

Abstract
Aim: Leukoplakias (LPLs) are lesions in the oral mucosa that have a potential to transform into oral squamous cell carcinoma (OSCC). As the degree of immunosurveillance may be important for this transformation to occur, the aim of this study was to determine the presence of immune cells in LPLs with dysplasia in relation to later development of OSCC. Materials and Methods: Biopsies from 16 patients with clinical diagnosis of LPL and histopathological diagnosis of hyperkeratosis with dysplasia were immunostained with antibodies to detect CD3+ T cells, CD1a+ LCs, Ki-67+ and p53-expressing cells. Patients were divided into two groups: LPL with dysplasia that transformed into OSCC (LPL-dys) and that which did not (LPL-ca). Results: Quantitative analyses showed significantly lower numbers of CD3+ T-cells in LPL-ca than in LPL-dys. No significant differences were detected when comparing LPL-dys and LPL-ca regarding CD1a+, p53+ and Ki-67+ cells. Conclusion: The number of CD3-expressing T-cells may be important for preventing malignant transformation of LPL.
- Premalignant leukoplakia
- oral cancer
- immunosurveillance
- biomolecular markers
Leukoplakia (LPL) (Figure 1A) is a potentially premalignant disorder in the oral mucosa (1). Approximately 3%-17% of LPLs transform into oral squamous cell carcinoma (OSCC) (Figure 1B) and the annual transformation rate is estimated at approximately 1% (2, 3). The risk of malignant transformation of LPL is difficult to predict. Several studies have attempted to identify potential biomarkers that could predict disease aggressiveness and clinical outcome. However, no diagnostic or treatment modalities are currently at hand that can prevent LPLs transforming into OSCC (4, 5). Hence, most clinicians arbitrarily regard the clinical diagnosis, size and severity of cell dysplasia to be proportional to the risk of malignant transformation.
During the last decades several studies have been carried out addressing the importance of the immune system and prognosis of cancer (6-8). The concept of cancer immunoediting has resulted in a view of dynamic interaction between the immune system and dysplastic cells/tumor cells, with phases of elimination, equilibrium and escape (9). Thus, in an early phase of cell dysplasia or early tumor cell formation the immune system has the capacity to eliminate cells with DNA damage that may result in, or already have resulted in, cancer (10). Immunoediting is probably of importance in the defence against malignant cells that may occur in LPL. The importance of immune activation in the defence against tumors in the head-neck region was observed in the 1970s when tumor-infiltrating T-cells were found to correlate to prognosis in OSCC (11). Since the initial reports on the importance of T-cells in tumor progression, further evidence has been provided regarding the role of T-cells and other leukocytes in antitumoral defence and correlation to treatment outcome (7, 12, 13).
Activation of T-cells demands interaction with other leukocyte subsets. Dendritic cells (DCs) are effective initiators of naive T-cells and can generate effector T-cells with the capacity to eliminate tumor cells (14). DCs engulf, process and present tumor-associated antigens (TAAs) to naive or memory T-cells (15). Depending on the TAA-presenting pathway, tumor-specific cytotoxic T-cells may be generated (16). Dendritic Langerhans cells (LCs) are a subset of DCs present in skin and mucosal linings, providing immunosurveillance to these tissue compartments (15). In the oral mucosa, an important role of LCs in evoking antitumoral response may be expected, although no definite proofs have been provided.

Leukoplakia on the right border of the tongue (A). The area was excised but 18 months later a squamous cell carcinoma appeared in the region (B).
A number of clinical and experimental studies have investigated T-cell response in established tumor diseases (reviewed in (17)) but immune response in oral premalignant lesions has not yet been extensively studied. The concept of cancer immunoediting implicates that an immune response may be mounted already in the premalignant phase, when cells of the immune system recognize dysplastic cells.
In premalignant disorders, such as LPL, mechanisms affecting both cell proliferation pathways and pathways involving growth factors have been investigated in the pursuit of a reliable biomarker foreseeing malignant transformation (18). Increase of p53 expression in LPL has been reported to correlate with a higher degree of malignant transformation in LPL (19).
Indices using the proliferation marker Ki-67 have also been extensively studied and proposed as a predictor of malignant transformation of LPL (19, 20). Altered intracellular signalling results in alterations in cell surface molecules and release of molecules recognized by cells of the immune system (17). A linkage between molecular markers like p53 and Ki-67 and immune response is likely to exist, leading to interest in expression of these biomarkers in the context of immune activation (21).
Our hypothesis is that recruitment of T-cells and DCs may prevent malignant transformation in LPL with cell dysplasia. Thus, the aim of this study was to compare the presence and distribution of T-cells and dendritic Langerhans cells in a group of LPL patients with no OSCC transformation and an OSCC-transforming group.
Patients and Methods
Patients. Biopsy specimens from 11 patients (LPL-dys) with a clinical diagnosis of LPL and a histopathological diagnosis of hyperkeratosis with dysplasia and no record of malignant transformation during follow-up were retrospectively retrieved from the archives of the Department of Oral Medicine and Pathology, University of Gothenburg. In parallel, 11 patients (LPL-ca) with a clinical diagnosis of LPL and a histopathological diagnosis of hyperkeratosis with dysplasia that transformed into OSCC, according to patients' records, were retrieved from the same archives, yielding a total cohort of 22 patients. The biopsies were formalin-fixed and paraffin-embedded specimens obtained between 1987 and 2003. Biopsies were reviewed in a blind manner and independently by two senior pathologists. One patient in the LPL-dys group and one patient in the LPL-ca group – initially judged as hyperkeratosis with dysplasia – were ascribed an early OSCC diagnosis. These patients were excluded from further analysis, leaving 10 patients in each group. Further on in this review, it was found that two patients in the LPL-dys group showed signs of fungal infection within epithelium and two patients in the LPL-ca group had received an OSCC diagnosis, according to hospital records, within a month of primary biopsy. Those patients were excluded from analysis. In total, 16 patients, 8 patients in each group, proceeded to final analysis. Patient characteristics are described in Table I.
Follow-up periods for patients. In the LPL-dys group patients were monitored for a median time period of 95 months (range=21–159) without developing OSCC (Table I). Corresponding data for the LPL-ca group revealed a median period of 62 months (range=7-192) before transformation into OSCC occurred (Table I).
The Ethical Review Board at the Sahlgrenska Academy, University of Gothenburg, approved the study and all patients signed an informed consent before being included in the study.
Immunohistochemistry. Sections from paraffin-embedded biopsies were retrieved and immunohistochemical staining was performed to describe the presence and phenotype type of cells in tissue specimens.
Antibodies. Monoclonal antibodies raised against CD3 (LN10; Novocastra, Newcastle, UK), CD1a (010; Dako A/S, Glostrup, Denmark), p53 (D07; DAKO A/S) and Ki-67 (MIB-1; Dako A/S) were used.
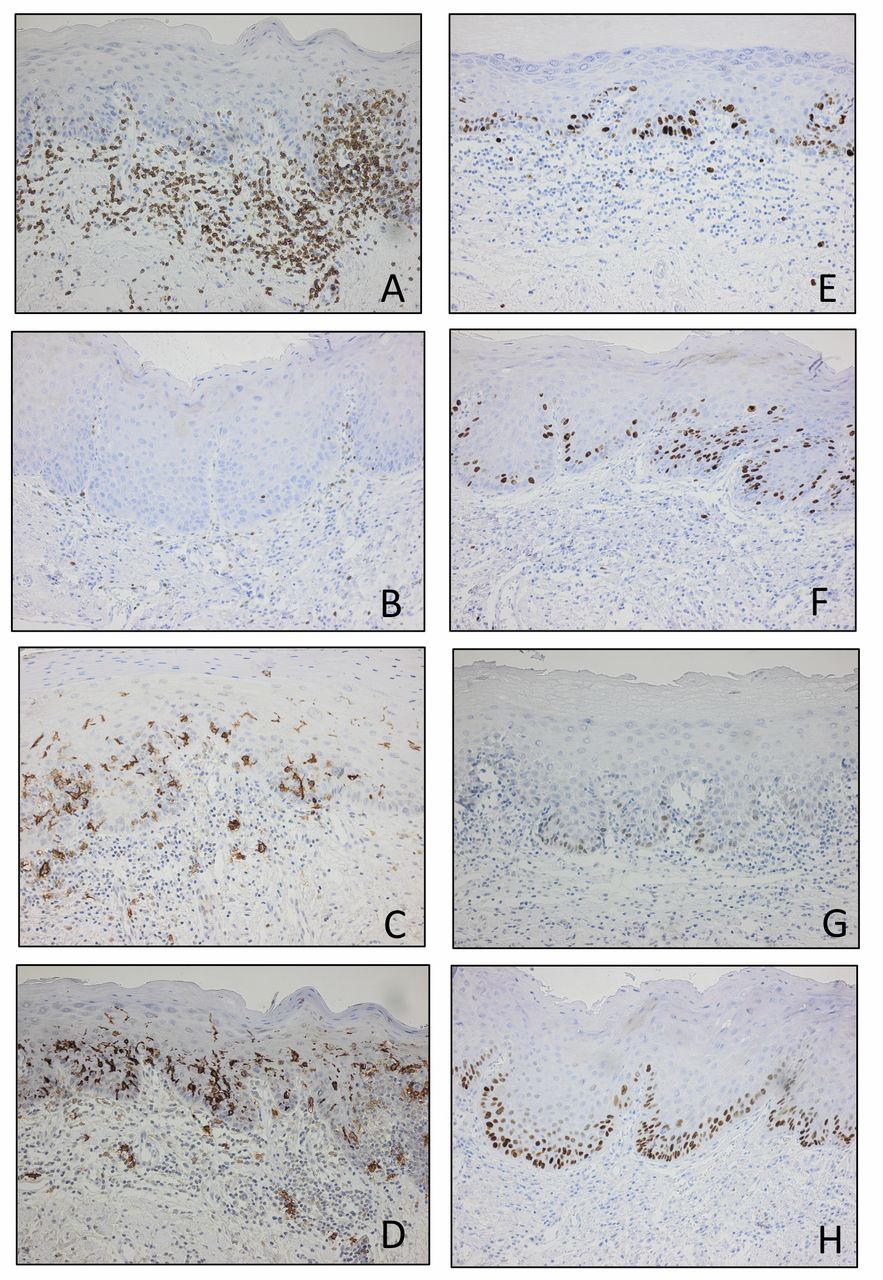
CD3-positive T-cells in (A) leukoplakia without malignant transformation and (B) leukoplakia with malignant transformation. CD1a-positive LCs in (C) leukoplakia without malignant transformation and (D) leukoplakia with malignant transformation. Ki67-positive cells in (E) leukoplakia without malignant transformation and (F) leukoplakia with malignant transformation. p53-positive cells in (G) leukoplakia without malignant transformation and (H) leukoplakia with malignant transformation. Positive cells stain brown. Magnification ×200.
Blocks of paraffin-embedded biopsies were cut into 4 μm-thick sections. The sections were then mounted on electrostatically precharged slides (Superfrost Plus; Menzel-Gläzer, Frankfurt, Germany), deparaffinized, and rehydrated. Antigen retrieval was carried out using TRIS /EDTA pH 9.0 and microwave treatment for 20 min. After cooling at room temperature (RT), the slides were rinsed in phosphate-buffered saline (PBS).

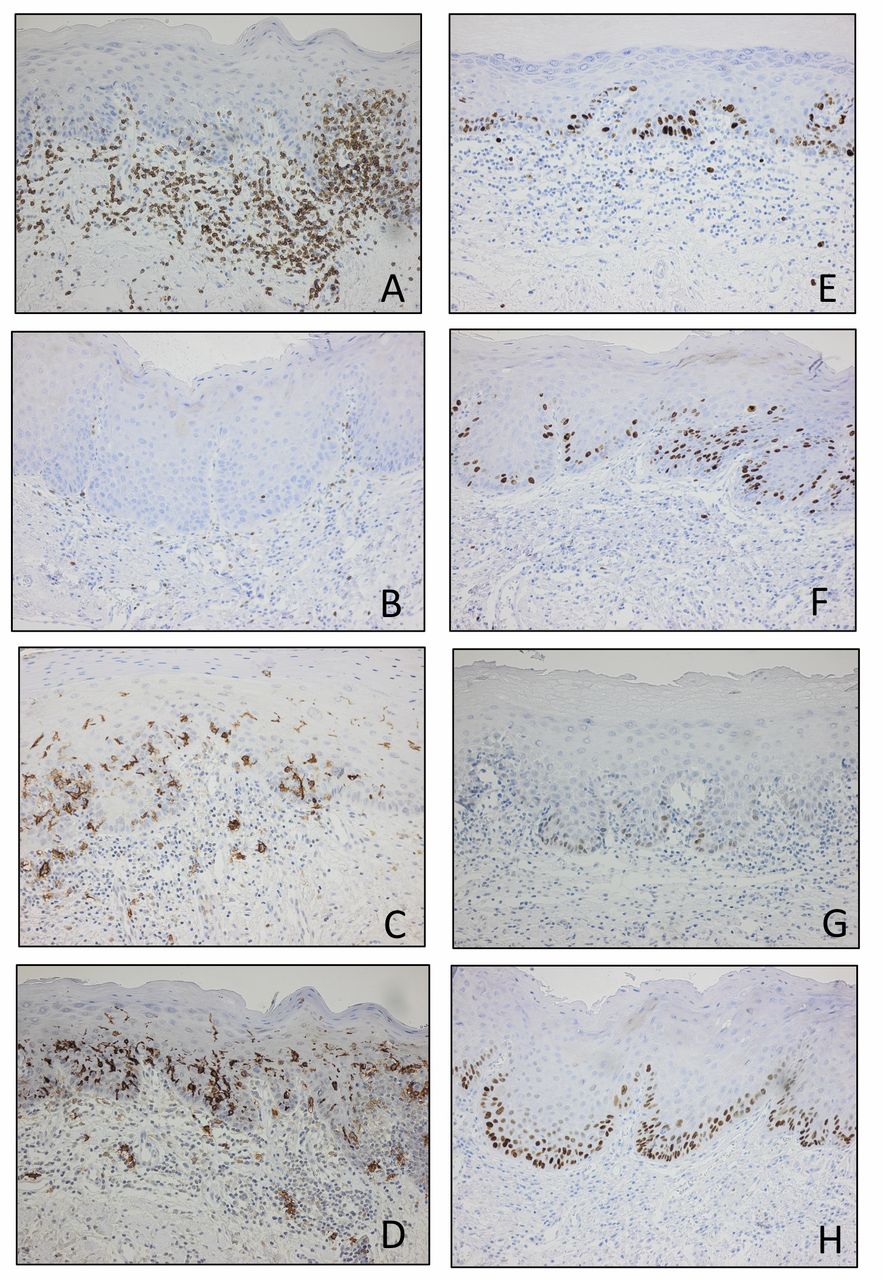
CD3-positive T-cells in epithelium of (A) leukoplakia without transformation (solid circles) and leukoplakia with malignant transformation (open circles), and CD3-positive T-cells in connective tissue of leukoplakia without malignant transformation (triangles) and leukoplakia with malignant transformation (inverted triangles). (B) CD1a-positive LCs in epithelium of leukoplakia without malignant transformation (solid circles) and leukoplakia with malignant transformation (open circles), and CD1a-positive LCs in connective tissue of leukoplakia without malignant transformation (triangles) and leukoplakia with malignant transformation (inverted triangles).
The sections were incubated with a primary antibody for 25 min at RT. All subsequent washings were performed with the ChemMate Buffer kit (K5006; Dako A/S). After blocking of endogenous peroxidase using the ChemMate Peroxidase-Blocking Solution (S 2023; Dako A/S), the sections were incubated with the ChemMate DAKO EnVision Detection Kit, Peroxidase/DAB, Rabbit/Mouse (K5007; Dako A/S) for 25 min at RT and developed with DAB substrate. Counterstaining with ChemMate Haematoxylin S2020 (Dako A/S) was followed by dehydration in ethanol/xylene. Mountex (Histolab AB, Gothenburg, Sweden) was used to permanently mount slides. Sections from tonsils served as positive controls, while omission of primary antibodies served as negative controls.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
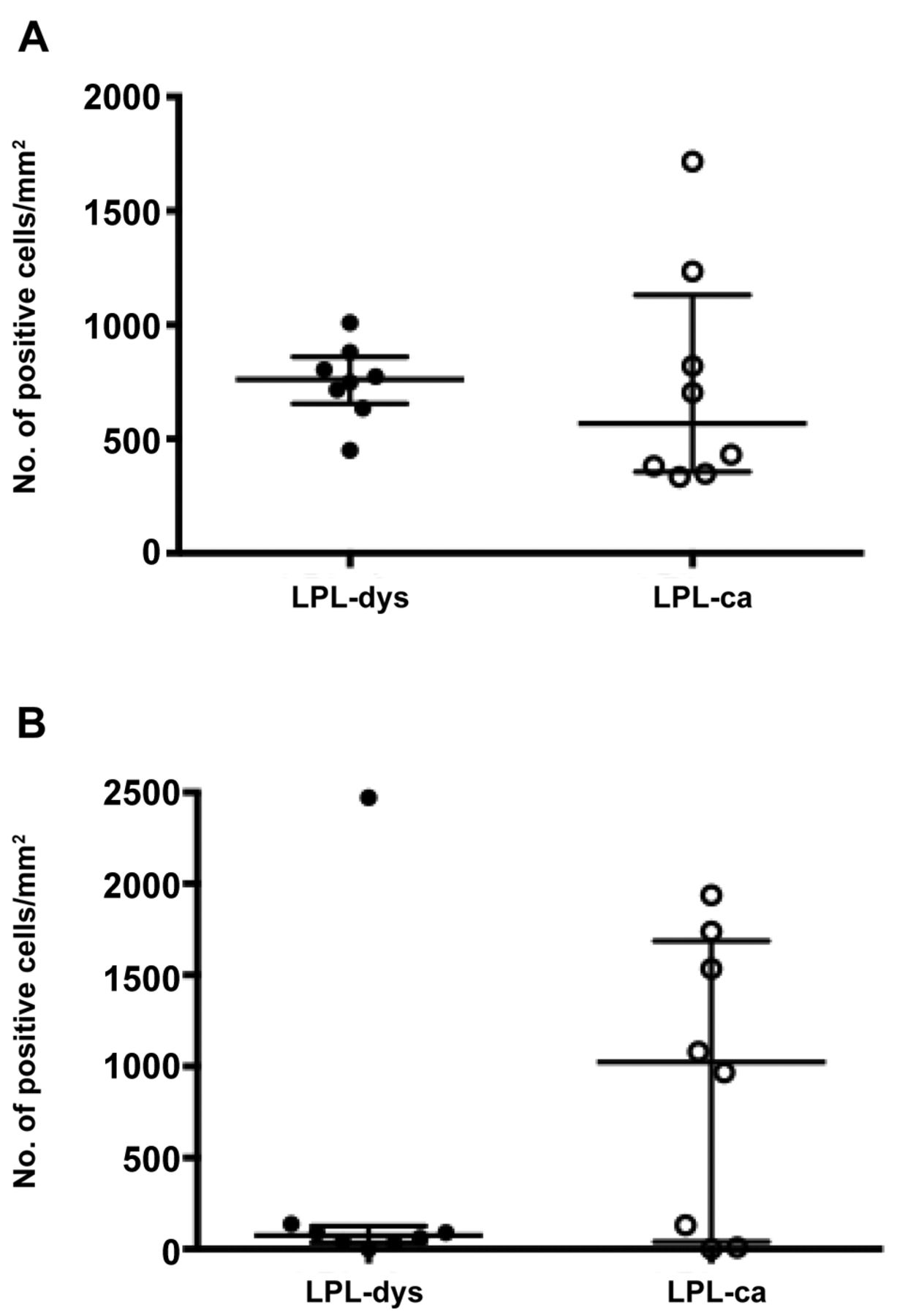
Ki67-positive cells in epithelium of (A) leukoplakia without malignant transformation (solid circles) and leukoplakia with malignant transformation (open circles), and p53-positive cells in epithelium of (B) leukoplakia without malignant transformation (solid circles) and leukoplakia with malignant transformation (open circles).
Quantitative analysis. Two compartments per biopsy, the epithelium and the connective tissue, were selected for quantitative analysis. Digitalized images of sections, where epithelium showed dysplasia and corresponding connective tissue compartment, were obtained with a light microscope (Leitz Wetzlar, Leica Microsystems, Wetzlar, Germany) and digital camera (UC30; Olympus, Microsystem, Norcross, GA, USA). One to six fields, depending on biopsy quality, with epithelial dysplasia were photographed at magnification ×63 (CD1a, p53, Ki-67, p53) or at magnification ×100 (CD3). For all antibodies, sections were analysed with computer software (CellSense; Olympus, Hamburg, Germany). Positively stained nucleated cells were counted and results were expressed as the number of positively stained cells / mm2. Cell counting was performed blinded by one observer, after calibration with two other observers.
Statistical analysis. Analyses of differences between groups were performed using the Mann–Whitney U-test, with the statistical software SPSS v17 (SPSS Inc., Chicago, IL, USA). A p-value <0.05 was considered as a significant difference.
Results
T-cells. T-cells were mainly seen in stratum basale and stratum spinosum of the epithelium. In the connective tissue, T cells formed a subepithelial infiltrate in close relation to the epithelial basal cell layer (Figure 2A and 2B). The number of CD3-positive cells per area unit was significantly higher in the LPL-dys group compared to the LPL-ca group, in both the epithelium and the connective tissue (Figure 3A; p=0.016 and p=0.016, respectively)
Langerhans cells. CD1a-positive LCs were found predominately in the epithelium but also in the connective tissue, mostly scattered in the T cell infiltrate (Figure 2C and 2D). No significant differences between the two groups were found regarding the number of LCs in either the epithelium or connective tissue (Figure 3B; p=0.630 and p=0.248).
Ki-67. The proliferation marker Ki-67 was present on cells in both epithelium and connective tissue in both LPL-dys and LPL-ca, though in higher amounts in the epithelium than in the connective tissue (Figure 2E and 2F). No statistically significant difference was found between the number of proliferating cells in LPL-dys and LPL-ca (Figure 4A; p=0.277).
p53. p53 was predominantly found in epithelium, while its presence in connective tissue was rare (Figure 2G and 2H). There was no significant difference in p53 expression when comparing epithelium between the two groups (Figure 4B; p=0.277).
Discussion
The main finding of this study is that a group of patients with dysplastic LPL and no subsequent malignant transformation had presence of significantly more T cells compared to a group with LPL with dysplasia that later on transformed into OSCC.
Tumor-infiltrating T-cells are important effector cells in inhibiting tumor development. A “friend or foe” relation exists as subsets of infiltrating T cells can guide disease progression into different directions. CD8-positive and CD4-positive T-cells without regulatory phenotype have been shown to improve prognosis (22). On the other hand, presence of CD4+CD25+ regulatory T cells is associated with impaired disease control (23). Recently, myeloid-derived suppressor cells and M2 macrophages have also been ascribed a role in down-regulating an effective anti-tumoral immune response (24).
The concept of immunoediting originally proposed by Dunn et al., with phases of elimination, equilibrium and escape (10), is well in line with the present state of knowledge regarding immune activation and antitumoral defence. Another important observation supporting the influence of immunosurveillance in antitumoral defence is that several studies report a dramatic increase in certain types of tumors in solid organ–transplanted patients receiving continuous immunosuppression (25, 26).
Patients' characteristics.
The bulk of knowledge accumulated during the last decades has been almost exclusively gained in studies on established tumors (13, 27-29). Less is known about immune activation in premalignant disorders. In an earlier study we reported that T-cells and dendritic Langerhans cells (LCs) respond to cell dysplasia in LPLs (30), providing evidence for immunosurveillance in this premalignant disorder.
In the present study we analyzed two groups of patients with LPL with different clinical outcome, one group of patients in which LPL developed into OSCC at the site of initial lesions and one group where LPL did not transform into OSCC during the observation period. In the group where the patients did develop OSCC, significantly fewer CD3-positive T-cells were registered, both in dysplastic epithelium and the subepithelial connective tissue, in comparison with patients that did not develop OSCC. Although the number of patients analysed in this study is limited, a difference in the presence of T-cells between non-OSCC-transforming and OSCC-transforming patients with LPL was registered. This finding lends further support to the immunosurveillance hypothesis, although we have not characterized the T-cell subsets. So far, most studies have emphasized the importance of presence of CD8-positive cytotoxic T-cells in antitumoral defence but in a recent study by Badoual (31) the presence of activated CD4-positive T cells was found to have an influence on patients' survival in head and neck tumors. Composition of the T cell infiltrate and OSCC transformation needs to be addressed in a prospective manner.
DCs are important effector cells in antitumoral defence (32). The LC subset has been investigated less. In an earlier report from our group comparing LPL with and without dysplasia, LCs were found to be more numerous in the dysplasia group, indicating an ongoing immune response (30). In this study, where all patients with LPL had dysplastic changes in biopsy specimens, no significant difference could be seen between the OSCC-transforming and non-OSCC-transforming groups. This result does not exclude the importance of DCs in the immunosurveillance process in LPL. Other subsets of DCs, not investigated in the present study, such as plasmocytoid DCs, possess a potent antitumoral capacity (33) and may be involved in orchestrating the antitumoral immune response in LPL.
In our patient cohort gender distribution differed between the groups. There was a dominance of men in the LPL-ca group, while women dominated in the LPL-dys group. In a study by Ho et al. no gender difference in hazard ratios for OSCC transformation from LPL with dysplasia between males and females could be registered (34). However, gender differences in environmental factors, such as smoking, may influence the outcome. The present patients' material is relatively small to interpret the influence of gender on the results but it is an issue that should be addressed prospectively.
An increased cell proliferation is associated with worse prognosis amongst patients with head and neck tumors (35). The proliferation marker Ki-67 has been used for decades in clinical and scientific settings. In oral leukoplakias, Vered and co-workers have presented evidence for a correlation with degree of dysplasia, malignant transformation and Ki-67 expression (19). Another group has reported a correlation between degree of dysplasia and Ki-67 expression (20). In contrast, Torres-Rendon et al. could not detect any correlation between Ki-67 expression and degree of dysplasia, although the study showed correlation when a co-labelling index with maspin was applied (36). In our patient groups no significant correlation was detected, which supports the findings by the aforementioned study.
In oral premalignant disorders, the expression of p53-positive cells in the suprabasal layers of the epithelium has been suggested as an indicator for malignant transformation (37). In a study by Angiero et al., a high expression of p53 was seen in epithelium with increasing dysplasia (38). In another study, an increased epithelial expression of p53 in OSCC was observed in comparison to normal mucosa. This study did not show any difference in p53 expression in epithelium between patients that developed OSCC from leukoplakia and patients who did not. However, the presence of p53 molecules in LPL epithelium reinforces the existence of an ongoing abnormal process, demanding DNA repair in accordance with what Hanahan and Weinberg propose (39).
In conclusion, the finding of the present study, increased number of T-cells in non-OSCC-transforming LPL compared to OSCC-transforming LPL, lends further to support the importance of an immunomediated antitumoral defence system. The findings should be further investigated in a prospective manner.
Acknowledgements
This study was supported by the Agreement for Doctoral Education, Region Västra Götaland, Sweden, the Assar Gabrielsson Foundation, the Swedish Dental Society, and the Gothenburg Dental Society. The authors are obliged to Ms. Christina Eklund, BSc and Ms. Marie Svensson for valuable assistance in laboratory procedures.
Footnotes
-
This article is freely accessible online.
-
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received August 28, 2014.
- Revision received September 9, 2014.
- Accepted September 15, 2014.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved