

Abstract
Background: Type IV macroscopic gastric cancer has the poorest prognosis of all gastric cancer types. Although progress of multidisciplinary treatments is outstanding, the current survival outcome of such therapies is obscure. Patients and Methods: Among 5,172 patients with gastric cancer between 1971 and 2013, 287 cases of type IV were identified (5%). We divided time period into early (1971-2004) and late periods (2005-2013), and compared their prognosis. Multivariate Cox proportional hazards model was applied to the univariate prognostic factors, and identified independent prognostic factors and long-term survivors. Results: Five-year overall survival (OS) was 13% and 31% in the early and late periods, respectively (p=0.0010). Univariate prognostic factors were age, pathological tumor depth of invasion (pT), pathological lymph node metastasis (pN), peritoneal dissemination (P), intra-peritoneal cytology test (CY), and margin status. Multivariate analysis determined independent prognostic factors to be treatment period (p=0.0001), pT (p=0.0024) and P (p=0.035). Survival outcomes were stratified by combination of pT and P in both periods, where OS was improved in the late period. Long-term survivors often underwent long-term postoperative chemotherapy with S-1. Conclusion: Long-term postoperative S-1 chemotherapy may improve survival outcome of patients with type IV gastric cancer, and their prognosis is predicted by pT and P status.
- Type IV gastric cancer
- survival
- chemotherapy
Gastric cancer is the fifth most common malignancy (952,000 cases in 2012) and the third leading cause of cancer-related death (723,000 deaths in 2012) worldwide (1). Advanced gastric cancer still has poor survival outcomes despite progress in multidisciplinary therapy (2, 3), while early gastric cancer is a curable disease (4). Among advanced gastric cancer types, Borrmann types I and II have relatively good outcomes, whereas the survival outcomes of Borrmann type IV cancer, known as linitis plastica, are extremely poor (5-8).
In Japan, D2 gastrectomy followed by postoperative chemotherapy with S-1 is the standard treatment for advanced gastric cancer (3), where this strategy is not necessarily satisfactory for improved prognosis of pathological stage III disease (9). Because patients who undergo postoperative chemotherapy often have inadequate nutritional intake, resulting in postoperative chemotherapy of insufficient dose intensity (10), neoadjuvant chemotherapy (NAC) may be an alternative promising strategy with conserved nutritional intake. In the Western world, surgery plus either perioperative chemotherapy or postoperative chemoradiotherapy has been reported to result in better overall survival (OS) in patients with resectable advanced gastric cancer (11, 12).
Although there is a notion that Borrmann type IV gastric cancer might not be indicative for surgery (13), long-term survivors are actually included in the group of patients with curative gastrectomy (6, 8). In Japan, instead of postoperative S-1 chemotherapy, some NAC regimens have been challenged in type IV gastric cancer in clinical trials. As a regimen for NAC, S-1 alone was disappointing for type IV gastric cancer compared to histological control in the JCOG0002 trial (6). Cis-diamminedichloro-platinum (CDDP, cisplatin)/S-1 remained promising as NAC treatment at present in Japan (14). Moreover, long-term administration of postoperative S-1 can be effective in stage II/III advanced gastric cancer, and may affect survival outcomes (15). Our Institute recently started to recommend patients to undergo docetaxel/CDDP/ S1 (DCS) therapeutic regimen for advanced gastric cancer including Borrmann type IV gastric cancer, and the overall response rate for DCS therapy against far-advanced gastric cancer was 81% (16, 17). Although progress of such multi-disciplinary treatments of advanced gastric cancer is outstanding, recent clinical outcome is uncertain in Borrmann type IV gastric cancer.

Overall survival (OS) of patients with gastric cancer is shown according to the Borrmann macroscopic features. N=5172, 1971-2013

Kaplan-Meier curves of overall survival (OS) in Borrmann type IV gastric cancer. a: Survival curve of total patients (1971-2013, n=287) is shown. Five-year OS represents 16.0%. b: Survival curves are shown according to time period. Prognosis was significantly better in the late period (2005-2013) than in the early period (1971-2004) (p=0.0010). c: Survival curve is shown according to clinical N stage of the lote period. Note that cases with cN3b exhibited dismal prognosis. d: Survival curves are shown according to the periods in Borrmann type IV gastric cancer excluding pT4b.
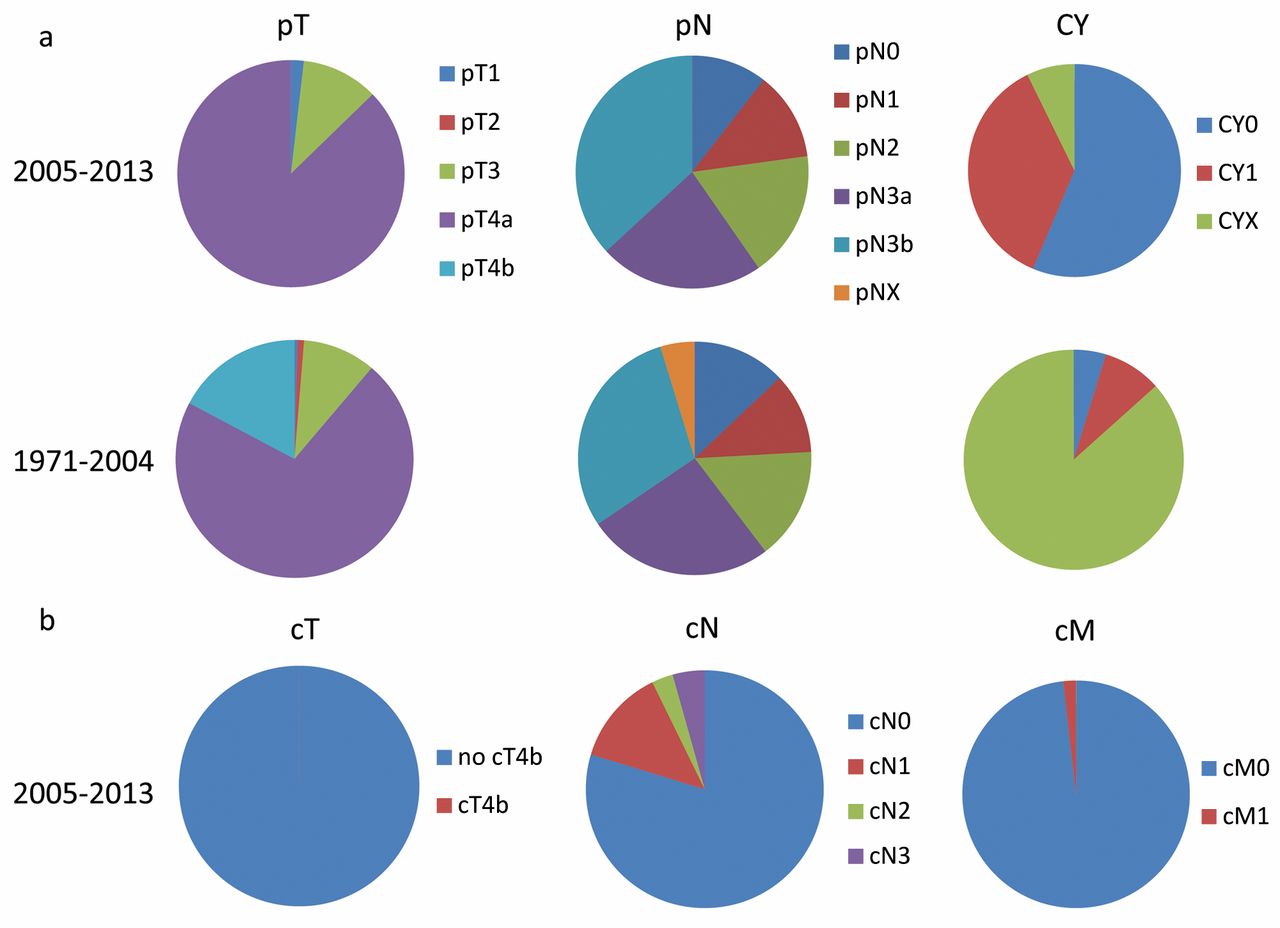
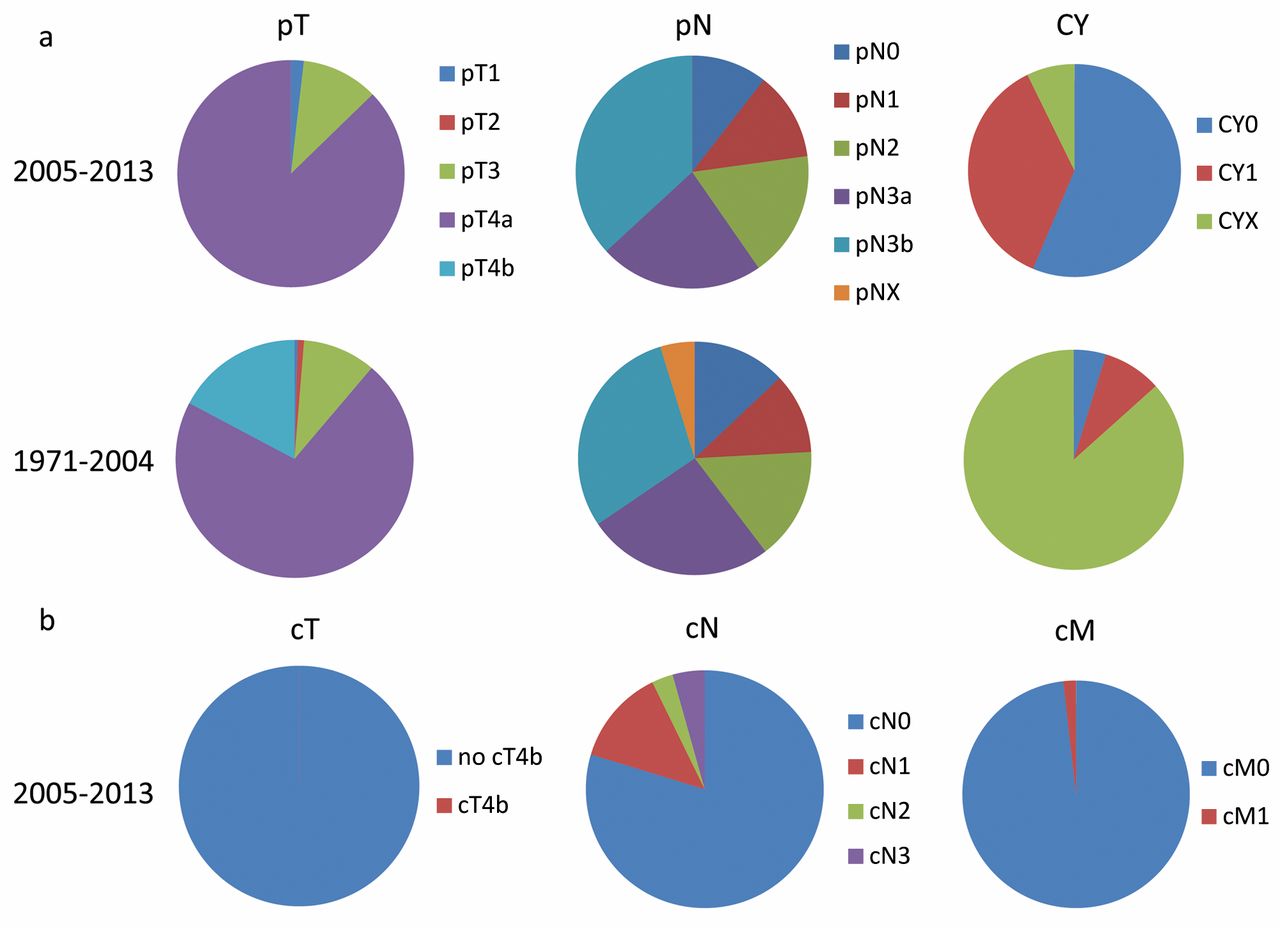
Distribution of clinical parameters are shown. a: Category distributions changed for pT and cytology (CY), but not for pN between the late (upper panel) and early periods (lower panel). b: Clinical stage in the late period.
Patients and Methods
Patients. Between 1971 and 2013, a total of 5, 172 patients with histologically confirmed primary gastric cancer underwent surgery at the Department of Surgery, Kitasato University School of Medicine, Sagamihara, Japan. Among these patients, 287 (5.5%) had a diagnosis of Borrmann type IV gastric cancer, as confirmed pathologically on gross examination of resected specimens. Intraoperative peritoneal lavage with cytological examination was carried-out in 82 patients (28.6%).
This study was conducted in accordance with the Declaration of Helsinki. The requirement for informed consent was waived because of the retrospective study design.
Clinicopathological factors. We performed prognostic analysis to identify independent prognostic factors in the 287 patients with Borrmann type IV gastric cancer. Pathological tumor depth (pT) and pathological lymph-node metastasis (pN) were classified according to the seventh edition of the International Union Against Cancer TNM staging system (18). Pathological tumor size was measured in accordance with the Japanese Classification of Gastric Cancer (19). The results of cytological examinations of either ascites or peritoneal lavage fluid (CY; cytology test) were evaluated according to the Japanese Classification of Gastric Cancer (JCGC) and were classified as CY1 (positive cytological test), CY0 (negative cytological test), CYX (not assessed by cytology) (19).
Chemotherapy. Adjuvant Chemotherapy Trial of S-1 for Gastric Cancer (ACTS-GC) showed in 2007, that S-1 is effective as adjuvant chemotherapy, and we positively participated in this clinical trial (3). From then, patients with stage II/III advanced gastric cancer were recommended to receive adjuvant chemotherapy with S-1. In 2009, the Institutional Review Board of the Kitasato University Hospital approved the use of docetaxel/cisplatin/S-1 regimen for the management of far-advanced gastric cancer (17).
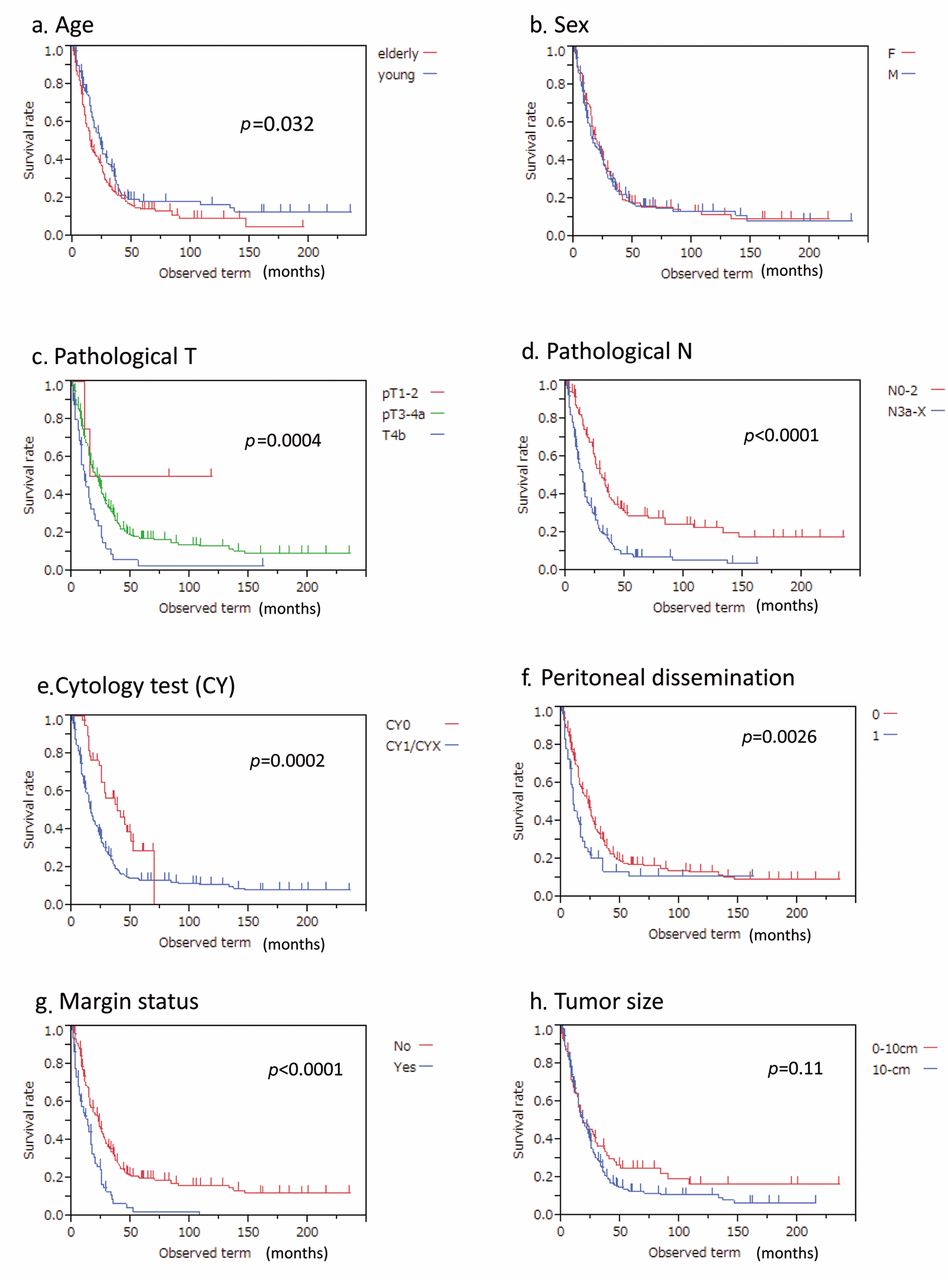
Kaplan-Meier curves of overall survival (OS) according to univariate prognostic factors in Borrmann type IV gastric cancer: a: Age (p=0.032); b: sex (no significant difference); c: pathological T stage (p=0.0004); d: pathological N stage (p<0.0001); e: cytological test (CY1: positive test; CY0: negative test; CYX: test not performed) (p=0.0002); f: peritoneal dissemination, 0: negative, 1: positive (p=0.0026); g: margin status, Yes: positive, No: negative (p<0.0001), and (h) tumor size (p=0.11).
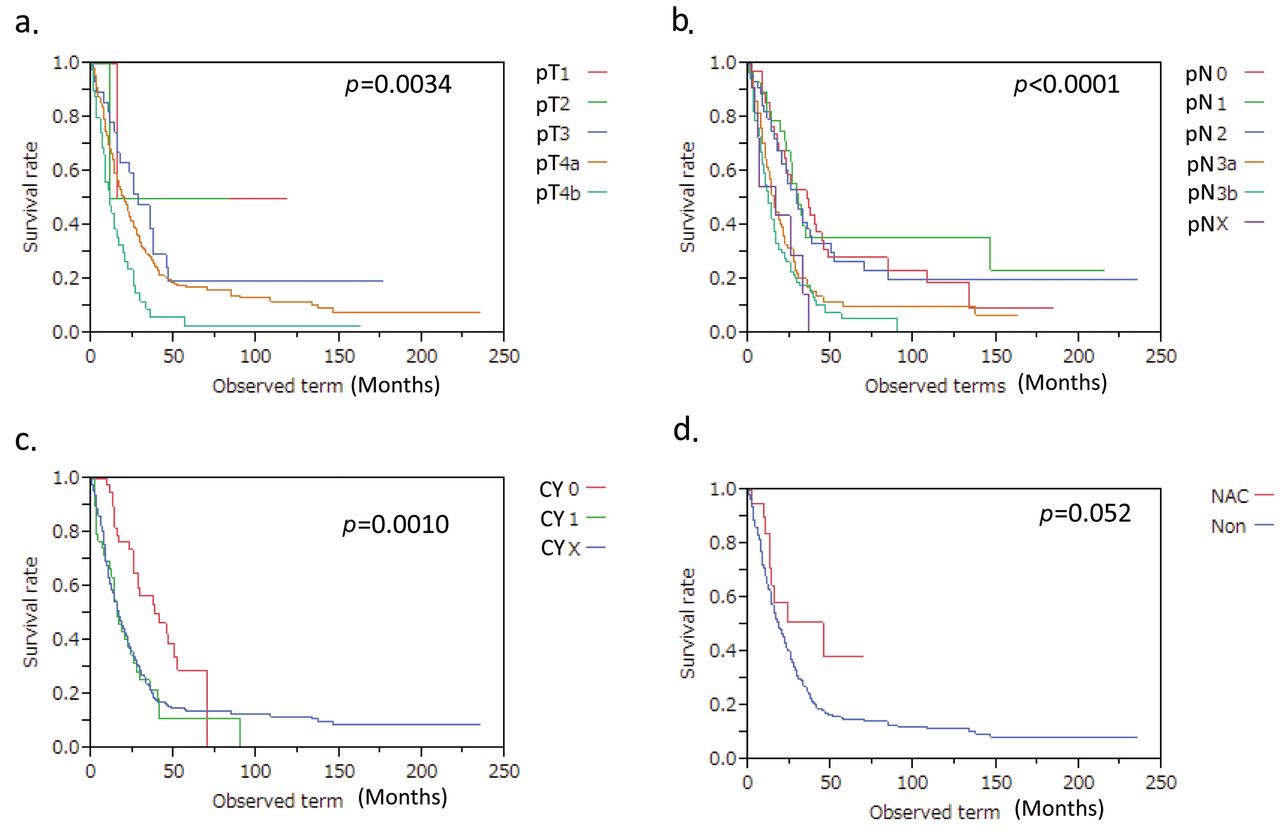
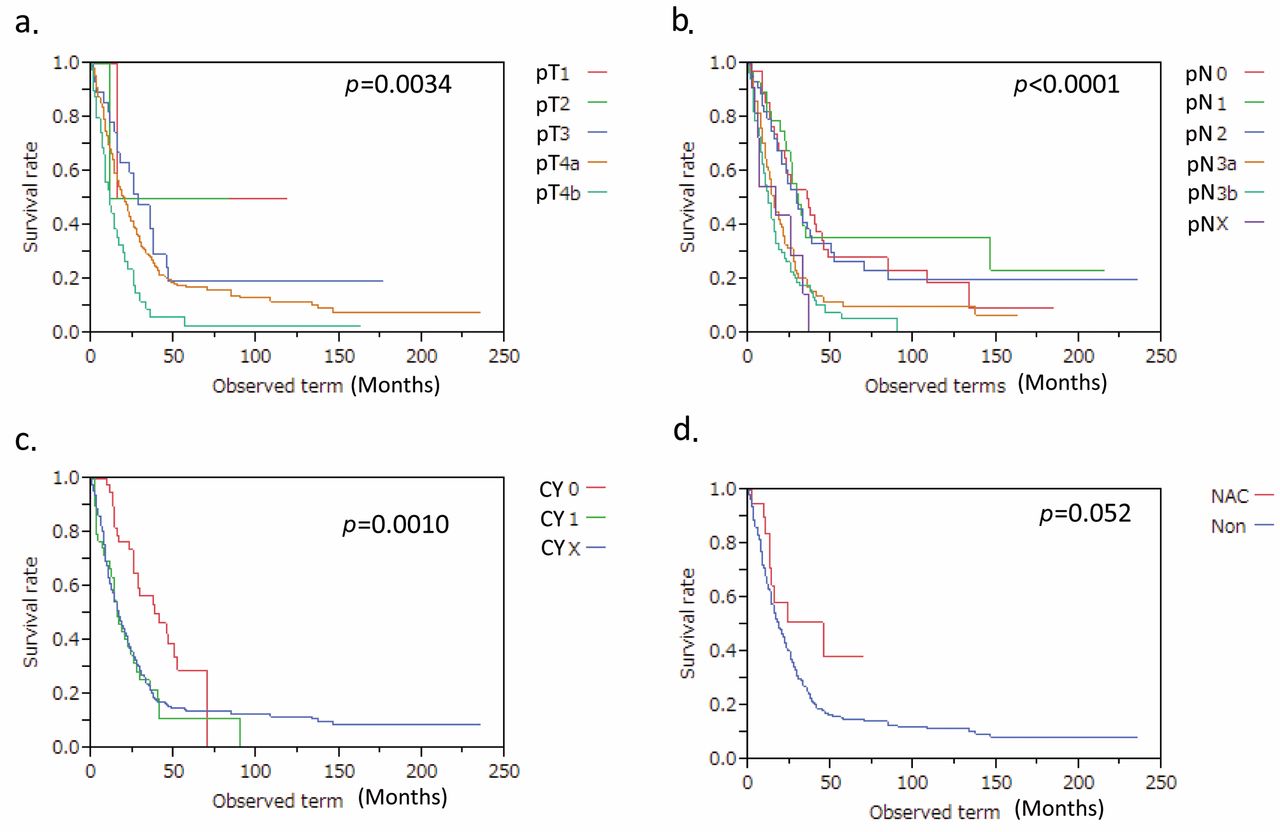
Kaplan-Meier curves of overall survival (OS) according to the following univariate prognostic factors in Borrmann type IV gastric cancer: a: Pathological T stage (p=0.0034); b: pathological N stage (p<0.0001); c: cytological test (CY1: positive test; CY0: negative test; CYX: test not performed) (p=0.0010); d: preoperative neoadjuvant chemotherapy (NAC) (p=0.11).
Statistical analysis. Continuous variables were evaluated by Student's t-test; categorical variables were evaluated by Fisher's exact test or the chi-square test, as appropriate. Survival was calculated by the Kaplan-Meier method. Univariate analyses of prognostic factors for OS were performed using the log-rank method. OS was defined as time from surgery to death from any causes, and data on surviving patients were censored at the last follow-up. The median follow-up was 36 months (range=0-235 months). Factors with a value of p<0.10 on univariate analysis were subjected to multivariate analysis using a Cox proportional-hazards model to identify independent prognostic factors. All calculations were performed with the use of JMP® 10 software (SAS Institute Inc., Cary, NC, USA). A value of p<0.05 was considered to indicate statistical significance.
Results
Borrmann type IV gastric cancer conferred dismal prognosis, but OS was improved in the recent treatment period (2005-2013). Among 5,172 patients with histologically-confirmed primary gastric cancer, Borrmann type IV gastric cancer was associated with the most dismal prognosis (Figure 1). Considering the 287 patients with Borrmann type IV gastric cancer identified in this current study, OS was 16% at 5 years (Figure 2a). Dividing the study period to perform surgery into early (1971-2004, n=232) and late periods (2005-2013, n=55), prognosis was significantly better in the late period than the early period (p=0.0010), with 5-year OS of 31% compared to 13%, respectively (Figure 2b).
Between the early and the late periods, there was significant difference in pT factor, while no significant difference in pN factor was recognized (Figure 3a) (Table I). During the late period, there was no case with pT4b. Even when pT4b cases were excluded, prognosis during the early period remained dismal (14.9% at 5 years) compared to that of the late period (p=0.0048, Figure 2d). These findings suggest that improved prognosis of the late period was not attributed to exclusion of pT4b cases of type IV gastric cancer. During the early period, cytology was carried out in 31/232 (13.4%) patients, while it was investigated in 51/55 (92.7%) during the late period (Table I, Figure 3a).
Regarding the clinical stage of the late-period patients, there were no cases of cT4b, and few of cN2/N3 or cM1 (Figure 3b). Unexpectedly, a large proportion of Borrmann type IV gastric cancer in the late period was composed of cN0 or cN1 cases. cN3 cases exhibited extraordinarily poor prognosis, while cN0-2 cases did not show unique prognosis (Figure 2c).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves of overall survival (OS) by combination of independent prognostic factors of pT and P according to time period. a: OS stratified by pT and P in the early period. OS for pT4b cases is shown separately because pT4b was only found in the early period. b: OS stratified by pT and P in the late period. Note that prognosis of the individual groups was improved.
Univariate prognostic analysis in Borrmann type IV gastric cancer. We then created Kaplan-Meier curves for potential prognostic factors in Borrmann type IV gastric cancer (Figure 4), and the log-rank test was used to compare the prognostic difference statistically (Table II). As a result, significant univariate negative prognostic factors were elderly age (Figure 4a, p=0.032), pT (Figure 4c, p=0.0004), pN (Figure 4d, p<0.0001), CY1 CYX (Figure 4e, p=0.0002), P (Figure 4f, p=0.0026), and margin status (Figure 4g, p<0.0001). There was no prognostic difference of sex (Figure 4b) or tumor size (Figure 4h).
pT factor was divided into pT1-2/pT3-4a/pT4b from a prognostic point of view (Figure 5a). pN factor was also divided into pN0-2/pN3a-X from a prognostic point of view (Figure 5b). CYX was associated with similar prognosis to CY1, hence CY was divided into CY0 versus CY1/CYX (Figure 5c). Preoperative NAC did not significantly affect prognosis in the patient cohort overall (p=0.052, Figure 5d).
Multivariate Cox proportional hazards model identified independent prognostic factors in Borrmann type IV gastric cancer. When multivariate Cox proportional-hazards model was applied to the significant univariate prognostic factors age, pT, pN, CY, P and margin status, independent prognostic factors were identified to be treatment period (p=0.0001), pT (p=0.0024), P (p=0.0086), and age (p=0.035) (see hazard ratio and 95% confident interval in Table II).
Prognostic curves by combination of pT and P status according to periods. We then stratified OS by combination of pT and P status according to treatment period (Figure 6). Cases with pT4b were only included in the early period, and the prognosis was the poorest among the Borrmann type IV gastric cancer cases. Cases with P1 also showed dismal prognosis, however, the prognosis was slightly better than for those with pT4b, and similar to that for patients with pT4aP0 in the early period (Figure 6a). On the other hand, cases with pT1-3P0 exhibited better prognosis than those with P1 or pT4aP0.
Such prognostic stratification was maintained even in the late stage, where prognosis is robustly improved (Figure 6b). In the late-treatment period, cases with pT1-3P0, pT4aP0, or P1 showed much better prognosis than the corresponding prognosis in the early period (Figure 6b). Five-year OS was greater than 30% in cases with pT4aP0 or P1 in the late-treatment period.
Clinical characteristics of long-term survivors (more than three years) of Borrmann type IV gastric cancer. We then explored patients who survived more than three years after surgery in the late period, and identified 19 patients (34.5%) as shown in Table III. Among these 19 patients, there were 8 cancer-free patients (14.5%), 1 of whom was with CY1 and administered with S-1 for 5 years. The 11 patients with cancer progression included six cases whose deaths were related to gastric cancer progression, and five cases who remain fighting their disease. Cancer-free patients were ultimately not as frequent as we had expected from the survival curve of the 5-year OS.
Discussion
In the present study, we performed multivariate prognostic analysis of Borrmann type IV gastric cancer, and identified the period, T factor, P factor, and age as independent prognostic factors. There has been no report which performed multivariate prognostic analysis including these four factors simultaneously in Borrmann type IV gastric cancer (13, 20, 21). The reason for the prognostic difference between the early and late periods may be due to various clinical factors. First of all, as the main reason, we focused on the fact that there was no case of pT4b in the late period, while a considerable number of patients with pT4b were included in the early period. Certainly, pT4b cases exhibited dismal prognosis, and they did not seem to be indicative for surgery from a prognostic point of view, however, the prognosis of patients with Borrmann type IV gastric cancer in the early period was almost similar with that of patients when excluding pT4b. Hence, improvement of prognosis in the late period may be due to causes other than inclusion of pT4b cases. Secondly, we suspected a difference in treatment strategies, hence the background distribution was compared in Table I. As a result, significant differences were found in pT, cytology, margin status, and preoperative chemotherapy between the early and late periods.
Clinicopathological features between early and recent cases.
In terms of pT, there was no different distribution when pT4b was excluded. In the context of cytology, there was little information in the early period, while cytological test was almost routinely performed in the late period, starting in 2000 in accordance with the 13th Japanese Classification of Gastric Cancer. Intriguingly, CYX cases exhibited a similar prognosis to those of CY1. As CYX was largely attributed to the early period, a large portion of cases with CYX in the early period might in fact have been CY1. We also observed the significantly different distribution of margin status, which could be explained by prevalence of preoperative chemotherapy. Preoperative chemotherapy was never performed in the early period, hence we believe this difference may be due to unique types of therapeutic options used in the late period, while the therapeutic efficacy remains to be clarified from a prognostic point of view in Japan. Routine performance of postoperative administration of S-1 is also characteristic of the late period, and there were several cases with postoperative administration of S-1 of over two years in type IV gastric cancer. Namely, multi-modality treatment could contribute to improved OS of patients with type IV gastric cancer.
NAC with S-1 was not proven to be effective for improving OS of patients with Borrmann type IV gastric cancer compared to the historical controls in JCOG0002 phase II clinical trials (6). On the other hand, NAC CDDP/S1 (CS) in the JCOG0210 phase II clinical trial has been completed, and the subsequent clinical trials are ongoing to test the hypothesis that CS is superior to the standard treatment for Borrmann type IV and large type III gastric cancer in the JCOG0501 phase III clinical trials (14). The former led to 35-40% of 3-year OS (18/55: 33% was stage IV), while the latter to about 25% (24/47: 51% was stage IV). In our current study including at least 20 stage IV cases (~36%), survival outcome of the late period was better as compared to that in the early period. Long-term survivors (over three years) totalled 19 patients out of the 55 surviving cases, and eight cases were cancer-free for over three years (14.5%). However, these eight cancer-free patients included only two patients who had NAC of S-1 (n=1) and Docetaxel/CDDP/S1 (DCS) and Docetaxel/S1 (DS) (n=1). On the other hand, there were 11 long-term survivors with a cancer burdens, among whom a considerable number (4/11: 36.3%) underwent DCS NAC, suggesting that DCS NAC can prolong survival; its efficacy for improved curability remains undetermined.
From 2007, when survival benefits of S-1 were published by ACTS-GC (3), postoperative adjuvant therapy with S-1 was routinely applied to patients with pathological stage II/III advanced gastric cancer as a standard treatment, almost all long-term survivor underwent postoperative adjuvant chemotherapy of S-1. Among them, cases 1, 6, and 8 (Table III) underwent S-1 for over 3 years, and case 8 was the patient with CY1 to whom S-1 had been administered for about five years and who remained free of cancer. There was a report which claimed that 2-year administration is superior in prognosis to 1-year administration for stage II/III gastric cancer (15), suggesting that long-term chemotherapy administration might rescue patients with minimally-residual disease of Borrmann type IV gastric cancer.
Univariate and multivariate prognostic analysis for overall survival (OS) in type IV gastric cancer.
The current study also had several limitations: survival data were collected long-term over a period of 43 years, so there was heterogeneous distribution of surgical indication, clinical diagnosis, surgical diagnosis including cytology test, hence we cannot accurately determine even pathological stage. In the early period, there were many cases with D3 lymph node dissection, but D1 lymph node dissection was actively selected for CY1 cases in the transition period; consequently, lymph node dissection level was hetero geneous. In the late period, among the 55 cases, 32 underwent D2 lymph node dissection, and 13 underwent D1+ lymph node dissection, meaning that operations aimed to complete R0 resection. As Borrmann type IV gastric cancer usually recurred in the peritoneum, not in the lymph nodes, there was no consensus for lymph node dissection range, especially for CY1 or P cases.
In conclusion, the prognostic analysis of the Borrmann type IV gastric cancer showed that: i) T4b cases represent the most dismal prognosis in type IV gastric cancer, consequently there is no active indication for surgery at present; ii) important prognostic factors were pT and P factors, both of which could be down-staged by potent NAC. Recent improvement of prognosis of Borrmann the type IV gastric cancer may be due to application of such potent NAC as DCS before surgery and postoperative long-term chemotherapy of S-1. If future novel multimodality treatment can further down-stage pT and P factors preoperatively/postoperatively, such therapies would improve prognosis of patients with Borrmann type IV gastric cancer in combination with surgery.
Clinical characteristics of long-term survivors (more than three years) of type IV gastric cancer.
- Received September 25, 2014.
- Revision received October 27, 2014.
- Accepted November 4, 2014.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved