, as did the Orita model (RMSE=18.8) (Table V).
Creatinine clearance (CLcr, ml/min) and glomerular filtration rate (GFR, ml/min) predictions obtained for the pre-cisplatin group using previously reported models and Model 1.
Discussion
We constructed a new model for estimating the renal function of patients treated with cisplatin-based chemotherapy. In addition, we performed detailed analyses of the predictive performance of the model. As a result, it was shown that a combination of BSA, Scr, and Alb exhibited good performance during the prediction of the renal function of patients with cancer prior to chemotherapy. Furthermore, the model also performed well in patients who had been administered cisplatin. The predictive model constructed in the present study, Model 1, is similar to the MDRD model, which includes Alb as an explanatory variable. Although the MDRD model displayed good performance during the prediction of renal function in the pre-cisplatin group, compared to Model 1 it did not exhibit a good predictive performance in the post-cisplatin group. Creatinine is a product of creatine metabolism, distributed throughout water found in the body, and is freely filtered by the kidney glomeruli (15). These characteristics mean that a negative correlation exists between 24 h CLcr and Scr. Although Alb did not exhibit a proportional relationship with 24 h CLcr (Figure 1), it was selected as the one of the significant variables in Model 1 (Table III). The main function of Alb is to regulate colloidal osmotic pressure in the blood. Furthermore, Alb is used as an index of liver function and nutrition. The utility of Alb for predicting renal function might depend on the subject's physical and nutritional status because Scr production depends on muscle volume. Patients with head and neck cancer suffer muscle mass loss due to inadequate feeding, the effects of high-dose cisplatin, and pharyngeal pain. We consider that Alb compensates for muscle mass loss in such patients, which would affect the Scr levels. BSA is a better indicator of metabolic mass than BW because BW is affected by abnormal adipose mass. BSA might be a useful parameter for estimating renal function because the weight of the kidneys is proportional to BSA (16). The good predictive performance of Model 1 and the Orita model in the post-cisplatin group might have been due to the fact that both models include body size-related variables derived from weight and height. Specifically, Model 1 and the Orita model include BMI and BSA, respectively. On the other hand, the MDRD model does not include any such factors. Katja et al. also reported that models that included body size-related parameters were preferred for estimating renal function in patients with lung cancer (17). The adjustment of renal function parameters based on such body size factors might be a suitable method for predicting CLcr in patients with cancer.

{kind=link}
{kind=link}
Relationships between measured and predicted creatinine clearance (CLcr). CLcr predictions obtained with Model 1 were compared with 24 h CLcr in the pre-cisplatin patients (•) and post-cisplatin patients (o). Predicted CLcr (ml/min)=107BSA−115 Scr+14.9Alb−45.8. n=72, R2=0.459, RMSE=22.7, p<0.0001 in the pre-cisplatin therapy patients; n=30, R2=0.421, RMSE=18.8, p<0.0001 in the post-cisplatin therapy patients.
The models that exhibited good performance, namely Model 1 and the Orita model, were constructed using different approaches. Model 1 is an inductive model produced using multiple regression analyses. On the other hand, the Orita model is a mechanical model. Due to their different characteristics, Model 1 and the Orita model exhibit different tendencies in terms of prediction errors. Therefore, the combined use of both models might provide robust estimates of a patient's renal function.
Statistical parameters obtained with the least-squares method used to assess the predictive performance of previously reported models and Model 1 in the post-cisplatin group
Conclusion
In the present study, a model for predicting CLcr in Japanese patients with cancer treated with cisplatin therapy was constructed and demonstrated strong predictive performance. Furthermore, it was demonstrated that Alb is an important factor for predicting renal function in such patients, as are BSA and Scr. The predictive model and the knowledge gained in this study can be utilized in the clinical setting for patients who receive anticancer chemotherapy.
- Received January 17, 2015.
- Revision received February 4, 2015.
- Accepted February 6, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved