

Abstract
Background/Aim: Combined hepatocellular-cholangiocarcinoma (cHC-CC) is found unexpectedly in explanted or resected liver specimens. The current study evaluated the longterm outcomes of living-donor liver transplantation (LDLT) between patients with cHC-CC and hepatocellular carcinoma (HCC). Patients and Methods: We performed 178 LDLT including 8 patients of pathologically and immunohistochemically diagnosed cHC-CC who all underwent LDLT with a preoperative diagnosis of HCC by imaging study. Results: Out of the 8 patients, 6 were within the Milan criteria and all were within the Kyushu University criteria. The 1-, 5- and 10-year overall survival (OS) and disease-free survival (DFS) rates after LDLT for patients with cHC-CC were 87.5, 72.9 and 48.6% and 85.7, 85.7 and 85.7%, respectively. The OS and DFS between patients with cHC-CC and HCC were not statistically different. Conclu sion: LDLT for patients with cHC-CC using the Milan criteria or the Kyushu University criteria, as well as HCC, could have an acceptable long-term outcome.
- Combined hepatocellular-cholangiocarcinoma
- hepatocellular carcinoma
- living-donor liver transplantation
Combined hepatocellular-cholangiocarcinoma (cHC-CC) is an uncommon form of primary liver malignancy composed of cells with histopathologic features of both hepatocellular carcinoma (HCC) and cholangiocarcinoma (CC) (1). It is almost impossible to obtain accurate preoperative diagnosis of cHC-CC with abdominal imaging studies. Therefore, liver malignancy with a preoperative diagnosis of HCC by imaging study is occasionally diagnosed with cHC-CC in explanted or resected liver specimens. We analyzed the longterm outcomes of living-donor liver transplantation (LDLT) between patients with cHC-CC and HCC.
Patients and Methods
Between July 1999 and March 2014, 178 patients underwent LDLT with a preoperative diagnosis of HCC by imaging study at our Institution. Indications for LDLT, the surgical techniques, and the immunosuppression protocol were described in our previous report (2-4). Eight patients were diagnosed for cHC-CC based on pathological and immunohistochemical features with the agreement of two pathologists. Their clinical, surgical and pathological data were collected retrospectively from the Institute's database, as well as from each patient's medical chart.
Patients' data are presented as medians and ranges. Survival rates were determined using the Kaplan-Meier method with a log-rank test.
Results
Patients' median age was 57.5 years (range=43-66). Four patients were male. Five patients had hepatitis virus C anti body and 3 had hepatitis B surface antigen. The maximal tumor diameter ranged from 0.7 to 6.6 cm (median=2.6). The median serum levels of alpha-fetoprotein, des-gamma carboxyprothrombin, carcinoembryonic antigen, and carbohydrate antigen 19-9 were 19.7 ng/ml (range=2.8-49.6), 50 mAU/ml (range= 13-613), 4 ng/ml (range=1-16.6),and 57.2 U/ml (0.6-100.9), respectively. The Milan criteria preoperatively were met in 6 cases and all cases were within the Kyushu University criteria. Pathological microvascular infiltrations, such as portal vein or hepatic vein infiltrations, were seen in 4 patients.
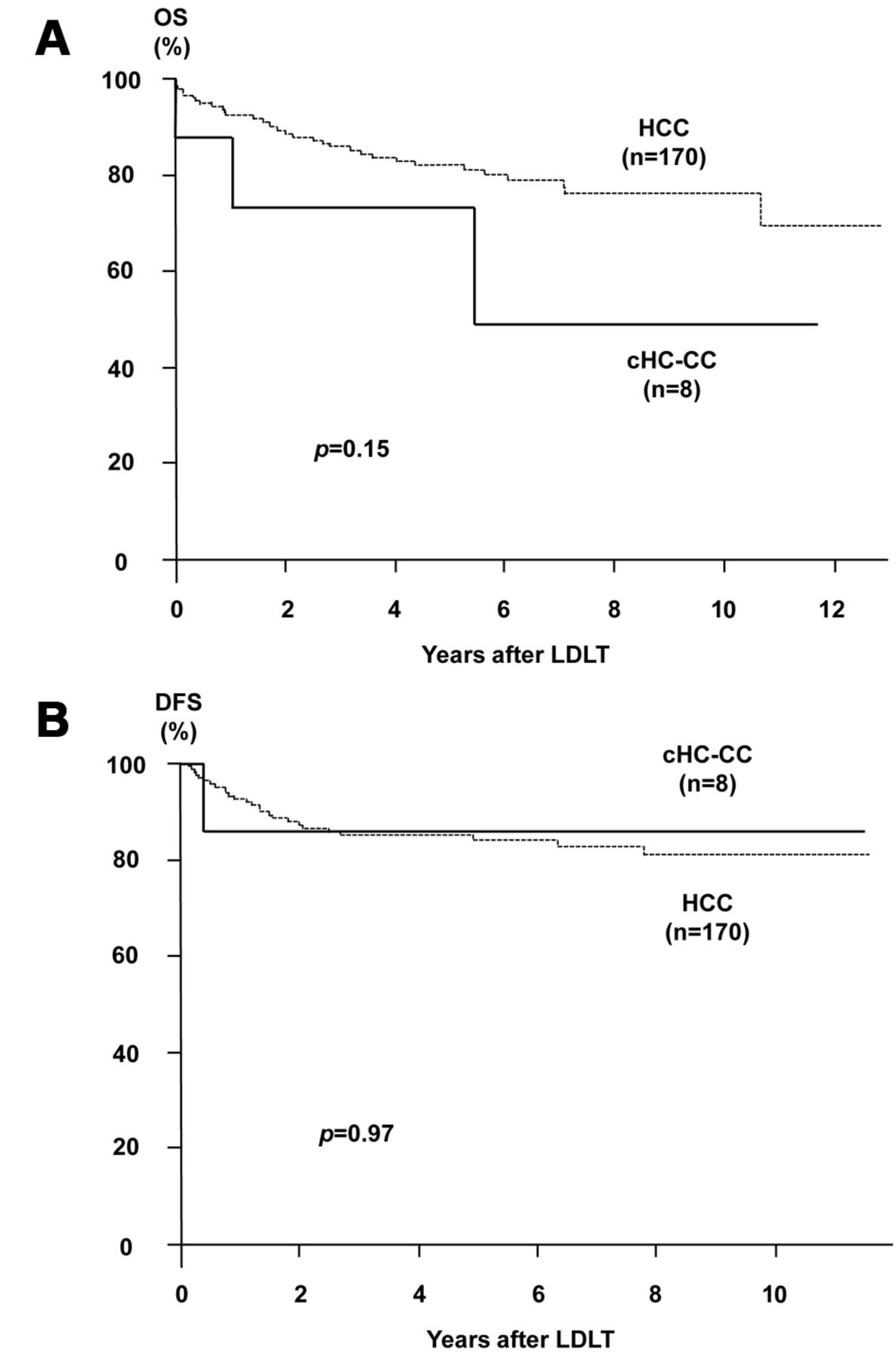
The 1-, 3-, 5- and 10-year overall survival (OS) and disease-free survival (DFS) rates after LDLT for patients with cHC-CC were 87.5, 72.9, 72.9 and 48.6 % and 85.7, 85.7, 85.7 and 85.7 %, respectively. The OS and DFS rates after LDLT for patients between patients with cHC-CC and HCC were not statistically different (Figure 1). Three patients with cHC-CC died during the observation period. The causes of death were primary graft dysfunction 9 days after LDLT, recurrence of cHC-CC and an accident. Only one patient had recurrence 5 months after LDLT, which was found in the para-aorta lymph node and lung.
{kind=link}
Overall survival (OS) (a) and disease-free survival (DFS) (b) curves after living-donor liver transplantation (LDLT) for patients between combined hepatocellular-cholangiocarcinoma (cHC-CC) and hepatocellular carcinoma (HCC).
Discussion
We herein report the first Japanese LDLT clinical study that com pares long-term outcomes between patients with cHC-CC and HCC at our institution. Yano et al. (5) showed that the clinicopathological characteristics of cHC-CC had more frequent macro scopic portal vein infiltration, more frequent multiple tumors, larger tumor size and poorer overall survival rate compared with typical HCC after hepatic resection. In the current study, patients with major vascular infiltrations were excluded from being candidates for LDLT. Therefore, there exist no statistical differences in OS and DFS after LDLT for patients between cHC-CC and HCC. Only one patient had early recurrence, with maximum tumor size of 6.6 cm and only one tumor, and died 13 months after LDLT. We recently reported that the maximum standardized uptake values (SUVmax) in fluorodeoxyglucose positron emission tomo graphy (PET) of cHC-CC were higher than that of the poorly differentiated HCC (6). Thus, PET evaluation might be useful for larger tumors towards the preoperative evaluation of the aggressiveness of primary liver malignancy, such as cHC-CC. A multi-institutional study is needed to provide evidence of the significant risk factors in LDLT for cHC-CC.
In conclusion, LDLT might be appropriate for patients with cHC-CC, as well as HCC, using the Milan criteria or the Kyushu Uni versity criteria and could have favorable long-term outcomes for these patients.
Acknowledgements
This work was supported by a grant Grant-in-Aid for Scientific Research (26380201) from the Ministry of Health, Labor and Welfare of Japan. No financial or other conflict of interest exists with the authors.
- Received January 11, 2015.
- Revision received January 29, 2015.
- Accepted February 2, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved