

Abstract
Background/Aim: Although it has been shown that microRNAs influence messenger RNA post-transcriptional control and can attribute to human tumorigenesis, little is known regarading the differences in microRNA expression between primary and recurrent epithelial ovarian cancer (EOC). The purpose of the present study was to assess the differential expression of microRNA between primary and recurrent EOC. Materials and Methods: Between September 2013 and May 2014, the expression of microRNAs in tumor tissues from 5 primary and 5 recurrent EOC cases were analyzed. The tumor histotype was serous cystadenocarcinoma in all patients. Total RNA was extracted from tumor samples and microRNA expression levels were measured by performing microarray analysis. Expression levels were compared between the two groups and analyzed statistically. Results: Several microRNAs were differentially expressed in recurrent EOC compared to primary EOC, including 18 under-expressed microRNAs and 33 over-expressed microRNAs among 6,658 human microRNAs. Four specific microRNAs were the most significantly over-expressed in recurrent EOC: miR-551b, miR-19b, miR-196b and miR-3198. Moreover, 4 specific microRNAs were the most significantly down-expressed in recurrent EOC: miR-8084, miR-3201, miR-3613 and miR-7515. Conclusion: Based on our data, dysregulation of microRNA expression was associated with the recurrence of EOC. Moreover, significantly over- and down-regulated microRNAs can be useful biomarkers for the prediction of recurrence in EOC.
- Epithelial ovarian cancer
- recurrence
- microRNA
Epithelial ovarian cancer (EOC) is the most lethal of all gynecological cancers, the fourth leading cause of cancer-related deaths in women in the United States and the fifth most common malignancy in women in developed countries (1). In general, less than half (45%) of EOC patients survive more than 5 years after their initial diagnosis (2). The poor survival in cases of EOC is due to the high percentage of patients diagnosed at an advanced stage that often develop resistance to combined chemotherapy.
Most patients with EOC are treated with platinum- and taxane-based chemotherapy. Although initial treatment is successful for 80~90% of patients, most responders eventually become resistant to a wide range of chemotherapeutic agents. While existing therapies are considered relatively effective in the treatment of EOC, mesenchymal/stem cell-like metastasizing EOC cells are generally resistant to these therapies and are largely responsible for EOC recurrence (3-5). The ability to predict which patients will respond to a distinct therapy would help to optimize personalized treatment.
MicroRNAs (miRNAs) are small (~22 nucleotide) non-encoding RNAs that regulate gene expression at the transcriptional and/or post-transcriptional levels (6). These molecules typically reduce the translation and stability of messenger RNA (mRNAs), including those of genes that mediate processes that are important in tumorigenesis, such as inflammation, cell-cycle regulation, stress response, differentiation, apoptosis and invasion. miRNA targeting is initiated through specific base-pairing interactions between the 5’ end (“seed” region) of the miRNA and sites within the coding and untranslated regions (UTRs) of mRNAs; target sites in the 3’ UTR lead to more effective mRNA de-stabilization (7). miRNAs play a role in the tumorigenic processes and hold potential as therapeutic targets and novel biomarkers in most types of human cancers, including ovarian cancer. Zhang et al. first suggested that approximately 40% of the miRNA genes exhibit altered DNA copy numbers (8). Moreover, some of the miRNAs associated with chemoresistance are also differentially expressed in advanced stage EOC and recurrent tumors. Low levels of miR-200c have been associated with a mesenchymal phenotype and, thus, may be associated with chemoresistance (9). Furthermore, low levels of miR-199a may reliably predict chemoresistance in recurrent tumors (10). These miRNAs can affect the response to chemotherapeutic drugs and might have both a prognostic, as well as a predictive value.
The comparison of miRNA expression between primary and recurrent tumor tissues may help reveal the mechanism of tumor recurrence and chemoresistance. Moreover, these miRNAs may be useful biomarkers for predicting tumor recurrence in EOC. To our knowledge, however, there is only one study that has reported examination of the expression levels of miRNAs in primary and recurrent EOC (11). The Authors concluded that miR-9 and miR-223 could be of potential importance as biomarkers in recurrent EOC (11).
In an attempt to understand the biology of recurrent EOC, we examined the expression of miRNAs in primary and recurrent EOC. The purpose of this study was to identify and compare the miRNA expression profiles in tissue samples of primary and recurrent EOC.
Materials and Methods
Patients and tissues samples. Between September 2013 and May 2014, tumor tissue specimens were obtained from 10 Korean patients with EOC (primary EOC, n=5; recurrent EOC, n=5) who underwent surgery at the Kyungpook National University Medical Center, Daegu, Korea. The histopathologic diagnoses were determined using the World Health Organization criteria and the tumor histotype was serous cystadenocarcinoma in all patients. The primary and recurrent EOC cases were different patient populations. The 5 patients with recurrent EOC received at least 6 cycles of platinum-based combination chemotherapy (paclitaxel plus carboplatin). The platinum-free interval was defined as the interval from the last platinum dose until progressive disease was documented. Tissue specimens were obtained during surgery and rapidly frozen in liquid nitrogen and stored at −80°C until analysis. Tissue samples were histologically confirmed by hematoxylin-eosin staining. The Institutional Review Board approved the study protocol and written informed consent was obtained from all patients.
miRNA microarray. Total RNA (2 μg) was extracted from the transduced cells using Trizol and the RNeasy Miniprep kit (Qiagen, Hilden, Germany) according to the manufacturers' protocols. The quality of the total RNA was verified with an Agilent RNA Bioanalyzer (Agilent Technologies, Palo Alto, CA, USA). Biotinylated cRNA was amplified using double in vitro transcription in accordance with the Affymetrix small sample labeling protocol VII (Affymetrix, Santa Clara, CA, USA). The total RNA was then hybridized onto an Affymetrix GeneChip® miRNA 4.0 according to standard protocols (Affymetrix user guide). Fluorescence intensities were quantified and analyzed using the Genechip operating software (Affymetrix). Raw data were normalized through the Robust Multi-array Average (RMA) method to remove systematic variations. Briefly, RMA corrects raw data for the background by using a formula that is based on a normal distribution and uses a linear model to estimate values on a log-scale. Transcripts whose log-transformed expression ratios differed by at least two-fold between recurrent and primary EOC tissues were identified.
Statistical analysis. For Genechip microarray analysis, statistical comparisons were made using the Student's t-test (ver. 12.0; SPSS, Inc., Chicago, IL). Differentially expressed miRNAs between primary EOC and recurrent EOC were detected through the t-test and data were considered statistically significant when p-value was <0.05.
Results
Clinicopathological characteristics of 5 primary and 5 recurrent EOC tissues. Table I summarizes the clinicopathological characteristics of the frozen tissue specimens used in this study. All patients were diagnosed with advanced-stage EOC (≥stage IIIB). The median platinum-free interval was 12 months (range=8-51) in the recurrent EOC cases.
Identification of differentially expressed miRNAs in primary and recurrent EOC. To identify miRNAs that were differentially expressed in recurrent EOC compared to primary EOC, we used a customized miRNA microarray that contained 6,658 human miRNAs. We analyzed the miRNA expression profiles of 5 primary and 5 recurrent EOC tissues using a two-color system. miRNAs were considered differentially expressed if the differences in their expression levels were greater than two-fold between the primary and recurrent cases.
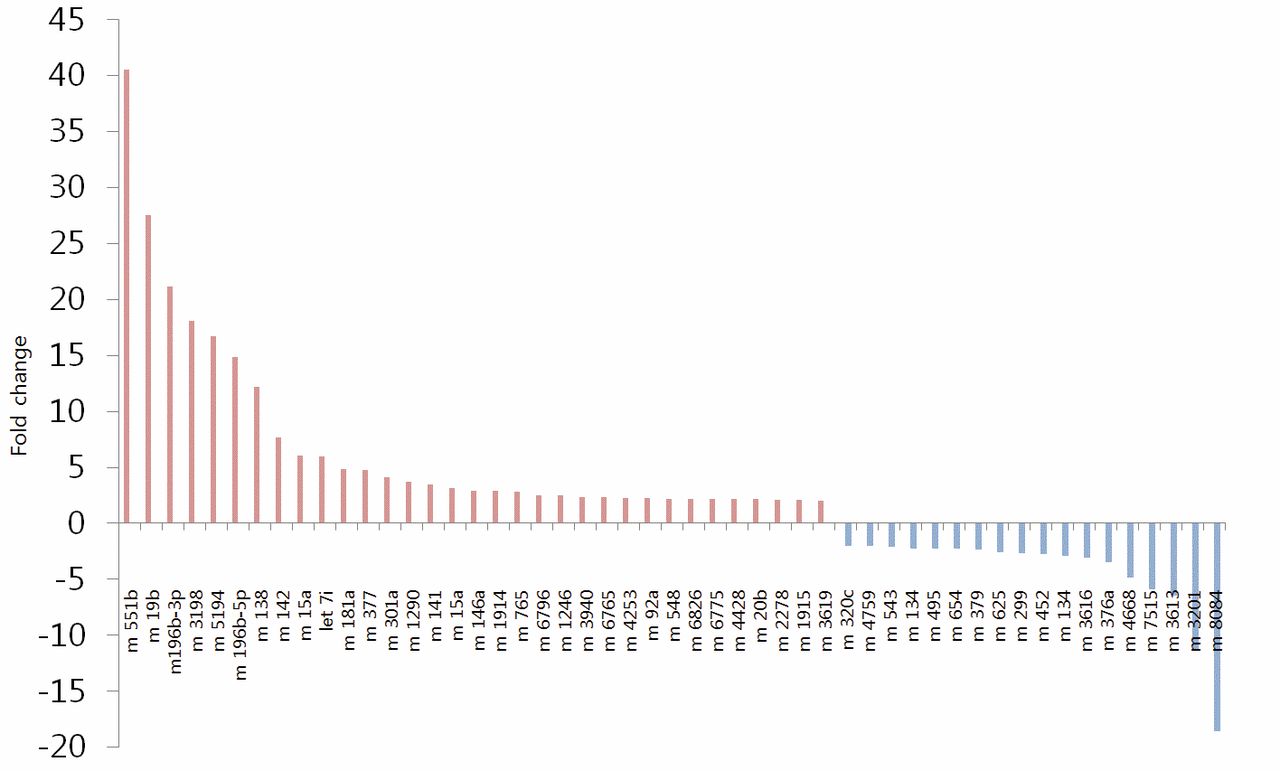
Figure 1 shows the results of the GeneChip® miRNA 4.0 Array assay. The under-expressed miRNAs (n=18) were miR-8084, miR-3201, miR-3613, miR-7515, miR-4668, miR-376a, miR-3616, miR-134, miR-452, miR-299, miR-625, miR-379, miR-654, miR-495, miR-134, miR-543, miR-4759 and miR-320c. The over-expressed miRNA (n=33) were miR-3619, miR-1915, miR-2278, miR-20b, miR-4428, miR-6775, miR-6826, miR-548, miR-92a, miR-4253, miR-6765, miR-3940, miR-1246, miR6796, miR-765, miR-1914, miR-146a, miR-15a, miR-141, miR-1290, miR-301a, miR-377, miR-181a, let-7i, miR-15a, miR-142, miR-138, miR-196b-5p, miR-5194, miR3198, miR-196b-3p, miR-19b and miR-551b (Table II, Figure 2).
Selection of miRNAs as biomarkers of recurrent EOC. In the Affymetrix miRNA 4.0 analysis, among 6,658 human miRNAs, 4 miRNAs were the most significantly over-expressed in recurrent EOC: miR-551b, miR-19b, miR-196b and miR-3198. As shown in Table III, the expression level of miR-551b was 130.1 (average score) in recurrent EOC and 3.2 (average score) in primary EOC (p=0.005). The expression level of miR-19b, miR-196b and miR-3198 were 76.5, 138.5 and 36.7 in recurrent EOC and 2.8, 6.5 and 2.0 in primary EOC, respectively (p=0.020, p=0.031 and p=0.029, respectively). The most down-expressed miRNAs in recurrent EOC were miR-8084, miR-3201, miR-3613 and miR-7515. The expression level of miR-8084, miR-3201, miR-3613 and miR-7515 were 2.9, 3.5, 156.2 and 2.3 in recurrent EOC and 54.7, 40.0, 1014.5 and 13.3 in primary EOC, respectively (p=0.002, p=0.008, p= 0.004 and p=0.024, respectively; Table IV).
Clinicopathological characteristics of the 5 primary and 5 recurrent cases of serous ovarian carcinoma.
Discussion
The present study demonstrates discrete miRNA signatures in primary and recurrent EOC in a histologically-homogenous set of ovarian tumor tissues (serous adenocarcinoma) from different patients. We identified 18 under-expressed and 33 over-expressed miRNAs in recurrent EOC compared to primary EOC. Among the 18 under-expressed miRNAs, 4 miRNAs were the most significantly under-expressed in recurrent EOC: miR-8084, miR-3201, miR-3613 and miR-7515. Among the 33 over-expressed miRNAs, 4 miRNAs were the most over-expressed in recurrent EOC: miR-551b, miR-19b, miR-196b and miR-3198.
The miRNA signatures of different cancer types could share some individual miRNAs (12). Of the miRNAs we detected as being over-expressed, many have similarly been shown to be over-expressed in other cancers: up-regulation of miR-551b in lung cancer (13), miR-19b in breast cancer (14) and non-small cell lung cancer (15), as well as miR-196b in oral cancer (16) and acute leukemia (17). However, to our knowledge, there exist no reports about miR-3198 expression in human cancers.
Expression profile of down-expressed and over-expressed miRNAs in recurrent versus primary epithelial ovarian cancers.

The results of microRNA Affymetrix array 4.0. (A) Signal scatter plots. (B) Heatmap of microRNA Affymetrix array 4.0.
Increased miR-551b expression in cells with acquired apoptosis resistance inhibited the expression of catalase and potentiated oxygen species accumulation and mucin-1 expression; mucin-1 is an important factor for acquired chemoresistance in lung cancer cells (13). Fan et al. demonstrated that the over-expression of miR-19b observed in human cancer cells can diminish p53 protein levels and this miR-19-mediated p53 reduction was shown to promote cell cycle progression, cell migration or invasion and to repress senescence and apoptosis (18). Furthermore, the over-expression of miR-19b significantly down-regulated the endogenous level of PTEN mRNA and promoted cell survival, rapid proliferation and cell growth. (19). The over-expression of miR-196b promotes an invasive and migratory phenotype in oral cancer through the NME4-JNK-TIMP-MMP signaling pathway (16).
{kind=link}
{kind=link}
Differentially expressed miRNAs in recurrent versus primary epithelial ovarian cancers. Relative fold changes are displayed on the y axis and the miRNAs are on the x axis.
Over-expressed microRNAs in recurrent epithelial ovarian cancers compared to primary epithelial ovarian cancers.
Down-regulated microRNAs in recurrent epithelial ovarian cancers compared to primary epithelial ovarian cancers.
To our knowledge, only miR-7515 is related to tumorigenesis of human cancer among the 4 most down-expressed miRNAs. miR-7515 led to decreased cell proliferation, migration and invasion in a lung cancer cell line by targeting c-Met (20).
Chemoresistance is the primary cause of the diminished anticancer efficacy (21). Although many patients initially respond to chemotherapy, acquired chemoresistance arises rapidly resulting in therapy failure (22). Notably, in cancer cells with chemoresistance, where chemotherapeutics lose their anticancer activity, they also promote cancer progression converting anticancer agents into tumor promoters (23). Importantly, one of the most significant prognostic factors is the response to platinum based chemotherapy in EOC. Moreover, many of the EOC patients who respond completely to first-line chemotherapy and who have no evidence of disease at the end of treatment are, unfortunately, diagnosed with recurrent disease during follow-up. In our study, all 5 recurrent EOC patients had received platinum-based combination chemotherapy (paclitaxel plus carboplatin). We identified 4 most significantly over-expressed and 4 most significantly under-expressed miRNAs in recurrent EOC compared to primary EOC. Our results may help to elucidate a new biological mechanism of chemoresistance and to identify recurrence biomarkers in EOC. To our knowledge, only one previous study has compared the miRNA expression between primary and recurrent EOC (11). They proposed a miRNA model for the molecular pathogenesis of recurrent EOC and determined that miR-9 and miR-223 might be of potential importance as biomarker in recurrent EOC (11).
In the present study, 33 miRNAs were over-expressed and 18 miRNAs were down-expressed in recurrent EOC. Furthermore, among 6,658 human miRNAs, 4 miRNAs were the most significantly over-expressed in recurrent EOC: miR-551b, miR-19b, miR-196b and miR-3198. Additionally, 4 miRNAs were the most significantly down-expressed in recurrent EOC: miR-8084, miR-3201, miR-3613 and miR-7515. These miRNAs may contribute to the understanding of the molecular pathogenesis of recurrent EOC and may be used as biomarkers for predicting the recurrence of EOC.
Acknowledgements
This research was supported by the new industry creation project of the National Research Foundation of Korea (NRF) Grant funded by the Korean Government (MSIP) (NRF-2013M3C1A8A01072754).
Footnotes
-
Conflicts of Interest
The Authors declare that there are no conflicts of interest.
- Received February 3, 2015.
- Revision received February 17, 2015.
- Accepted February 20, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved