

Abstract
Aim: We investigated whether serum markers and clinical factors could be used to preoperatively predict lymph node (LN) metastasis in colorectal cancer (CRC). Patients and Methods: The present study enrolled 157 curative CRC patients for whom preoperative serum carcinoembryonic antigen (CEA), systemic inflammatory markers (C-reactive protein (CRP) and angiopoietin-like protein 2 (ANGPTL2)) and objective preoperative clinical factors were available as indicators of pathological LN status. Results: Specific clinical factors, including gender, tumor size, histopathology of biopsy sample and tumor morphology, were significantly correlated with LN metastases. Additionally, CEA, CRP and ANGPTL2 levels were also predictive factors for LN status. Multivariate analysis revealed that clinical factors, including gender, histopathology, tumor morphology and ANGPTL2, were identified as independent predictive factors for LN metastases. A combination of clinical factors reached high predictive accuracy of LN metastases and, combined with clinical factors, ANGPTL2 further improved the accuracy. Conclusion: Serum ANGPTL2 improves preoperative detection of LN metastasis in CRC.
- ANGPTL2
- C-reactive protein
- CEA
- lymph node metastasis
- colorectal cancer
Colorectal cancer (CRC) is one of the most common malignancies worldwide and a major cause of cancer-related deaths (1). The only cure for CRC, in particular for patients with locally confined disease, is surgical resection. In general, curative surgical resection consists of primary, standardized, systematic dissection of all potentially-affected lymph nodes (LNs), which determines the extent of bowel resection. A recent meta-analysis revealed histopathological features of primary CRC that can predict LN metastasis (2). Among common histopathological findings, lymphatic invasion, tumor depth, tumor differentiation and tumor budding are known to be the most predictive factors of LN metastasis. However, these factors are not determined prior to surgery but by hematoxylin and eosin staining of tumor samples postoperatively; no single histopathological feature of the primary tumor convincingly and reliably predicts LN metastasis.
In contrast, imaging studies are frequently used to predict LN metastasis from CRC to determine preoperative treatment strategies. Imaging modalities frequently used for the preoperative diagnosis of LN metastasis in CRC patients include computed tomography (CT), magnetic resonance imaging (MRI) and endorectal ultrasonography (EUS). These modalities, however, have shown low image sensitivity for diagnosing LN metastases (3-5), making it difficult to tailor the extent of LN dissection.
Conversely, tumor size, tumor location, tumor morphology and histopathology in biopsy samples have also been demonstrated to be objective findings for predicting LN metastasis preoperatively (2). In addition, many biomarkers have the potential to act as supplementary tools for further improvement of LN metastasis classification in CRC patients. For example, we have previously demonstrated that the preoperative serum tumor marker carcinoembryonic antigen (CEA) and systemic inflammatory response markers, which include C-reactive protein (CRP) and angiopoietin-like protein 2 (ANGPTL2), are significantly associated with postoperative LN status (6, 7).
Thus, in the current study, we first evaluated which factors among preoperative objective clinical factors and serum markers reliably predict LN metastasis in CRC. Next, we investigated whether the combination of several independent predictors of LN metastasis improved the accuracy of LN metastasis detection, which may be valuable for treatment planning treatment in CRC patients.
Association between pre- and post-operative clinicopathological findings and lymph node metastasis.
Patients and Methods
Patients. A total of 157 patients (90 men, 67 women) with curative CRC were enrolled at the Mie University Medical Hospital, Japan, between January 1, 2006 and December 31, 2011. Exclusion criteria included inflammatory bowel disease, familial adenomatous polyposis, hereditary non-polyposis colon cancer or other rare and complex types of tumors. The mean age was 67 years (range=35-89). No patient received chemotherapy or radiotherapy before surgery and no perioperative mortalities were observed. All patients were classified according to the TNM classification: 48 patients had stage I disease, 55 had stage II and 54 had stage III CRC. The median follow-up duration was 18.3 months (range=1-62). This study was approved by the Institutional Review Board (IRB) of the Mie University Hospital in Japan. All participants provided written informed consent and indicated their willingness to donate blood for research.
Laboratory measurement of CEA and CRP. CEA and CRP were analyzed using routine blood tests. Blood samples from each patient were obtained within 1 week prior to surgery. The cut-off value for CEA was ≤5 ng/ml and >5 ng/ml according to the normal range used in our hospital. The cut-off value for CRP was defined as 0.5 mg/dl as levels <0.5 mg/dl are below the level of detection in our hospital.
ELISA. ANGPTL2 concentrations in serum were measured using the human ANGPTL2 ELISA kit (IBL, Fujioka City, Japan) made at Kumamoto University. The assay was performed according to the manufacturer's instructions and values are reported as ng/ml. In brief, 100 μl serum samples were incubated in microplate wells pre-coated with monoclonal anti-human ANGPTL2 antibody (IBL, Fujioka City, Japan) for 1 h at 37°C. After washing four times, the labeled antibody was added and incubated with captured ANGPTL2 for 30 min at 4°C. After washing five times, chromogen complexes (TMB solution) were added to the wells for a 30 min reaction at 37°C and the absorbance was read at 450 nm using a multiplate reader (Multiskan FC; Thermo Scientific, Rockford, IL) within 30 minutes after adding the stop solution. All specimens were tested blindly, measured in duplicate and the average of the duplicates was used for analysis.
Statistical analysis. The associations between preoperative clinical factors, including CEA, inflammatory status (CRP and ANGPTL2) and pathological LN metastasis status were analyzed using the Mann-Whitney test, Kruskal-Wallis test or the χ2 test, as appropriate. Receiver operating characteristic (ROC) analysis was performed to determine the diagnostic performance of several preoperative clinical factors for distinguishing CRC patients with pathological LN metastasis from those without. Sensitivity versus 1-specificity was plotted at each cut-off threshold and the area under the curve (AUC) values reflect the probability of correctly identifying CRC patients with pathological LN metastasis from those without. The optimal cut-off thresholds for diagnosis were obtained by the Youden's index. In brief, the optimal cut-off threshold values were determined at the point on the ROC curve at which the Youden's index (sensitivity+specificity-1) was maximal. Finally, a multivariable logistic regression model was used to calculate odds ratios (ORs) associated with LN metastasis according to several preoperative clinical factors. All p-values were two-sided and p<0.05 was considered statistically significant. All statistical analyses were carried-out using Medcalc 7.2 for Windows (Mariakerke, Belgium).
Results
Associations between pre- and post-operative factors and pathological LN status. We first examined the relationship between various clinical factors before surgery, such as the tumor marker CEA and inflammatory markers and those of post-operative pathological LN metastasis. Pathological LN metastasis positivity was significantly associated with large tumor size (p=0.02), tumor shape (ulcerative and/or diffuse type; p=0.0001), histopathology on preoperative biopsy (moderate, poorly differentiated and/or mucinous type; p=0.001) and females (p=0.04). In addition, levels of all preoperative serum markers (CEA, CRP and ANGPTL2) were significantly elevated in patients with LN metastases compared to those without (CEA; p=0.007, CRP; p=0.05, ANGPTL2; p=0.003). However, neither age nor tumor location revealed any association with pathological LN status.

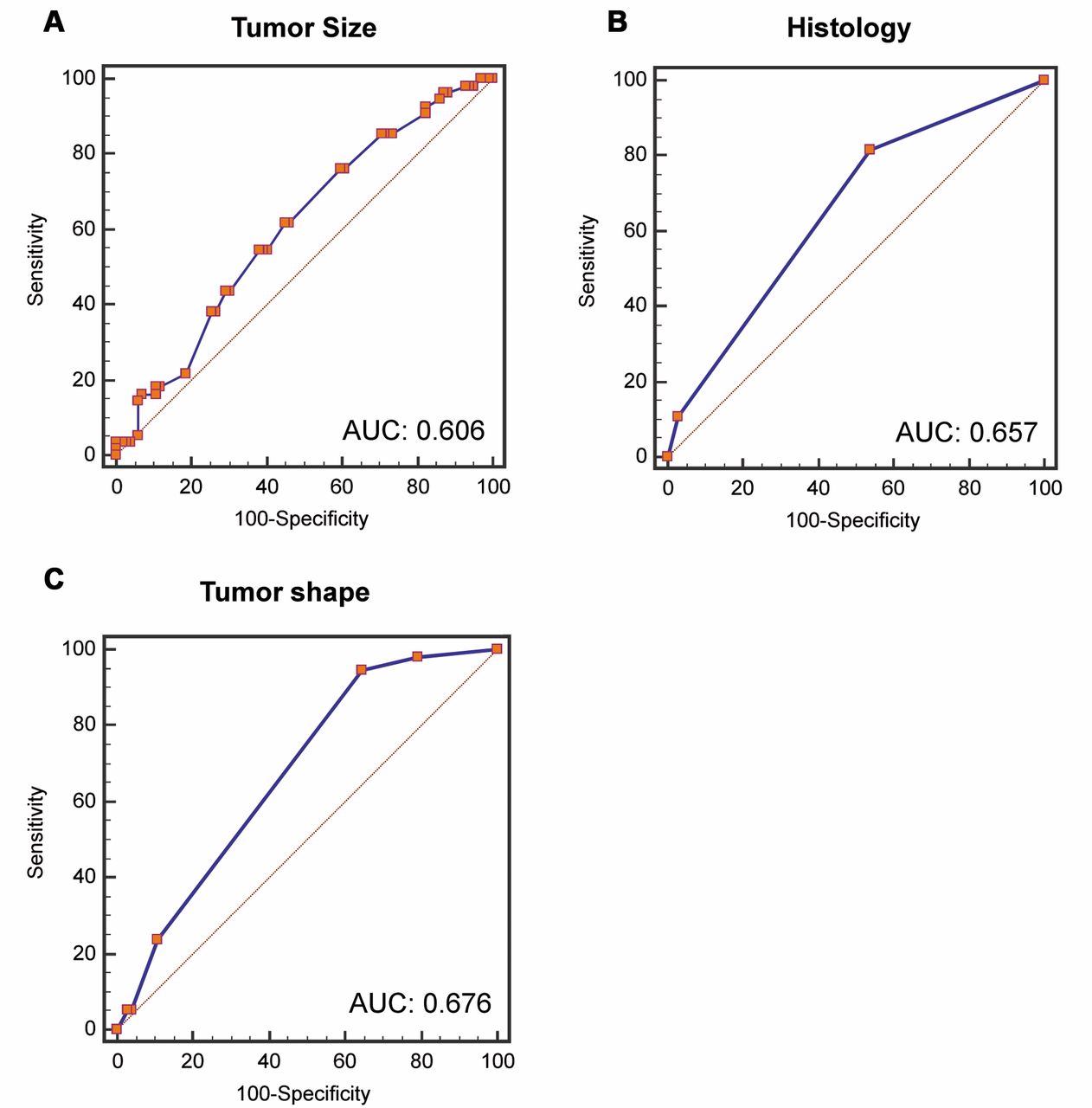
Receiver operating characteristics (ROC) curve analysis using preoperative objective factors for distinguishing colorectal cancer (CRC) patients with lymph node (LN) metastasis from those without. (A) Primary tumor size yielded an area under the curve (AUC) value of 0.606 (95% confidence interval (CI)=0.525 to 0.683) with 61.82% sensitivity and 54.90% specificity for distinguishing CRC patients with LN metastasis. (B) Histopathology in preoperative biopsy samples yielded an AUC value of 0.657 (95% CI=0.525 to 0.683) with 81.82% sensitivity and 46.08% specificity for distinguishing CRC patients with LN metastasis. Histopathological score was defined as follows: well-differentiated adenocarcinoma (score=0), moderately differentiated adenocarcinoma (score=1) and mucinous and poorly differentiated adenocarcinoma (score=2). (C) Tumor morphology yielded an AUC value of 0.676 (95% CI=0.596 to 0.748) with 94.55% sensitivity and 35.29% specificity for distinguishing CRC patients with LN metastasis. Tumor morphological score was defined as follows: superficial type (score=0), polypoid type (score=1), ulcerated type (score=2), local infiltrative type (score=3), diffuse infiltrative type (score=4) and mixed type (score=5).
We then examined the relationship between various postoperative pathological factors and pathological LN status. As expected, pathological LN metastasis was associated with pathological T stage (p=0.01), lymphatic duct invasion (p<0.0001) and venous invasion (p=0.02) (Table I).

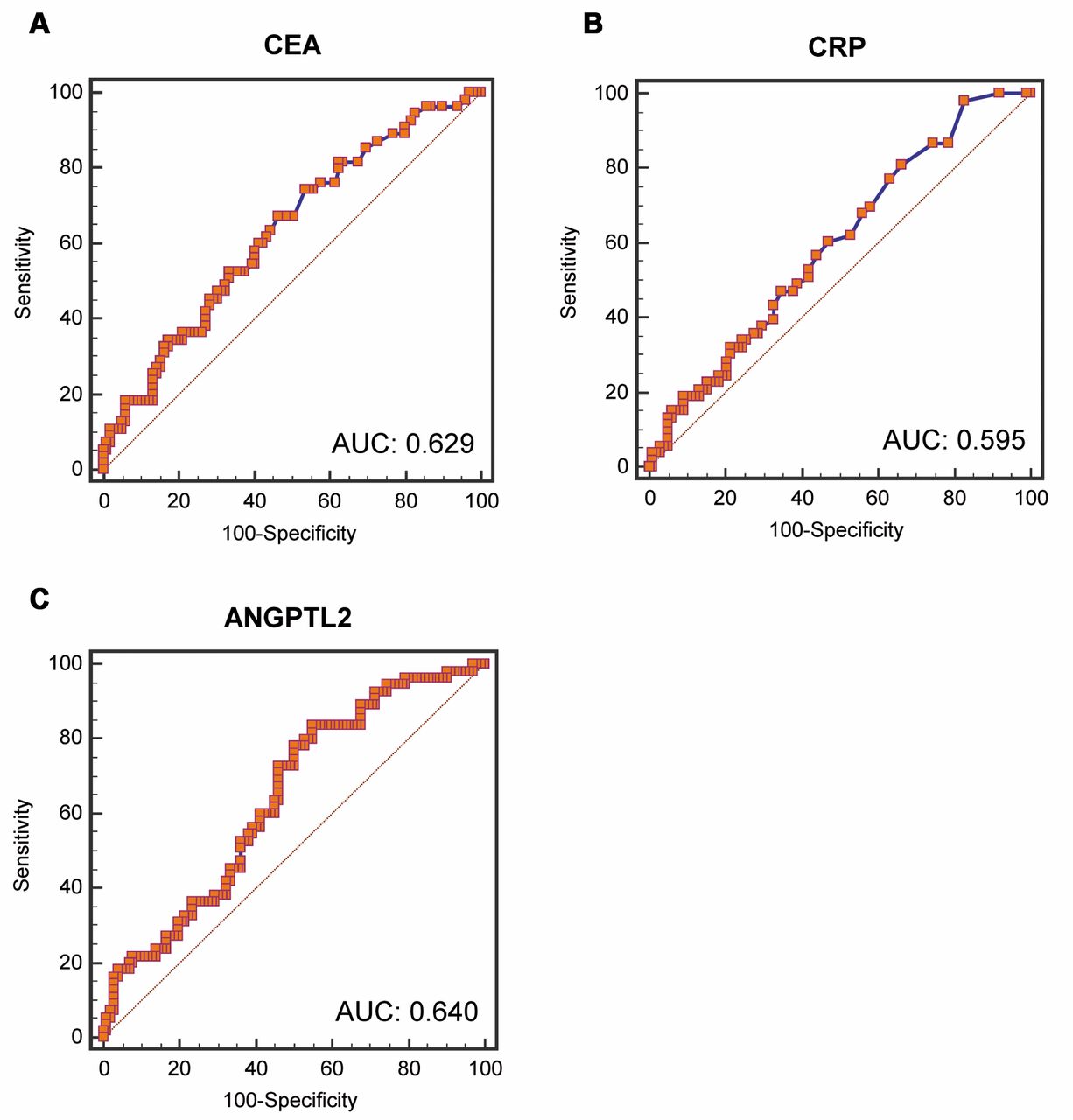
Receiver operating characteristics (ROC) curve analysis using preoperative serum markers for distinguishing colorectal cancer (CRC) patients with lymph node (LN) metastasis from those without. (A) Preoperative serum CEA yielded an area under the curve (AUC) value of 0.629 (95% confidence interval (CI)=0.548 to 0.706) with 74.55% sensitivity and 46.46% specificity for distinguishing CRC patients with LN metastasis. (B) Preoperative serum CRP yielded an AUC value of 0.595 (95% CI=0.512 to 0.674) with 98.11% sensitivity and 17.35% specificity for distinguishing CRC patients with LN metastasis. (C) Preoperative serum ANGPTL2 yielded an AUC value of 0.640 (95% CI=0.560 to 0.715) with 83.64% sensitivity and 45.10% specificity for distinguishing CRC patients with LN metastasis.
Predictive capacities of LN metastasis in patients with CRC using preoperative clinical factors and serum markers. We performed ROC analyses to evaluate the potential usefulness of preoperative clinical factors and serum markers as convenient biomarkers for the diagnosis of pathological LN metastasis. ROC analyses demonstrated that tumor size, tumor shape and histopathological findings in preoperative biopsies could reliably differentiate patients with pathological LN metastasis from those without (Figure 1A-C), as evidenced by AUC values of 0.606 (95% confidence interval (CI)=0.525-0.683; p=0.0219; tumor size), 0.657 (95% CI: 0.577-0.731; p<0.0001; histopathology on biopsy) and 0.676 (95% CI=0.596-0.748; p<0.0001; tumor shapes). In addition, ROC curves revealed that preoperative serum CEA, CRP and ANGPTL2 levels could significantly discriminate CRC patients with LN metastases from those without (Figure 2A-C), with AUC values of 0.629 (95% CI=0.548-0.706; p=0.0054; CEA), 0.595 (95% CI=0.512-0.674; p=0.0443; CRP) and 0.640 (95% CI=0.560-0.715; p=0.0018; ANGPTL2).

{kind=link}
{kind=link}
{kind=link}
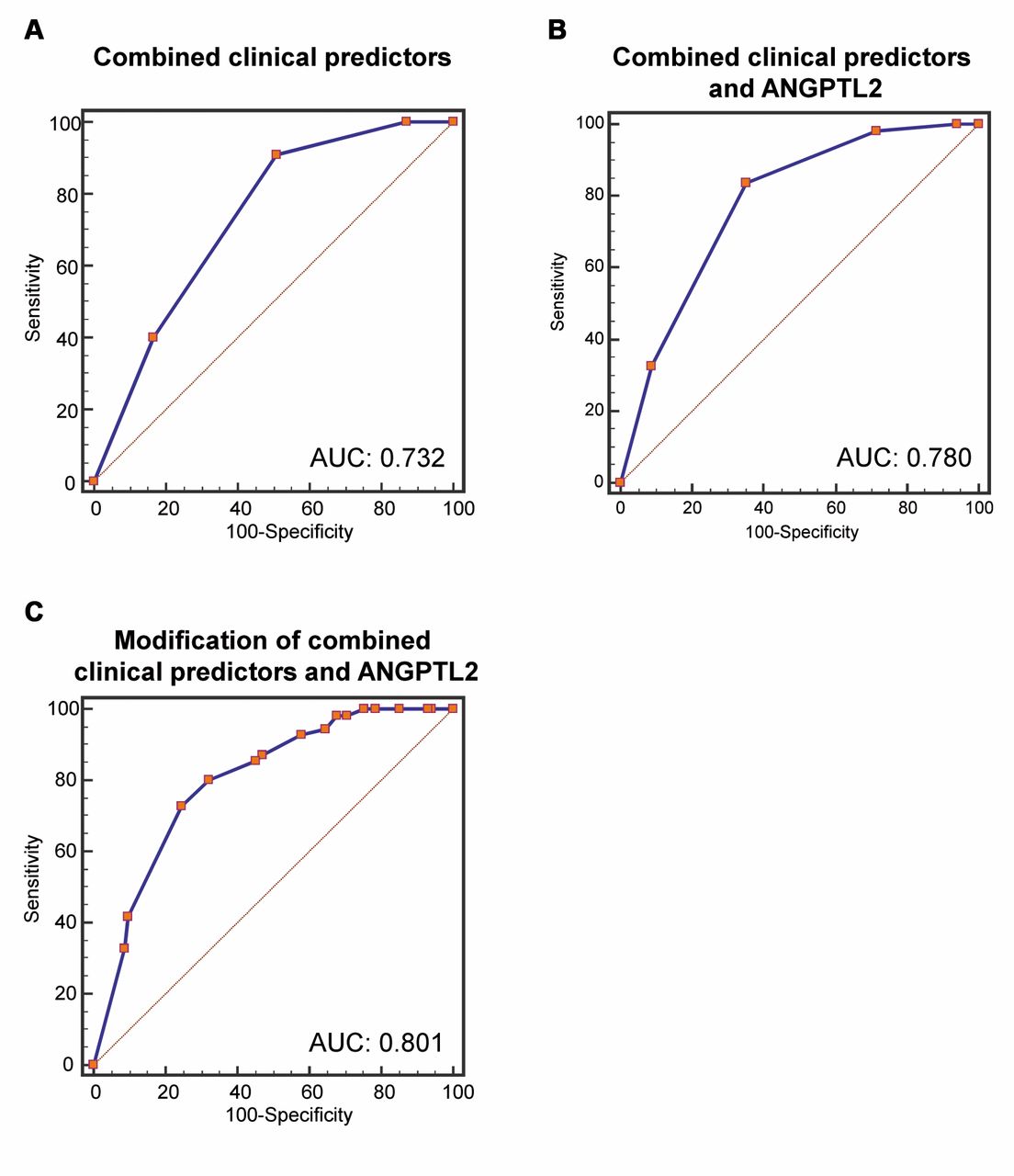
Combined receiver operating characteristics (ROC) curve analysis using preoperative independent predictors for distinguishing colorectal cancer (CRC) patients with lymph node (LN) metastasis from those without. (A) Combined ROC using preoperative independent clinical predictors (gender, tumor type and histopathology in biopsy sample) for predicting LN metastases yielded an area under the curve (AUC) value of 0.732 (95% confidence interval (CI)=0.655 to 0.799) with 90.91% sensitivity and 49.02% specificity for distinguishing CRC patients with LN metastases. (B) Combined ROC using preoperative independent clinical and serum predictors (gender, tumor type and histopathology in biopsy samples, as well as serum ANGPTL2) for predicting LN metastases yielded an AUC value of 0.780 (95% CI=0.708 to 0.843) with 83.64% sensitivity and 64.71% specificity for distinguishing CRC patients with LN metastasis. (C) Adjusting combined ROC by multiplying the hazard ratios of each independent predictor improved the AUC value to over 0.8 (95% CI=0.725 to 0.857) with 72.73% sensitivity and 75.49% specificity for distinguishing CRC patients with LN metastasis.
Univariate and multivariate analysis of preoperative factors for risk of LN metastasis.
Independent preoperative predictors of pathological LN metastasis in patients with CRC. The results from ROC analyses were further strengthened by logistic regression analyses that included variables, such as preoperative clinical factors and serum markers. In univariate analysis (Table II), pathological LN metastasis in CRC patients was associated with female (p=0.0275), large tumor size (>35 mm, p=0.0448), tumor shape (ulcerative, diffuse type, p=0.0001), histopathological findings of biopsy samples (moderate, poorly-differentiated, or mucinous adenocarcinoma, p<0.0003) and high levels of ANGPTL2 in preoperative serum (>1.2649, p=0.0002). Furthermore, multivariate analysis revealed that independent preoperative predictors of pathological LN metastases were female gender (hazard ratio (HR)=2.8514, 95% CI=1.2858-6.3235, p=0.0099), tumor shape and type (HR=15.0608, 95% CI=2.7506-82.4634, p=0.0021), histopathological findings of biopsy samples (HR=2.5716, 95% CI=1.070-6.1799, p=0.0347) and high serum ANGPTL2 levels (HR=4.0971, 95% CI=1.6635-10.0910, p=0.0022).
Serum ANGPTL2 combined with preoperative clinical factors improves prediction of LN metastasis in CRC. We next performed combined ROC analysis using independent preoperative predictors, such as gender, histopathological types on biopsy and tumor shape, to determine whether this approach can improve the predictive accuracy of pathological LN metastasis in CRC. The combination of three preoperative clinical factors successfully identified patients harboring LN metastases with a high AUC value (0.732, 95% CI=0.655-0.799; p<0.0001) (Figure 3A). Next, we added serum ANGPTL2 level, which was selected as the only preoperative serum predictor of LN metastases, to analyze whether this helps to further increase the ability to differentiate patients with LN metastasis. The results indicate that adding serum ANGPTL levels successfully improves the AUC value for selecting CRC patients with LN metastases (0.780, 95% CI=0.708-0.843; p<0.0001) (Figure 3B). Finally, we modified the risk of LN metastases by multiplying the HR of each independent preoperative predictor and performed combined ROC analysis. As expected, the AUC value for discriminating LN metastases increased to over 0.8 (0.801, 95% CI=0.725-0.857) (p<0.0001; Figure 3C).
Discussion
Surgery is the main treatment with curative potential for localized and metastatic (mainly LN and liver) CRC. The presence of disease at a site distant to the planned surgery affects the type and timing of treatment. Together, this wide variation in disease presentation and treatment extent underpins the rationale for accurate preoperative staging. Currently, neoadjuvant chemotherapy or chemo-radiotherapy are performed for stage II and stage III rectal cancer because neoadjuvant therapy decreases local recurrence and increases survival (8-11). Therefore, correct preoperative staging plays a critical role in determining whether patients should undergo neoadjuvant therapy in rectal cancer. Similarly, for colon cancer, preoperative strategies for the application of neoadjuvant treatments and decisions reducing the range of LN dissection are dependent on accurate LN staging (12).
Although colonoscopy is the most common method for detecting and diagnosing colorectal cancer, this technique does not produce accurate preoperative information regarding LN involvement (13). For this purpose, imaging using CT and MRI are standard modalities for preoperative staging of CRCs (14). Radiologists screen images for the occurrence of large LN (≥10 mm) to detect metastatic disease (15). Clearly, the likelihood of detecting a LN metastasis increases with increasing LN size (16, 17). However, even in the ≥10 mm group, the rate of LN involvement positivity is reported to be only 28% (16). In other words, 72% of very large LN are negative and the vast majority of positive LN metastases (73%) are <10 mm in diameter. Collectively, these data explain why the results of radiological imaging in the field are disappointing (18).
In contrast, a recent meta-analysis demonstrated the diagnostic performance of positron emission tomography (PET) scan for the preoperative assessment of LN staging in patients with CRC (19). The pooled estimates of sensitivity and specificity of PET/CT for the detection of preoperative LN involvement in patients with CRC were 42.9% and 87.9%, respectively (19). PET/CT can be used to confirm the suspected metastatic LN detected by other imaging modalities. Although a recent report demonstrated that, even with a standardized uptake value max of 2 or 3, pathologically metastatic LN were seen frequently (20) and there is no firm evidence to support the routine clinical application of PET/CT to determine LN involvement (21); thus, further clinical experience is needed to evaluate its utility for LN staging.
In the current study, we first investigated the detection accuracy of LN metastasis using preoperative features of CRC and serum markers, which are objective parameters. Data from our ROC analysis demonstrated that significant predictors included gender, tumor size, tumor histopathology and tumor morphology when colonoscopy was performed preoperatively, which is consistent with previous results (2). In addition, preoperative serum CEA, CRP and ANGPTL2 were also significantly associated with postoperative LN status. However, the detection accuracy of LN metastasis for each single parameter was under 70% (AUC <0.7). Thus, we performed multivariate logistic regression analysis to identify independent preoperative LN predictors since a combination of preoperative clinical features and serum molecular features may be able to better-identify pathological LN metastasis; several clinical features, including gender, tumor histopathology and tumor morphology, as well as ANGPTL2 levels as a serum marker, were independent LN predictors.
Next, we performed a combined ROC analysis using identified independent clinical predictors to evaluate whether the detection accuracy of LN metastasis can be increased. As expected, the AUC value increased to 0.73. Additionally, combining serum ANGPTL2 levels, which is another independent predictor, can further increase the diagnostic accuracy. Furthermore, adjustments using the HRs of each independent predictor finally brought us to over 80% accuracy. Collectively, we showed that objective evaluation using preoperative predictors of both tumor features and serum markers has the potential to diagnose LN metastases preoperatively.
In conclusion, we demonstrated -to our knowledge, for the first time- that the combination of identified preoperative tumor features can be a useful detection method for pathological LN metastases. In addition, adding preoperative serum ANGPTL2 levels can further improve the detection accuracy of LN involvement preoperatively. However, the specificity of our preoperative detection method regarding LN involvement is lower than imaging modalities (22, 23); thus, it might be better to use our method for LN staging assessment after multi-modality imaging evaluation.
Footnotes
-
Conflicts of Interest
The Authors have no conflicts of interest to disclose.
- Received February 1, 2015.
- Revision received February 6, 2015.
- Accepted February 10, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved