

Abstract
Aim: The present, was a feasibility study of extended-field (EF) external-beam radiotherapy (EBRT) and vaginal brachytherapy (VBT) given sequentially following complete staging and adjuvant chemotherapy for patients with advanced-stage endometrial carcinoma (EC). Patients and Methods: A cohort study was carried out in 38 patients with stage IIIC and IVB EC treated by surgery, six cycles of paclitaxel-carboplatin chemotherapy followed by EF EBRT and VBT. Results: A total of 60% of the patients had non-endometrioid histology, 45% had both pelvic and para-aortic lymph node metastases. Two patients experienced recurrence in the previously irradiated field. Five-year overall and progression-free survival were 77% and 72.5%, respectively. Grade 1 diarrhea and grade 1 cystitis were the most common acute and delayed side-effects. Conclusion: EF EBRT and VBT following complete staging and adjuvant chemotherapy is a safe and effective treatment for patients with advanced-stage EC. Compared to historical data, our study suggests an improved progression-free and overall survival with acceptable acute and delayed side-effects.
- Advanced-stage endometrial cancer
- extended-field external-beam radiotherapy
- intensity-modulated radiotherapy
Endometrial cancer (EC) is the most common gynecological cancer and the seventh leading cause of cancer death in women of developed countries (1). Patients with locally advanced disease and distant metastasis account for 15% to 30% of cases but more than half of all deaths. Virtually all early-stage and low-risk tumors are cured by surgery alone (2). Adjuvant treatment is reserved for patients with adverse tumor features, such as deep myometrial invasion, presence of lymphovascular invasion, poorly-differentiated or non-endometrioid tumor types and advanced-stage disease (3). There is controversy regarding the adjuvant management of women with optimally resected stage III and IV disease.
Postoperative pelvic irradiation has been shown to reduce the risk of pelvic recurrence without any overall survival (OS) benefit. This is related to a 15% to 30% rate of extrapelvic relapse. The addition of systemic chemotherapy has the potential to reduce the extrapelvic relapse rate and increase OS (4). However, the significance of treating para-aortic lymph nodes could be valuable as these nodes appear to be involved in more than 50% of patients with positive pelvic lymph nodes, and some have suggested that the majority of para-aortic lymph node metastases in these patients (88%) are located between the inferior mesenteric artery and the renal veins (3).
Retrospective studies have shown that combined modality treatment can lead to superior progression-free survival (PFS), OS and lower recurrence rate compared to either modality alone. However, the timing and sequencing of radiotherapy, the choice of chemotherapy agents, and the addition of brachytherapy remain to be established (5-7). Over the past two decades, there has been an increasing number of deaths due to EC, which may be related to an increased rate of high-risk histologies and advanced-stage disease (8). Adequately powered studies comparing different treatments adapted to each sub-group are lacking. The aim of our study was to evaluate the feasibility, safety and efficacy of EF EBRT and VBT given sequentially following complete staging and adjuvant chemotherapy for patients with advanced-stage EC
Patients and Methods
A retrospective cohort study was carried out of 38 patients with EC of FIGO (2009) (9) stages IIIC1, IIIC2 and IVB treated with surgery followed by adjuvant chemotherapy, extended-field external beam radiotherapy (EF-EBRT) and vaginal brachytherapy (VBT). Following Institutional Review Board approval (approval number; 14/13), the Radiotherapy Department's database was screened for eligible patients and demographic, surgical, and pathological data, together with information on chemotherapy, radiotherapy and clinical outcome were extracted. Total hysterectomy, bilateral salpingo-oophorectomy, peritoneal washings, pelvic and para-aortic lymph node dissection, omentectomy and maximal tumor debulking were performed either by laparotomy or robotically assisted minimally invasive surgery. Following six cycles of adjuvant chemotherapy containing carboplatin and paclitaxel, patients were evaluated by either computed tomography (CT) of the thorax, abdomen and pelvis or whole body Positron Emission Tomography scan.
Summary of clinical and pathological characteristics of patients with stage IIIc and IVb endometrial carcinoma treated by extended field external beam radiation as part of a tri-modality approach (n=38).
Side-effects [n (%)] of extended field external beam radiation in patients with stage IIIc and IVb endometrial carcinoma treated by tri-modality approach (n=38).
Radiotherapy was planned to start 6-8 weeks post chemotherapy. EF-EBRT including the pelvis and para-aortic areas was delivered either by 4-field box technique (3D conformal; 3DC) or intensity-modulated radiotherapy (IMRT) technique. A total dose of 45 Gy, at a daily dose of 1.8 Gy, was administered in 25 fractions over five consecutive weeks. In patients with macroscopic residual disease following surgery and chemotherapy, or an area of significant risk of recurrence, a concomitant boost of 5-10 Gy was delivered to the affected areas (dose per fraction of 2-2.2 Gy). The superior border of all fields was placed to cover the contoured para-aortic clinical target volume up to the level of L1. It was extended to include adjacent visible, suspicious lymph nodes or positive lymph nodes on pathology. The inferior border was placed to cover the upper two thirds of the vagina, usually at the inferior aspect of the obturator foramina. The target volumes for the pelvis were drawn according to Consensus Guidelines for the Delineation of the clinical target volume in the Postoperative Pelvic Radiotherapy of Endometrial and Cervical Cancer (10). High-dose-rate VBT using either Nucletron CT/magnetic resonance imaging-compatible cylinder or Miami applicator was used in all patients immediately following EBRT. Patients received a total of 6-18 Gy in 1-3 fractions, depending on the involvement of the lower uterine segment or cervix, and status of the resection margins. The dose was prescribed at 5 mm depth from the vaginal vault, and at the surface of the upper 4 cm of the vagina. The dose to organs at risk was kept within the dose limits set by Emami et al. (11).
{kind=link}
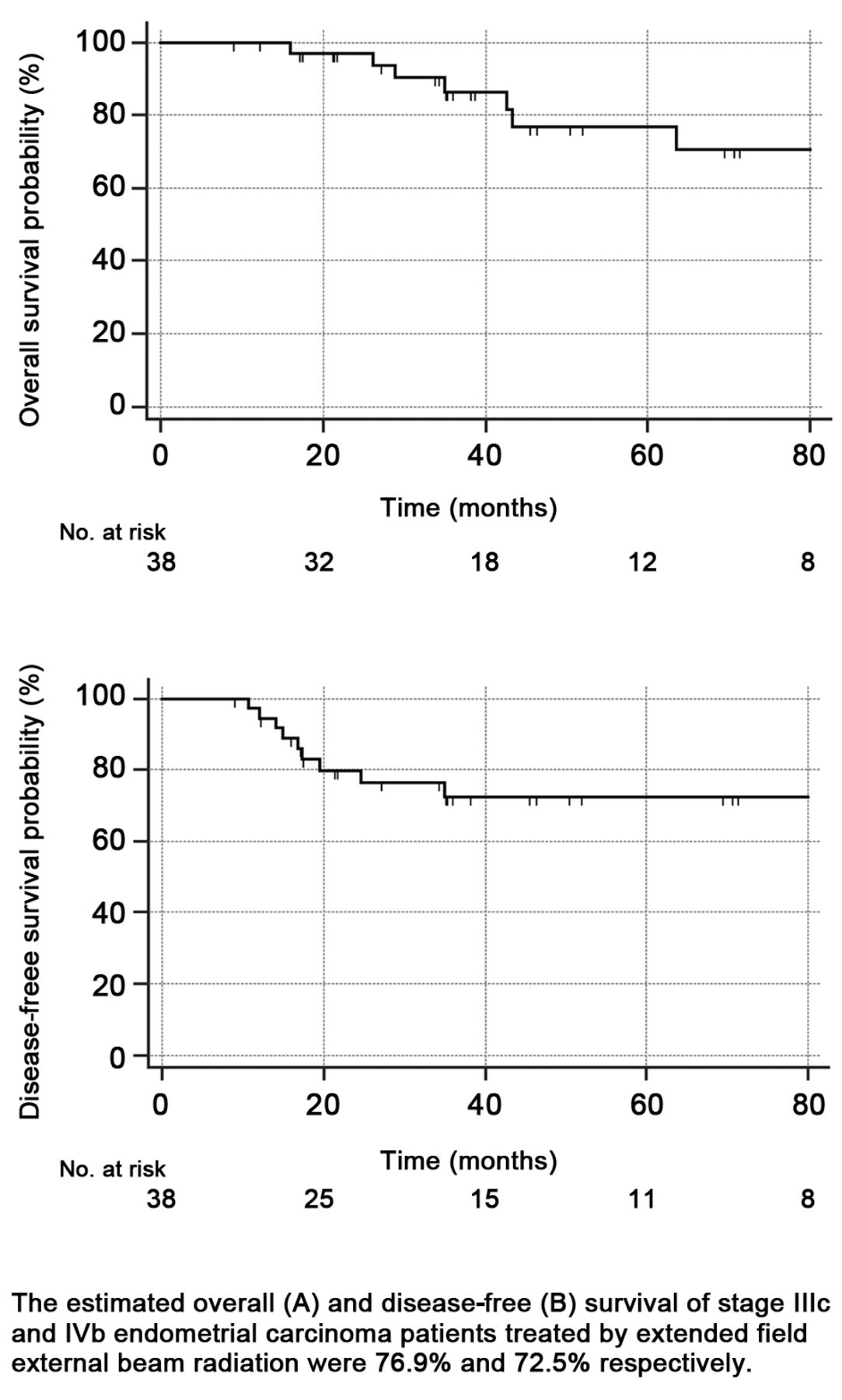
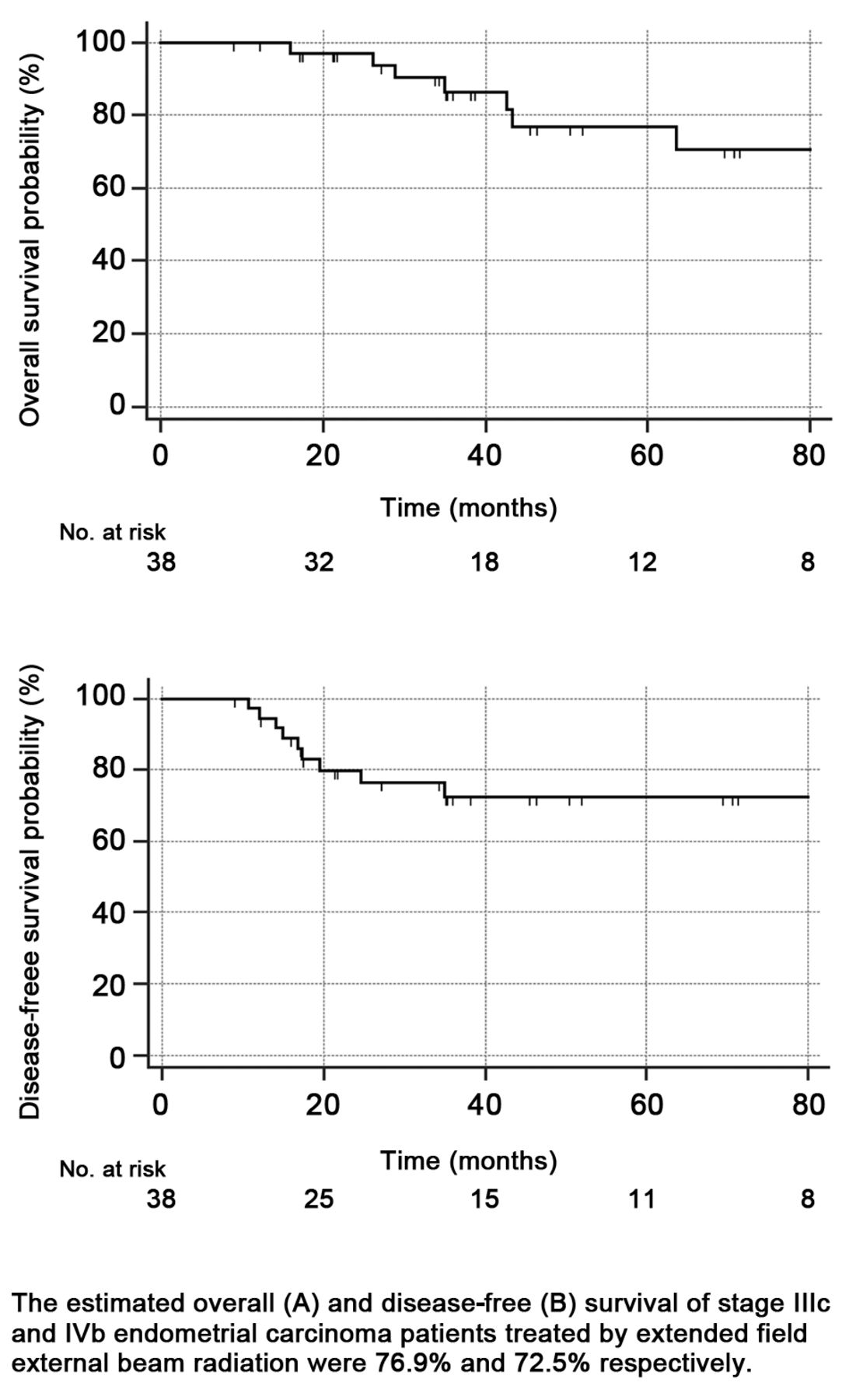
Projected overall (A) and disease-free (B) survival curves of patients with stage IIIc and IVb endometrial carcinoma treated by extended-field external-beam radiation as part of a tri-modality approach (n=38).
Grading of toxicity was based on the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.0 (12), with the highest grade of any observed toxicity reported for each patient. All patients received prophylactic anti-emetic. Patients were monitored for side-effects at each visit, once per week during treatment and every three months after the completion of treatment. After two years, patients were followed every six months for an additional three years, and yearly thereafter. The follow-up was performed alternating with the referring gynecological oncologist.
Disease-free survival (DFS) was defined from the date of surgery to the corresponding date of recurrence. OS was defined as the time elapsed from the date of diagnosis to the date of death or the date of last follow-up. Probability estimates of DFS and OS were determined using the Kaplan-Meier method. Hazard ratios were computed using the Cox proportional hazard model. All analyses were performed using SAS 9.3 software (SAS Institute Inc. Cary, NC, USA).
Results
Most patients had stage IIIC1 and 2 disease; five patients had stage IVB EC by omental or distant nodal involvement, but no liver or lung metastaseses were observed (Table I). Out of all tumors, 60% were deeply invading non-endometrioid tumors with associated high-risk factors such as lymphovascular space invasion and lower uterine segment involvement. A median of 11 lymph nodes were counted by pathology from the pelvis and, three from the para-aortic area. The median number and size of positive lymph nodes in the pelvis and para-aortic area were 2 and 4 cm, and 1 and 2.5 cm, respectively. Twenty-one patients had affected pelvic nodes and 17 patients (45%) had both pelvic and para-aortic lymph nodes involved.
In 37 patients, radiotherapy treatments were completed within 36 days without delays or dose reduction. One patient received only 32 Gy in 16 fractions without additional VBT due to non-recovering grade 4 thrombocytopenia. During treatments, side-effects were mild to moderate and easy to manage (Table II). Grade 1 diarrhea and nausea were the most significant acute side-effects. Hematological toxicities were encountered in 15 (39.5%) patients; only 2 patients (13.3%) had grade 3 and 4 toxicity. At the second follow-up, 4 months following the treatment, 63% of patients complained of cystitis, defined as one of the following: increase in urination frequency, urgency, dysuria, nocturia or new onset of incontinence. One year after treatment, 37.8% of patients still had symptoms compatible with grade 1 cystitis while grade 1 diarrhea was diagnosed in 11% of patients. Yet at the last follow-up, at a median of 39 months (range=9-109 months) after diagnosis, none of the patients complained of radiotherapy-related side-effects. Altogether, the Karnofsky performance status improved by 10% in six patients, declined by 10% in six patients, and remained unchanged in the rest.
Nine patients (23.7%) had recurrent disease at a median of 17 months (range=11-35 months) after initial diagnosis (Table III). All patients with recurrence had widespread distant metastases. In two patients, the recurrences were noticed in a previously irradiated field i.e. vaginal vault and para-aortic lymph node, respectively. On univariate analysis, grade 3 tumor and tumor histology, non-endometrioid vs. endometrioid histology, were found to be statistically significant predictors for poorer OS with hazard ratios (HR) of 12.0 [95% confidence interval (CI)=1.4-103.8; p=0.03] and 6.7 (95% CI=1.3-35.2, p=0.08), respectively. For disease-free survival, the corresponding values were 5.7 (95% CI=1.2-26.9, p=0.02) and 4.9 (95% CI=1.3-19.3, p=0.03), respectively. For recurrence of EC, the HRs for grade 3 tumor and such tumor histology were 5.0 (95% CI=1.0-24.5, p=0.05) and 4.3 (95% CI=1.0-17.4, p=0.1), respectively. On multivariate analysis, greater time from the last chemotherapy to start of radiotherapy was the only statistically significant predictor for poorer OS (HR=4.88, 95% CI=1.13-21.12). Using Kaplan-Meier statistics, the estimated 5-year OS and DFS were 76.9% and 72.5% respectively (Figure 1). With a median follow-up of more than three years after the initial diagnosis, 28 patients (73.7%) were alive with no evidence of disease, three were alive with recurrent disease, six had died of uterine cancer and one patient from unrelated causes (Table III).
Summary of clinical outcomes of patients with stage IIIc and IVb endometrial carcinoma treated by extended-field external-beam radiation as part of a tri-modality approach (n=38).
Discussion
The management of advanced-stage EC remains controversial. In surgically staged patients with EC, occult pelvic, and more importantly, extrapelvic metastases are the focus of treatment. Regardless of the regimen chosen, most of the 30%-40% treatment failures are predominantly due to extra-pelvic recurrences (13-15). With the exception of the Gynecologic Oncology Group (GOG) 122 trial (16), there have been no randomized controlled trials for locally advanced uterine cancer, despite the need to develop treatment strategies to improve survival and quality of life of such patients. In 2003, Martinez et al. published a retrospective analysis showing improved outcome at 10 years in 132 patients with serous-papillary/clear cell or high-risk endometrial cancers treated by adjuvant high-dose (30 Gy) whole-abdominopelvic irradiation (17). In their study, chemotherapy was used only at first relapse. A total of 89 patients had stage III disease (FIGO 1998 criteria), mostly due to positive peritoneal cytology (38%); 25 patients (19%) had positive pelvic/para-aortic lymph nodes. The para-aortic field was treated to 42 Gy, while the pelvis and vagina received 51 Gy and 58.2 Gy, respectively. With a mean follow-up of 6.4 years, patients with stage III disease had 73% and 62% cause-specific survival for adenocarcinoma or papillary-serous carcinoma, respectively. There were 13% of patients with grade III and 1% with grade IV bowel toxicity.
At the time of starting the present evaluation, data suggested that adjuvant chemotherapy with concurrent or sequential radiotherapy could be beneficial, but the results were not consistent (18), and the impact of EF radiotherapy on lymphatic recurrences beyond the pelvis remains uncertain (19, 20). EBRT alone and with VBT has been shown to reduce pelvic relapses, but treatment failures at distant sites, including the para-aortic area, are frequently observed (21). Because chemotherapy was used, in our study we omitted whole-abdominopelvic irradiation but increased the dose to the para-aortic field, keeping the same dose to the vagina. Many reports compare heterogeneous study populations and an array of adjuvant treatments, grouping high-risk stage I with stage IIIC patients and single modality with combined treatments. Consequently, the management of high-risk advanced EC is still frequently individualized (22, 23).
The present study focused on a homogeneous population of patients with advanced high-risk EC, stages IIIC and IVB without lung or liver metastases, and utilized one treatment approach consisting of six cycles of chemotherapy followed by EF-EBRT and VBT. In our cohort of patients, radiotherapy was generally well tolerated. Klopp et al. described hematologic toxicities in 37% of 43 patients with EC treated by IMRT alone as part of the RTOG 0418 trial, with approximately half having grade 3 or higher toxicity (24). Using two EBRT techniques, we encountered a similar rate of hematological toxicities, but significantly fewer grade 3 and 4 toxicities. In most cases, hematological toxicities did not necessitate treatment delay. Radiotherapy treatment was discontinued in one patient due to non-recovering grade 4 thrombocytopenia. Grade 1 diarrhea (79%) and grade 1 nausea/vomiting (55%) were the most common side-effects during radiotherapy. These were easily managed without causing treatment delays. In a smaller cohort of patients with stage III treated by EF-EBRT, De Jong et al. (25) reported similar results, 75% and 68.8% respectively. Similarly to Shih et al., who described late side-effects in 46 patients treated by IMRT only (26), our results depict genitourinary (GU) side-effects, particularly cystitis as the predominant late complication both at 4 and 12 months after treatment. Most publications focus on gastrointestinal (GI)/small intestine-associated side-effects because the small intestine is the most vulnerable organ in the pelvis and small-bowel damage has been associated with significant morbidity and mortality (27). Extending the field of radiotherapy has been associated with increased dosage to the small intestine, whereas implementation of the IMRT technique has been reported to reduce the dose to the small bowel (28). Chen et al. described a cohort of 101 patients treated by both 3DC and IMRT techniques (29). Their late grade 1 and 2 complication rates were 30.8% and 18% for GI and GU effects, respectively. The rate of severe late GI and GU toxicity is reported as 1%-25%, with an accepted average of 5% (27). None of the patients in our cohort had grade 3 or 4 GI/GU complications. After a follow-up of more than 12 months, there was no biochemical evidence of kidney injury. Moreover, none of our patients had any radiotherapy-related complaints at the last follow-up, on average 4 years after completion of radiotherapy. A 24% recurrence rate with a median time to relapse of 17 months are equal or better than the expected failure rate in advanced-stage EC regardless of the adjuvant treatment.
Kuku et al. (30) described their experience with 90 patients surgically-staged with IIIA-IIIC EC treated by adjuvant radiotherapy or chemotherapy only or combined radiotherapy and chemotherapy. Only 31% of their patients (28) had stage IIIC disease. Forty-one (45.5%) of their patients experienced disease recurrence, 17.1 months after treatment. Similarly to our findings, most (93%) of their patients had distant recurrences.
There exist only scarce information about site specific para-aortic region recurrence following EF radiotherapy. Milgrom et al. (31) described 33 patients with stage IIIC EC treated by EBRT concurrent with cisplatin followed by paclitaxel with carboplatin. Fifteen patients had EF-EBRT. Three patients (20%) experienced disease recurrence in the para-aortic nodes. Choi et al. treated 64 patients, 13 with stage IIIC disease, by EBRT with VBT (32); four patients had EF EBRT, two of whom experienced disease recurrence in the para-aortic area (50%). Only one patient in our cohort of 15 patients with stage IIIC2 had recurrence in the para-aortic region (6.6%).
Table IV presents OS and DFS data from prospective and retrospective studies describing treatment of patients with stage III and IV EC by various combined modality treatments. The estimated 5-year OS of 76.9% and DFS of 72.5% in our group of patients compares well to those of other combined modality treatments (21, 33-36). Similarly to Brown et al. (37), our results indicate an impact of tumor grade and non-endometrioid histology on OS and DFS in univariate analysis. On multivariate analysis, the time interval between the last chemotherapy to the beginning of radiotherapy stood out as the only statistically significant parameter influencing survival. Recently, Cattaneo et al. (38) concluded that delaying adjuvant radiation treatment by more than nine weeks after hysterectomy was associated with worse DFS and OS in patients with early-stage EC who did not receive chemotherapy. To the best of our knowledge, similar studies have not been conducted in patients with advanced-stage EC.
The results of this study are subject to the limitations inherent to any single-institution experience. Nonetheless, every attempt was made to select a homogenous patient population with detailed toxicity and outcome information. Grouping of stage IIIC with five stage IVB patients did not affect OS or DFS rates. Grade 3 EC had marginal statistical significance for recurrent disease on univariate but not on multivariate analysis. Furthermore, there were no significant differences in survival rates between patients treated by 3DC and IMRT techniques (OS: HR=1.36, 95% CI=0.15-12.17; DFS: HR=1.27, 95% CI=0.33-4.97).
It is difficult to draw conclusions from the variety of studies, but one can conclude from the available data that we have not yet achieved optimal outcomes with the currently available therapies. Although randomized trials are underway to evaluate the role of combined modality therapy in high-risk and advanced-stage EC, many questions remain unanswered. Specifically, the extent of surgical nodal staging, the sequencing of systemic therapy and the systemic agents used, and the optimal radiation treatment volumes and doses are unknown. The randomized GOG 258 trial will determine if combination chemotherapy and radiation is superior to chemotherapy alone, whereas the PORTEC-3 trial will compare chemotherapy and radiation to radiation alone (39). The most significant limitation of the ongoing prospective trials is the inclusion of a heterogeneous group of patients with a wide distribution of stages, residual disease and operative procedures.
In conclusion, the use of regional radiotherapy may include treatment volumes that cover the pelvis/para-aortic lymph nodes, but the optimal treatment fields and doses have not yet been defined. The present study shows that despite pelvic or para-aortic nodal involvement, excellent local/regional control and very good survival rates might be achieved by employing a combination of chemotherapy with EF-EBRT, while avoiding significant/debilitating short or long-term side-effects. For Centers not implementing IMRT, the 4-field box technique (3D conformal) is an acceptable alternative. Optimal systemic therapy, radiotherapy and sequencing of the two modalities requires further research in order to improve survival and quality of life of patients who are at high risk of recurrence of EC.
Overall survival and disease-free survival in patients with advanced-stage endometrial carcinoma treated by combined tri-modality approach.
Acknowledgements
The Israel Cancer Research Fund, the American Physicians Fellowship for Medicine in Israel, the Israel Cancer Association, and Ben-Gurion University of the Negev supported the fellowship of Alex Rabinovich.
Footnotes
-
* These Authors contributed equally to this study
-
Conflicts of Interest
The Authors declare no conflict of interest in regard to this study.
- Received January 14, 2015.
- Revision received January 29, 2015.
- Accepted February 2, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved