

Abstract
Background: One third of non-small cell lung cancer (NSCLC) affects elderly patients in a locally advanced (LA) stage. Induction therapy followed by a curative approach is becoming the standard-of-care for LA-NSCLC. Patients and Methods: We compared the efficacy and tolerance to induction chemotherapy or chemo-radiation followed by surgery or definitive radiotherapy in patients younger (N=64) and older (N=44) than 70 years with LA-NSCLC. Results: Elderly patients trended towards having a worse baseline performance status, and presented a higher percentage of IIIB, and squamous tumors. Nevertheless, no significant differences in response rate, operability, or disease-free and overall survival were found between age groups in the whole series, nor in the sub-group of resected patients. Grade 3-4 toxicity tended to be lower in elderly patients. Conclusion: Age by itself did not significantly worsen either the efficacy or tolerance to combined induction and definitive treatment in patients with LA-NSCLC and Eastern Cooperative Oncology Group performance status 0-2.
- Chemoradiation
- chemotherapy
- elderly patients
- induction treatment
- locally advanced
- non-small cell lung cancer
Almost one third of non-small cell lung carcinomas (NSCLC) are diagnosed beyond the seventh decade of life and at a locally advanced (LA) stage. Combinations of chemotherapy, radiotherapy, and surgery obtain 9-36% five-year overall survival (OS), and induction followed by consolidation therapy are becoming the standard of care for LA-NSCLC because it provides the same 5-7% benefit for OS as adjuvant treatment; it increases the rate of microscopically complete resections; it tests the efficacy of treatment in vivo providing prognostic information; and increases the therapeutic fulfillment (1).
Elderly patients have historically not been considered for induction treatment, but this attitude is changing. We analyzed the impact of age on the efficacy and tolerance to induction chemotherapy or chemoradiation (IT) followed by surgery or definitive radiotherapy in LA-NSCLC.
Patients and Methods
Six-hundred cases of NSCLC were diagnosed at our Center from October 2005 to June 2012. One hundred and eight consecutive histologically-confirmed patients with LA-NSCLC aged ≥18 years, with Eastern Cooperative Oncology Group performance status (ECOG) 0-2 and baseline clinically T3-4 or N2-3 tumors (supraclavicular involvement or malignant pleural effusion were excluded) were treated with IT, and planned for surgery or consolidation radiotherapy to 60-70 Gy after re-staging at the end of induction. Age by itself defined neither IT nor consolidation treatment, which were decided by our Thoracic Malignancy Board accordingly to stage, performance status, comorbidity, and functional test of each patient.
Follow-up and clinical charts were retrospectively reviewed. We compared the feasibility, tolerance, and efficacy of IT followed by surgery or radiotherapy in patients with LA-NSCLC younger and older than 70 years. The assignment of 70 years as a cut-off to define elderly patients was arbitrary, but is commonly used in literature (2-4).
Tumor response was assessed by combining RECIST-1.1 criteria (5) for computed tomography scan, uptake changes in positron-emission tomography, and pathology of resected specimens. Staging and toxicity were graded according to the seventh TNM classification (6) and to the NCI Common Toxicity Criteria version-3.0 (7), respectively. Statistical analyses were performed using SPSS-21 (IBM Corporate, Armonk, New York, USA) software. Differences between age groups were compared by UNIANOVA test for a 95% confident interval, assuming statistical significance for p≤0.05. OS and disease-free survival (DFS) were analyzed by Kaplan–Meier curves. Survival differences between age groups were analyzed by Mantel–Cox test.
Results
The mean age of the series was 66.7 years (range=47-84 years). Sixty-four patients were younger than 70 years, and 44 were 70 years or older, including four octogenarian patients. From this point, results will be referred to comparing younger versus elderly patients.
Women represented 7.4% of cases (7.82% vs. 6.82%; p=0.848). There were no significant differences in smoking habit, baseline performance status (ECOG 0: 92.18% vs. 77.2%; ECOG 1: 7.81% vs. 20.45%; p=0.088), baseline respiratory tests, histology (squamous carcinoma: 67.18% vs. 79.54%; adenocarcinoma: 15.62% vs. 6.81%), or baseline clinical stage (stage II: 17.18% vs. 20.45%; stage IIIA: 46.87% vs. 28.54%; stage IIIB: 35.93% vs. 50%) between age groups.
Treatment strategy was the following: 24 patients were treated with induction chemoradiation plus surgery (26.56% vs. 15.9%); 36 with induction chemoradiation plus radiotherapy (32.81% vs. 34.09%); 31 with induction chemotherapy plus surgery (26.56% vs. 31.81%); and 17 with induction chemotherapy plus radiotherapy (14.06% vs. 18.18%). Disease in five patients (one from the younger and four from the elderly group) treated with induction chemotherapy progressed to stage IV and therefore did not undergo consolidation therapy.
All the patients received platinum-based chemotherapy (carboplatin plus taxanes: 14.06% vs. 20.45%; carboplatin plus vinorelbine or gemcitabine: 1.56% vs. 13.63%; cisplatin plus taxanes: 21.87% vs. 6.81%; and cisplatin plus vinorelbine or gemcitabine: 62.5% vs. 45.45%), with a mean number of cycles of 3.78 vs. 4.06, respectively. Carboplatin-based regimens were more commonly applied to elderly patients (15.6% vs. 34.1%; p=0.025), and six (13.63%) elderly patients received carboplatin monotherapy. Radiotherapy was administered to the primary tumor and mediastinum. Radiation doses ranged from 33 to 66 Gy, with a mean of 54.97 Gy (54.57 vs. 55.6 Gy).
There were no significant differences between groups in radiological or metabolic response to IT (progression: 1.56% vs. 6.81% and 4.68% vs. 9.09%; stabilization: 29.68% vs. 27.27% and 48.43% vs. 36.63%; partial response: 64.06% vs. 61.36% and 14.06% vs. 19.18%; and complete response: 4.68% vs. 4.54% and 32.81% vs. 35%; p=0.723 and p=0.323, respectively). Grade 3-4 toxicity while on IT tended to be more frequent in younger patients (20.3% vs. 6.8%, p=0.053), especially regarding neutropenia (18.75% vs. 6.81%). Grade 3-4 esophagitis was uncommon in both age groups (1.56% vs. 2.27%), and no relevant pneumonitis was observed.
Surgery was performed in 50 patients (51.56% vs. 50%), and included pneumonectomy (17.18% vs. 9.09%), bi/lobectomy (29.68% vs. 20.45%), and sublobar resection (4.68% vs. 9.09%). Mediastinal lymph-node dissection was performed in 90% of cases (90.9% vs. 88.23%). Two patients from the younger and one from the elderly group died due to surgical complications within 60 days of resection. There were no significant differences between age groups in the pathological stage (stage 0: 9.37% vs. 6.81%; stage I: 25% vs. 27.27%; stage II: 15.62% vs. 4.54%; stage III: 1.56% vs. 0). Over 30% of patients achieved a major pathological response (34.37% vs. 34.08%). Adjuvant treatments were not administered.
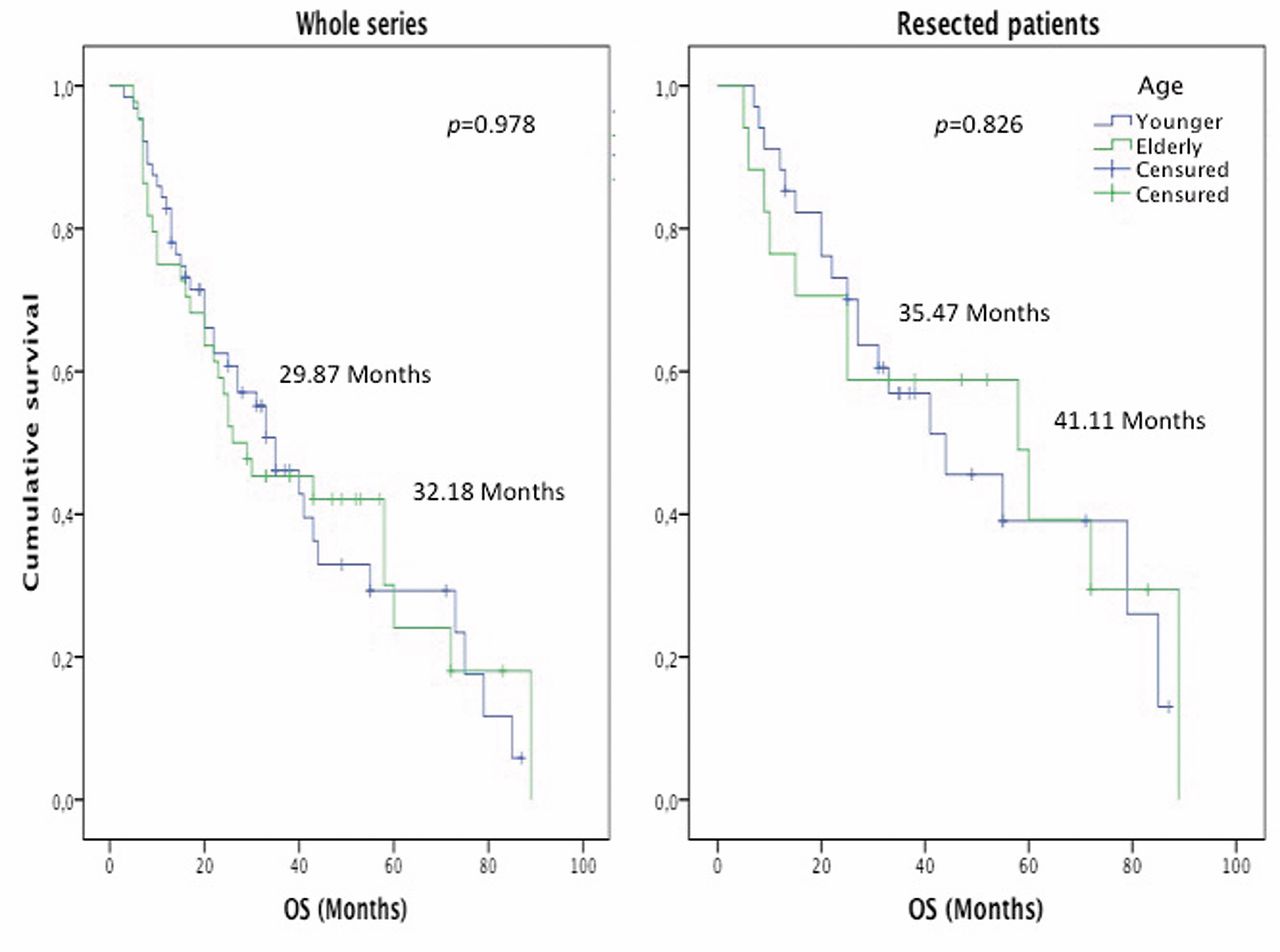
At the time of the analysis, 20 patients presented distant recurrence, 42 local recurrence or progression, and 46 no relapse or progression. The mean DFS of the series was 19.68 months (19.76 months if patients progressing while on IT were excluded), without differences in DFS between age groups in the whole series (18.18 vs. 19.81 months; p=0.642) or among resected patients (27.29 vs. 27.94 months; p=0.924). The mean OS was 30.81 months, without differences in OS between groups in the whole series (29.87 vs. 32.18 months; p=0.978) or among resected patients (35.47 vs. 41.11 months; p=0.826).
Discussion
Classic studies exploring IT in elderly patents with LA-NSCLC were biased by an under-recruitment of elderly patients in prospective trials, and by an overselection of the fit ones in retrospective analyses (8, 9). Our series, entirely composed of daily assisted patients, confirms more recent publications reporting that age does not modify feasibility or efficacy of IT. Regardless of age, we equally considered any consecutively attending young or elderly patient with LA-NSCLC and ECOG 0-2 to receive IT followed by surgery or consolidation radiotherapy. The similar proportion of resected patients in our age groups is proof of that.
Accordingly, there was no overselection of fit elderly patients. Patients with ECOG 2 were admitted to treatment, and our elderly group tended to present a higher proportion of unfavorable prognostic factors, such as current smoking, stage IIIB tumor, and squamous histology, than the younger one. Nevertheless, the rate of operability and radiological, metabolic, and pathological response after IT were similar in both age groups. Patient outcome was similar too, and both DFS and OS were even slightly better among elderly patients.
In regard to tolerance, trials in early and advanced NSCLC reported a slightly worse tolerance to chemotherapy in elderly patients (2, 8-11) that could be minimized with closer surveillance and using less toxic regimens such as carboplatin doublets or carboplatin and taxane monotherapy (11). In our series, elderly patients (more commonly treated with carboplatin-doublets or monotherapy) presented a good tolerance without a loss in efficacy. They even received a slightly higher number of cycles with a smoothly better tolerance than younger patients, confirming that no systematic reduction of chemotherapy doses or cycles are necessary for elderly patients (2).
Both sequential and concurrent chemoradiation are feasible and active as IT or radical treatments for elderly patients with LA-NSCLC (12, 13). Sequential chemoradiation is preferred for unfit patients or those treated with induction chemotherapy that finally cannot be resected. Concurrent chemoradiation is more effective (14) but increases the incidence of esophagitis, and pneumonitis to 29.8% and 1.9%, respectively (15, 16). The incidence of grade 3-4 esophagitis in our series was low in both age groups (1.56% vs. 2.27%), and no grade 3-4 pneumonitis was observed even in those undergoing concurrent regimens.

Kaplan–Meier disease-free survival curve according to age in both the whole population and the subgroup of resected patients.

{kind=link}
{kind=link}
Kaplan–Meier overall survival curve according to age in both the whole population and the subgroup of resected patients.
Tolerance to surgery in elderly patients with LA-NSCLC is controversial. Some series reported no meaningfully increment in the frequency and intensity of surgical complications (2), meanwhile others showed a tendency to present more and more severe postoperative complications, with a higher early and lately mortality rate (9, 17) (2.2% vs. 3.6%, and 2.5% vs. 4.7%, respectively). In our series, the operability rate was similar in both age groups, and postoperative mortality was limited to two patients from the younger and one from the elderly group even with 9.09% of pneumonectomies. Currently, pneumonectomy after IT is mostly excluded from our protocols.
Conclusion
In our series, age did not worsen the efficacy or tolerance to IT or to the following consolidation therapy. Fit elderly patients with LA-NSCLC are eventual candidates for combined treatments.
Acknowledgements
Authors would like to thank: patients and relatives, whose trust and affection motivate us to improve; co-workers from our Center and from Vall d'Hebron and Bellvitge Hospitals, whose collaboration in our Thoracic Malignancy Board helped to obtain the reported results; and Svetozara Georgieva Hristova for her convenient suggestions about language and style.
Footnotes
-
Preliminary data of this study were presented at the Fourth European Lung Cancer Conference (Geneva, March 2014).
-
Conflicts of Interest
The Authors did not have any conflicts of interest in the redaction of this article.
-
Funding source
No funding sources were used for the development of this work.
- Received April 8, 2014.
- Revision received June 4, 2014.
- Accepted June 5, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved