

Abstract
Background: There are still controversies about the benefit of surgery after concurrent radiochemotherapy (CRT) for locally advanced cervical cancer. The aim of this study was to evaluate toxicity, local tumor control and overall survival of surgery after CRT in stage IB-IIB cervical cancer. Patients and Methods: Between 2002 and 2008, 24 patients with stage IB-IIB cervical cancer were treated with external-beam radiotherapy concomitantly with chemotherapy. High-dose rate brachytherapy fractions were given once weekly. Radical hysterectomy was undertaken after a median of 42 days. Results: Overall survival at five years was estimated at 75% (95% confidence interval=52-88%) and sustained thereafter through to 8.9 years. No patient experienced local failure in the surgical bed. Postoperative complications were recorded in two patients. Conclusion: Surgery after CRT in stage IB-IIB cervical cancer is safe and leads to better local control of the disease and overall survival.
- Cervical cancer
- high-dose-rate brachytherapy
- concomitant chemoradiotherapy
- surgery
Cervical cancer is the second most common cancer in §women worldwide and the leading cause of death among women in developing countries (1). In Croatia, the incidence is 9.2 per 100000, ranking as the eighth most common cancer in women. Croatia has considerably lower cervical cancer incidence compared to surrounding Central and Eastern European countries, and mortality is among the lowest in Europe, estimated as 2.5 per 100,000 women (2). The majority of cervical cancer cases in Croatia are diagnosed at an early stage and are managed surgically, with a 5-year survival of 74% (3).
Cervical carcinoma stages IB2 and IIA according to the 1995 International Federation of Gynecology and Obstetrics system (4), and IIB stage with 1/3 proximal parametrial involvement, according to the Gustave Roussy Institute Staging system (5) are associated with greater rates of treatment failure (5-9). Radiation therapy combined with concurrent chemotherapy, with or without surgery, is considered to be standard treatment for these patients (10-16).
However, very few studies have evaluated the role of external-beam radiotherapy (EBRT) and high-dose-rate brachytherapy (HDR-BT) as a preoperative strategy (17-19). In particular, the optimum radiotherapy dose, as well as the role of surgery, still has to be determined (20-23).
Herein we report results of 24 patients presenting with bulky early-stage cervical carcinoma and with negative pelvic or para-aortic lymph nodes on pre-treatment imaging who were prospectively followed. All were treated with preoperative and concurrent EBRT–chemotherapy and HDR-BT.
Materials and Methods
Patients' characteristics. Between 2002 and 2008, 24 patients with operable cervical carcinoma were referred to the Department of Oncology and Nuclear Medicine for radiation therapy and chemotherapy. Staging procedure included gynecological examination, biopsies, computer tomography of the abdomen, magnetic resonance of the pelvis, chest radiography and cystoscopy. Treatment prescriptions. Radiotherapy: EBRT was administered using photons via a four-field ‘box’ technique (two lateral fields plus one anteroposterior and one posteroanterior field). Patients were treated prone. The anterior–posterior treatment fields extended from the L4/L5 interspace to the foramina obturatoria, encompassing the lowest level of disease. Lateral fields were individually placed according to computer tomography imaging. Radiation volume always included the uterus, paracervical and parametrial tissues, the uterosacral region, and external iliac and hypogastric lymph node regions. The radiation dose was prescribed at the isocenter of all beams. The intended pelvic dose was 40 Gy in 22 fractions over 30 calendar days.
BT was intended to commence after the second week of pelvic irradiation at which point anatomical and geometrical conditions for brachytherapy had been evaluated. Intracavitary HDR-BT treatment was delivered using Ir-192 via tandem-and-ring after-loading applicators. The prescribed dose to point A (a reference location 2 cm laterally and 2 cm superiorly to the cervical os) was to be administered in four weekly insertions, at 7 Gy each.
Chemotherapy: Concurrent chemotherapy was to be administered weekly, consisting of an intravenous infusion of cisplatin (30 mg/m2 of body) in four to six cycles.
Surgery: Subsequent to EBRT, chemotherapy and HDR-BT, all patients were to undergo radical hysterectomy and bilateral salphingo-oophorectomy without lymph node dissection.
Pathological examination. Pathological response was evaluated in surgical specimens according to the presence of residual tumor at the cervix or in paracervical tissues. Categories were pathological complete response, or microscopic or macroscopic-residual disease.
Follow up and statistical analysis. During treatment, patients were evaluated weekly by clinical assessment, pelvic examination, and complete blood count with differential and platelet counts. Renal function tests were obtained prior to each cycle of chemotherapy. Upon completion of all treatments, asymptomatic patients were followed at three-monthly intervals for six months, then six-monthly intervals for two years, and annually thereafter. All patients were evaluated by a gynecologist and a radiation oncologist. Statistical analyses included descriptive distributions, with overall survival estimated and plotted by the method of Kaplan–Meier.
Analysis of complications. Complications were recorded for the genitourinary gastrointestinal tracts. All acute and late complications were scored according to the Radiation Therapy Oncology Group (RTOG) scale (34).
Results
In this prospective clinical study, we evaluated the relative safety and effectiveness of a multimodality strategy with attention to high cumulative preoperative radiation dose with a scheduled surgery. In total, 24 patients were enrolled into the study; their characteristics are shown in Table I. All 24 patients had negative pelvic and para-aortic lymph nodes on imaging and a World Health Organization performance status of 1 or less; none had a prior history of malignancy.
All patients commenced first-line treatment between September 2002 and January 2009. Actual delivered doses for EBRT and HDR-BT are shown in Table II. Regardless of the final delivered dose, all EBRT fractions were administered at 1.8 Gy per day. Field arrangements were 4-field in 20 cases, but were 2-field in four cases (due to treatment planning requirements). The median dose of EBRT was 40 Gy, sixteen cases received 40 Gy in 22 fractions, four cases received between 42 and 46 Gy, in 23-25 fractions, and two received 50.4 Gy in 28 fractions. Two cases received doses under 40 Gy: 28.8 in 16 fractions because of severe diarrhea; and 37.8 Gy in 21 fractions because of patient indolence. All cases received weekly cis-platinum of 30 mg/m2 of body surface during the course of EBRT, but two patients had only four cycles of chemotherapy due to myelosupression.
HDR commenced in the third week of EBRT. HDR fractions were given seven days apart with no EBRT on the same day. The median delivered dose was 28 Gy to point A with BT HDR. The median biologically -effective dose (BED) to point A was therefore 47.6 Gy (range=23.8-63.8 Gy). The median dose at the rectal reference point was 15.43 Gy (mean=15.1 Gy, range=5.57-21.12 Gy), with a median BED of 36.5 Gy (range=16.2-63.8); and the median dose at the bladder reference point was 17.38 Gy (mean=16.0 Gy, range=5.09-23.43 Gy), with a median BED of 42.3 (range=15.2-71.1 Gy). Two patients received only two HDR applications each due to myelosuppresion, with admissions to another Hospital at the time they were to receive HDR-BT. One patient received seven HDR fractions due to gynecological estimation for tumor response. However, all three of the patients with variations in HDR-BT received 40 Gy in 22 fractions for their EBRT-phase of treatment.
Overall treatment time from commencing EBRT to completing HDR applications was a mean of 42 days (median=40, range=29-60 days). Following the last HDR application, surgery was undertaken between 20 and 64 days later, with a median duration of 42 days. Pathology demonstrated no cancer present in 12 out of 24 cases at the time of surgery (50% complete response, 95% confidence interval 29-71%). One of these 12 cases exhibited only atypical epithelial cells at the tumor site, and six showed chronic erosions on the cervix and post-radiation changes, but no residual cancer. The one case with adenosquamous disease, along with two out of the four with adenocarcinoma, were all tumor-free at surgery (i.e. 3/5 had a complete response) as compared with cases of squamous cancer (9/19), with a non-significant two-tailed p-value of 0.9).
No patient was lost to follow-up (up to September 2012, for this analysis). Overall, six patients had died (Table III). Three deaths were from distant metastatic disease (13%; 95% confidence interval=3-32%) and these three cases were without evidence of local failure. One patient died from a comorbidity (pneumonia) unrelated to cancer and cancer treatments. Another died due to a renal comorbidity but this was unrelated to cis-platinum (postoperative sepsis after T1 renal tumor removal). A sixth patient died with renal failure and renal toxicity likely secondary to cis-platinum treatments, which thus may be considered a treatment-related fatality (1/24 or 4%, 95% confidence interval=0.1-21%). Notably, during follow-up to death, none of the six cases experienced local failure in the surgical bed, despite 50% tumor complete response.
Patients' characteristics (N=24).
Treatment characteristics.
Overall, treatments were well-tolerated. No immediate or acute treatment-related deaths were observed (Table IV). Chemotherapy toxicity and acute radiation complications were acceptable, with no severe grade 3-4 acute toxicities (Table V).
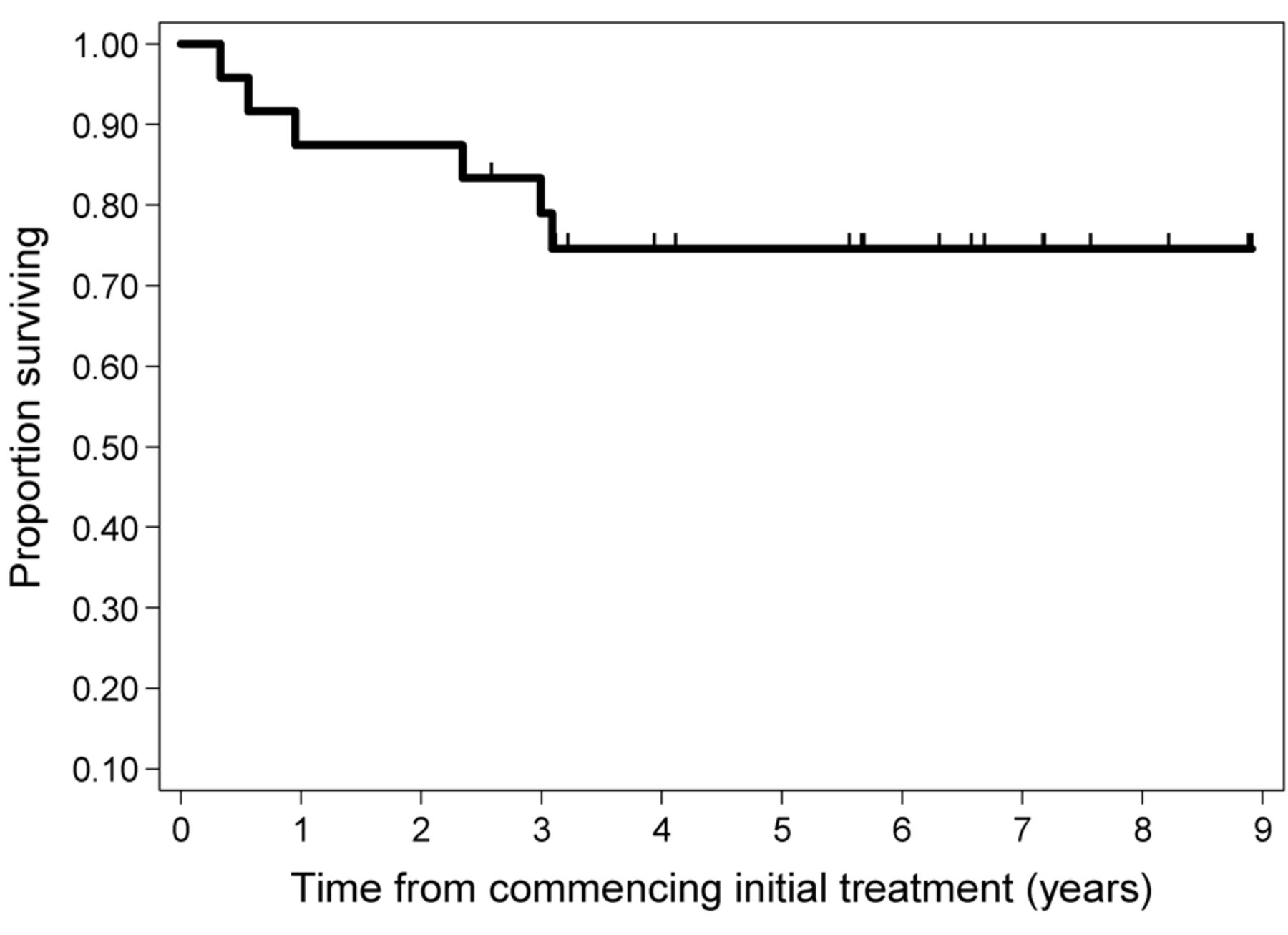
Crude observation time ranged from 0.32 to 8.90 years, with a mean of 4.87 and a median of 5.59 years. By the method of Kaplan–Meier, overall survival at five years estimate at 75%, sustained thereafter through 8.9 years (Figure 1; 95% confidence interval=52-88%). Overall, 13 of the patients had between 5.5 and 8.9 years of follow-up without recurrent disease, while all six deaths occurred between 0.33 and 3.1 years from commencing initial treatment.
Death cases analysis (N=6).
Overal survival.
Incidence of toxicity according to the Radiation Therapy Oncology Group RTOG criteria
Discussion
The clinical management of women with stage IB-IIB cervical cancer with completion surgery following chemoradiotherapy remains a controversial and debatable matter.
In many Centers, surgery is considered for patients with residual disease. Residual disease is a strong predictor of disease progression and death (24-27). However, the impact of surgery on survival remains to be proven in randomized trials. Meanwhile, chemoradiotherapy might not yet be fully-optimized for local control of disease. Greater local control by improving the delivery of radiation therapy, especially in BT, might pre-empt the debate about surgery, which would then not be required. BT is a crucial part of treatment to achieve local control. The new modalities of this treatment with 3-D magnetic resonance imaging-guided procedures are becoming the new standard for reducing the rate of local failure in patients, without surgery (28-30). However, the reliability of emergent methods to control local disease without subsequent surgery has yet to be reported. Therefore, and for most Institutions for the foreseeable future, radiotherapy-alone (EBRT plus HDR-BT), chemoradiotherapy (i.e. chemo-EBRT plus HDR-BT), or tri-modality therapy (the foregoing plus surgery for any residual disease) are standards of care.

{kind=link}
Kaplan–Meier overall survival plot for all 24 patients: 5-year estimate at 75%, sustained thereafter through to 8.9 years; 95% confidence interval=52-88%.
Tri-modality approach for all patients with stage IB-IIB might improve local control and even survival but could expose patients to greater adverse events, including surgical complications. There are few published reports of results of surgery after chemoradiotherapy (9, 18, 26, 31, 32). In these studies, the rate of residual disease was associated with the initial stage of disease, and the use of preoperative brachytherapy. Morbidity varied between 15% and 47%. This was associated with how radical or aggressive the surgical procedure was, along with the size and extent of any residual disease. The rate of pathological complete response was found to be between 52% and 76%. Survival was associated with the presence and size of residual disease, and nodal involvement (33). All of these associations are expected. However, in these studies, different disease stages were investigated (IB2-IVA), and doses of external radiation varied somewhat (39 to 45 Gy), along with heterogeneity in modalities of chemotherapy (cisplatin-alone, or in combined regimes) and in brachytherapy (e.g. different dose rates), number of BT sessions, and dose per fraction (1×15 Gy low-rate and 2×6 Gy HDR). Heterogeneity increases the generalizability of the main findings that pathological complete response is not guaranteed with modest regimens of chemoradiotherapy, and that surgical eradication may benefit some patients, including those at greater risk of, or who have evident persistent disease. Further research into tri-modality therapy and intensification of chemoradiotherapy seems justified.
This study demonstrates that tri-modality therapy is relative safe (only one death as a possible complication from chemotherapy) and there were few acute and chronic adverse events. Patients had stage I and II disease and 50% demonstrated complete pathological response with no evidence of tumor, as documented with surgical excision following concurrent cisplatin therapy with EBRT, and HDR–BT, but no case failed centrally in the surgical bed. Overall survival at five years was 75%, sustained thereafter through to 8.9 years. There were no disease-related deaths: three deaths were secondary to distant failure and three additional deaths were without evidence of active malignancy, despite 50% tumor complete response.
This experience indicates that tri-modality therapy is feasible. The modal regimen was 40 Gy of EBRT combined with weekly cisplatin (30 mg/m2) and with four sessions of HDR–BT prescribing 7 Gy to point A, followed by surgery six weeks after the last session of HDR-BT. The four sessions of HDR-BT represent a relative dose escalation to improve locoregional eradication of disease, to improve surgical margins, and it did not result in any significant perioperative toxicities.
Limitations of our study include a small sample size, such that confidence intervals on all point estimates of effects are relatively wide. Furthermore, several patients were not able to receive the complete EBRT, chemotherapy and HDR–BT treatments. Our study does, however, demonstrate the feasibility of consistently administering all aspects of the treatment plan as intended. Patients had a range of pathologies and stages, making this a relatively heterogeneous group of cases. While this was a prospective clinical study of consecutive cases, it was not a randomized trial. Comparison with other studies can generate hypotheses for further testing towards the goal of improving survival of women with cervical cancer.
Modern therapy for cervical cancer of all stages has evolved considerably over the past several decades due to results from randomized trials, combining chemotherapy with EBRT as a radio-sensitizer, converting from low-dose-rate to HDR–BT, and escalating the HDR–BT regimen. The role of chemosensitization remains controversial. Several other randomized trials have compared BT regimens. Due to on-going controversies about chemosensitization and the radiobiology of differing BT regimens, a randomized trial of the International Atomic Energy Agency was initiated in 2005 for patients with stages IIB and IIIB cervical cancer, and who are HIV-negative. This 4-arm trial (accrual completed in 2010, at 601 patients) compares 2×9 Gy HDR-BT against 4×7 Gy HDR-BT, and compares cisplatin to no cisplatin. No case proceeds to surgery following completion of all protocol therapy. Early results from this trial are expected in 2013. Should there be appreciable local failures, it might indicate the potential for planned surgery to improve results further. Conversely, this trial might demonstrate that 2×9 Gy is more effective than 4×7 Gy, which would be resource sparing. However, whether two large doses of HDR-BT would be associated with greater surgical complications would be unknown, as routine surgery is not being conducted in this trial.
Cases with lesser stages than IIB and IIIB, as included in our study (11 out of the 24 cases) are likely to experience a smaller risk of locoregional failure and a correspondingly better 5-year overall survival than those in the IAEA Registered Trial NCT00122772, listed at http://clinicaltrials.gov/ct2/show/NCT00122772. trial, for example. Our rate of local failure was 0%, with possibly one treatment-related death (chemotherapy renal event). Surgical findings demonstrated 50% complete response about six weeks after the completion of initial chemoradiation and BT. A further delay to surgery might have produced better pathology findings, but delaying surgery might result in surgical complications.
In summary, our experience indicates the relative safety and efficacy of modern tri-modality therapy in the management of stage IB and II cervical cancer, with planned surgery approximately six weeks after completing neoadjuvant chemoradiation and BT. As evidence accumulates of success with optimized modern tri-modality strategies, a randomized trial to compare the sequential tri-modality strategy against chemoradiation and BT without planned surgery becomes appropriate.
Footnotes
-
Competing Interests
All Authors have completed the Unified Competing Interest form downloaded from www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
- Received February 20, 2014.
- Revision received May 5, 2014.
- Accepted May 7, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved