

Abstract
Background: Intraosseous lipoma remains a poorly-characterized tumor. In paticular, the natural course of intracalcaneus lipoma after conservative treatment and the appropriate surgical modalities are still quite controversial. Patients and Methods: We reviewed six symptomatic patients who underwent curettage of intracalcaneus lipoma followed by grafting of α- or β-tricalcium phosphate. An endoscopically-assisted technique was used in one case. Results: All patients experienced heel pain that increased acutely after minor trauma. Heel pain disappeared soon after surgery in five cases. One patient experienced short-term mild chronic regional pain syndrome for short term. β-tricalcium phosphate was completely resorbed and remodeled after transplantation. Conclusion: Surgical treatment is indicated for cases that are: i) symptomatic, ii) larger than the critical size, and iii) prone to pathological fracture. Curettage of intracalcaneus lipoma involving an endoscopically-assisted technique and filling of the defect with β-tricalcium phosphate is a feasible method and is minimally-invasive for the patient.
- Intraosseous lipoma
- calcaneus
- β-tricalcium phosphate
- endoscopy
Intraosseous lipoma was first reported in 1910 by Wehrsig, who described this tumor in the proximal fibula of a 5-year-old girl (1). To our knowledge, approximately 20 reports of intraosseous lipoma of the extremity have so far been published in the English literature (2-6). Amongst these, Child, in 1955, was the first to describe a case of intracalcaneus lipoma (ICL) (7), ICL comprises fewer than 15% of all intraosseous lipomas.
Intraosseous lipoma remains a poorly-chacterized tumor for orthopedic surgeons and the etiology of ICL in particular is completely unknown. The natural course of ICL after conservative treatment and the appropriate surgical modalities are still quite controversial. In the present study, we reviewed six symptomatic patients who underwent curettage of ICL followed by grafting of bone substitute into the defect. Our purpose was to elucidate the clinical features of ICL and to discuss the appropriate surgical modalities for this rare lesion.
Patients and methods
We reviewed six patients with symptomatic ICL who visited the Yamaguchi University Hospital beginning in 2007. The mean age of patients was 43.8 (range=22-74) years and there were five females and one male. All patients were treated surgically. The preoperative diagnosis was made by plain radiography (Figure 1) and magnetic resonance imaging (MRI) (Figure 2) and was confirmed postoperatively by the histological findings. At surgery, curettage of ICL was performed and the defect was filled using artificial bone substitute. α-tricalcium phosphate, Biopex® (HOYA Technosurgical Corporation, Tokyo, Japan) was used for three cases, while β-tricalcium phosphate (β-TCP), Superpore® (HOYA Technosurgical Corporation) was used in the others. An endoscopically-assisted technique proposed by Futani et al. was used in case 6 (Figures 3, 4). Full weight-bearing was permitted the day after surgery (8). We assessed the onset of symptoms, tumor location, tumor size, image findings, Milgram's classification (9, 10), preoperative differential diagnosis, pain relief after surgery and complications. Milgram classified intraosseous lipoma into three stages as follows (9, 10). Stage I lesions are purely radiolucent and contain viable lipocytes and bony trabeculae without any necrosis (Figure 5). Stage II lesions are partially radiolucent, with some calcification, and display a mixture of necrotic and viable lipocytes. Stage III lesions are larger calcifications and the fat component is fully necrotic. The mean follow-up period for this cohort was 40 (range=6-72) months. We received informed consent from patients to carry out this study.
Results
The detailed patient information is summarized in Table I. All patients had experienced heel pain for several months to years that had increased acutely after minor trauma, such as rope jumping, falling or long periods of standing at work. Two cases were treated as plantar fasciitis. In all patients, the location of the ICL was in the so-called Ward's triangle and the mean size was 19 mm (range=16-20 mm). Calcification in the ICL was recognized by radiography in only two cases (33%). MRI on T1-weighted images showed lower signal intensity than surrounding normal adipose tissue. All ICL's showed high signal intensity on T2-weighted images. According to Milgram's classification (9, 10), two ICLs were stage I, two were stage II and two were stage III. Heel pain disappeared soon after surgery in five cases. Case 4 showed mild chronic regional pain syndrome but healed within three months. There were no other complications. Plain radiographs showed residual Biopex® in the calcaneus for up to five years in three cases, whereas Superpore® was completely resorbed and re-modeled within six months after transplantation.
Data of six patients with intracalcaneus lipoma.
Discussion
Incidence and etiology. Although the incidence of intraosseous lipoma is thought to be less than 0.1% of all primary bone tumors, its true incidence may be much higher. This is because many patients are unlikely ever to consult an orthopedic clinic due to the absence of symptoms. In a study by Goto et al., only two out of 13 affected cases were symptomatic (11). This type of lesion is usually found incidentally on radiographs taken for an unrelated disorder. We experienced one such case of intraosseous lipoma in the humeral head where the lesion was found incidentally following a minor trauma.
Intraosseous lipoma frequently causes pain in the foot. Apart from the calcaneus, Atay et al. reported a case of intraosseous lipoma of the talus in a 38-year-old male (12). In the present study, the six cases with ICL were symptomatic. Interestingly, all patients noticed increased pain after minor trauma. Intraosseous lipoma may cause symptoms when present in weight-bearing bones. Middle-aged and older female patients showed weakened mechanical strength of the calcaneus due to aging and ICL. Following minor trauma, small pathological fractures may occur in the affected calcaneus.
The etiology of ICL is unknown. Some hypotheses have been proposed, including post-traumatic secondary bone reaction, healing bone infarction and benign neoplasm (13-15). Kapukaya et al. classified intraosseous lipomas as intramedullary, intracortical, sub-periosteal and parosteal types according to their location (16). All ICLs are classified as the intramedullary type. It was interesting that all cases of ICL were localized within the neutral, or so-called Ward's triangle (17). This area is devoid of the trabecular network that crosses the calcaneus and is thus sometimes referred to as pseudo-tumor in standard radiography. More recently, the theory of a true benign tumor is gaining support as the most likely origin (13). However, if ICL is a true neoplasm, we cannot explain why ICL always arises at the intramedullar Ward's triangle in patients of different ages. Trauma can be a trigger for pain, but it cannot cause the tumor. The vascular theory is not supported because ICL also occurs in young patients. Further investigations are required to fully-elucidate the etiology of ICL.

Case 6. A lateral view of the calcaneus showed a well-defined osteolytic lesion at the neutral, or so called Ward's triangle.
Diagnosis. ICL cannot be diagnosed using only plain radiographs. If the radiograph shows a cystic lesion, this can be misdiagnosed as a solitary bone cyst or other cystic tumor. Because the radiographic appearance of ICL is not unique, it is impossible to distinguish the two lesions. A central calcified or ossified nidus is often seen. In our series, 3 cases showed calcification in the ICL but this was not diagnostic.
MRI is a very useful tool to distinguish solitary bone cysts from ICL (18). This is because MRI shows high signal intensity on both T1-weighted and T2-weighted images. ICL shows low signal intensity on MRI of short T1 inversion recovery. However, the tumor signal can be different if the lesion is involuted. Milgram stage III lesions exhibited a low signal in T1-weighted images but high signal in T2-weighted images because of cystic or myxomatous changes (Figure 2).
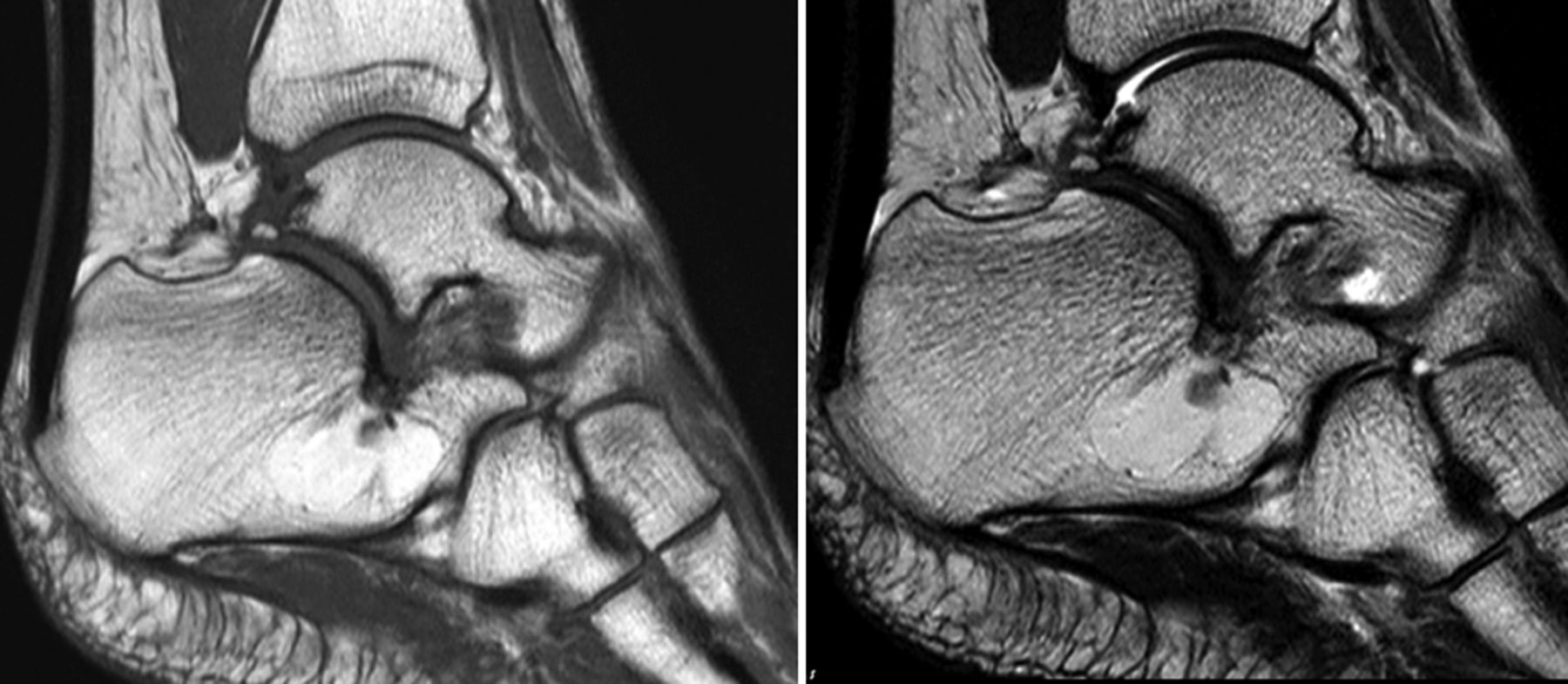
T1-(right) and T2-(left) weighted magnetic resonance imaging of a high-signal heterogenous tumor, suggesting cystic change of the intraosseous lipoma.

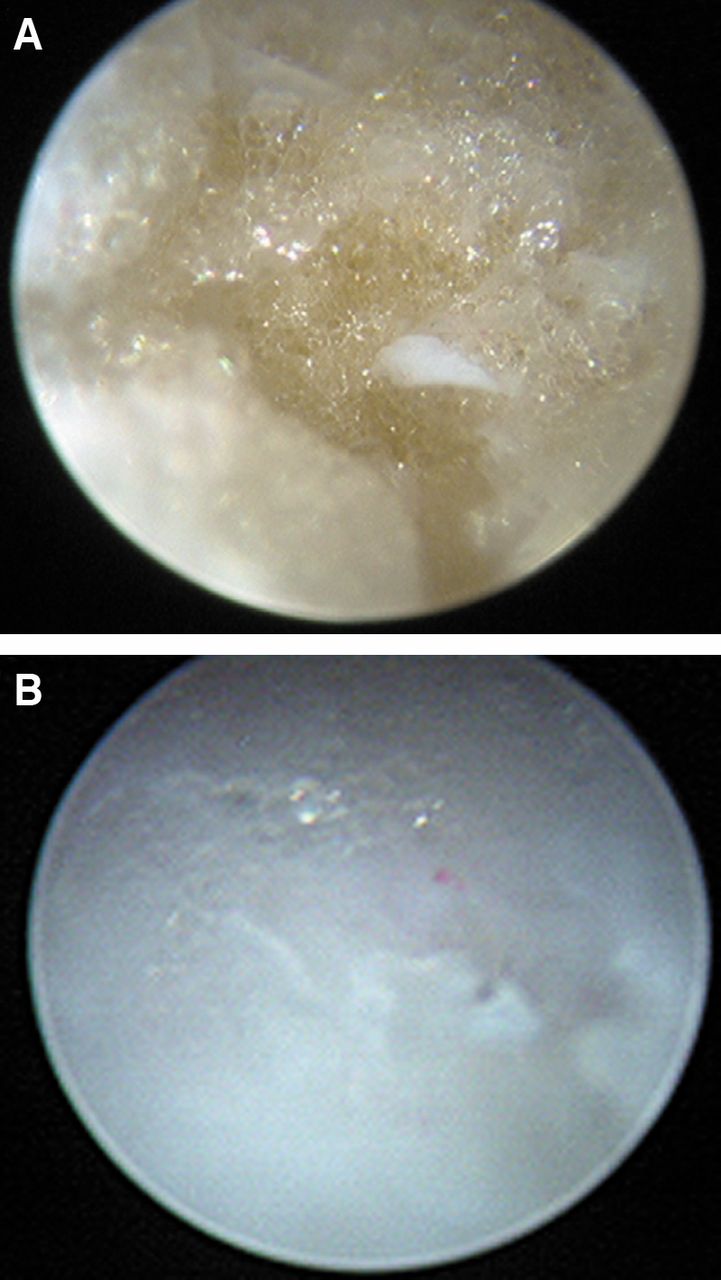
A 2.7 mm diameter, 30 degree Hopkins telescope (Karl Storz, Germany) was inserted through the lateral portal of the calcaneus. Endoscopic image of intracalcaneus tumor. A: Before resection, a yellowish intracalcaneus lipoma was seen on the surface of the bone. B: The intact bony surface was seen after curettage of the tumor.
Karthik and Aarthi reported a case of ICL that was misdiagnosed as plantar fasciitis (19). Similarly, two of the present cases were diagnosed as plantar fasciitis. Pre-operative biopsy is not necessary if the surgeon is aware of the possibility of ICL.

Postoperative X-ray showed beta-tricalcium phosphate filling the bony defect.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
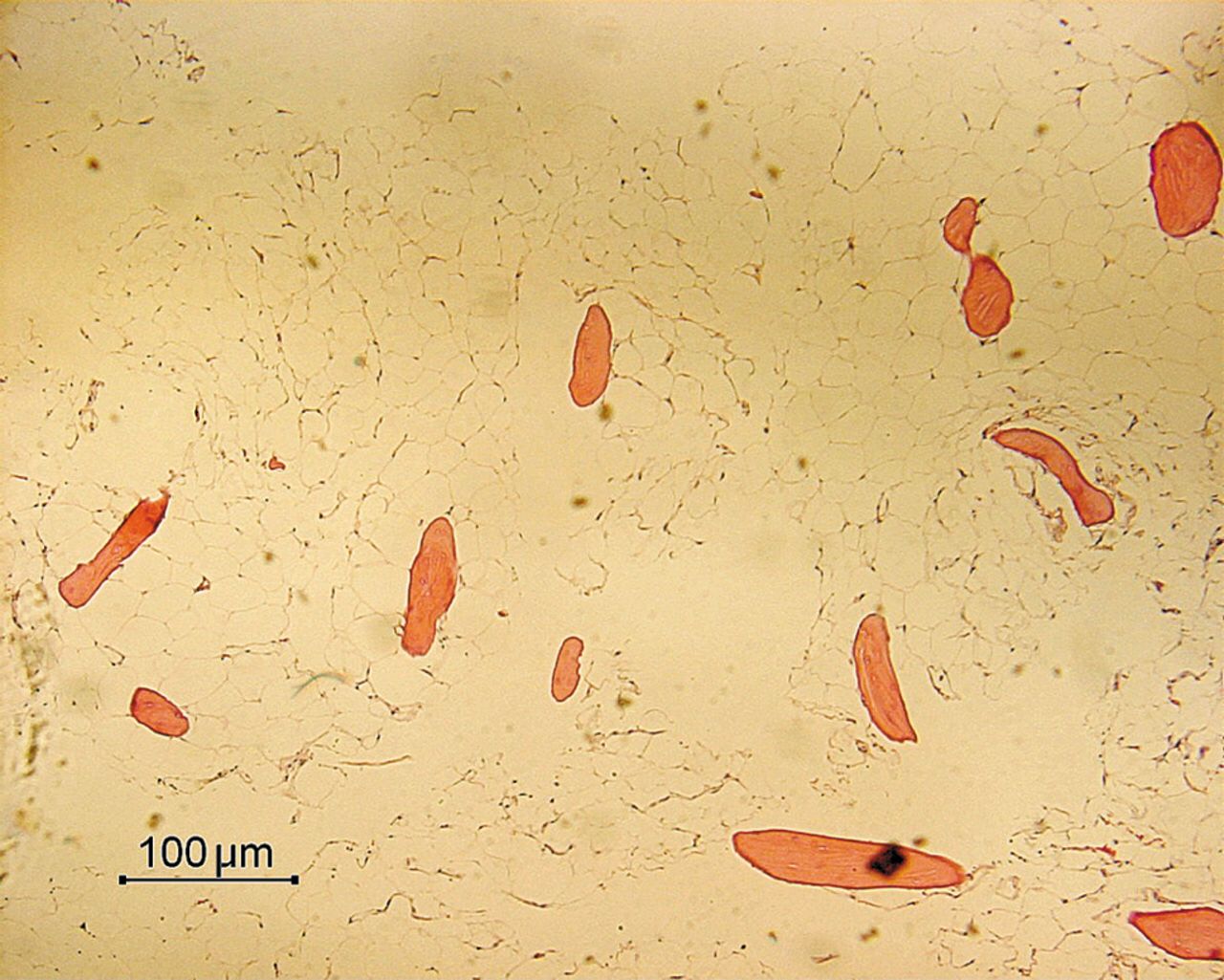
Histopathological diagnosis was the intraosseous lipoma, compromised of viable fatty tissue and small bone trabeculae.
Treatment. The natural course after conservative treatment is still unknown. Pathological fracture of the calcaneus has been reported in association with intraosseous lipoma. Weinfeld et al. reviewed four cases with ICL, one of which involved a pathological fracture of the calcaneus (20).
The most appropriate treatment for ICL is still controversial and is likely to depend on site, size and symptoms. A critical size for ICL has been defined as a lesion that extends the full breadth of the calcaneus laterally to medially in the coronal plane, while occupying at least 30% of the anteroposterior length of the calcaneus (21).
Because ICL is a benign lesion, surgical treatment is not always necessary (22). Hirata et al. reviewed 11 patients, of which seven were surgically-treated and four were conservatively treated (23). They concluded that surgical intervention was not always necessary, but that it did relieve symptoms in some patients. Asymptomatic ICL should not be treated surgically because the aim of surgery is to relieve pain and to prevent a pathological fracture, especially when the lesion is located in Ward's triangle. Our indications for surgical intervention are: i) symptomatic, ii) larger than the critical size, and iii) possible occurrence of a pathological fracture.
Treatment options include curettage with or without bone grafting, or with a bone graft substitute. There have, as far as we aware, so far been no reports of local recurrence of ICL after simple curettage. Goldner et al. made a bony fenestration of 2×2 cm for curettage of ICL and allowed weight bearing at 12 weeks after surgery (24). To reduce the non-weight bearing period, the endoscopically-assisted method is useful for resection of ICL. Futani et al. first introduced this procedure and reported that it avoided the risk of postoperative pathological fracture (8). They made a small fenestration of 5×5 mm so as not to reduce the strength of the calcaneus. We made one portal on the lateral side of the calcaneus and this was sufficient to see the lesion and to complete curettage of the ICL.
Filling material for calcaneus bone defect. We used two different types of bone substitute for filling the defect resulting from curettage of ICL. Biopex® is an injectable, bioactive bone cement consisting of α-tricalcium phosphate (25). Because of its closed porous architecture, absorbance and replacement occurs only at the surface. The compressive strength of Biopex is 70 MPa. We initially used Biopex® as the filling material because of its high compressive strength, but in three cases residual material was seen in the calcaneus on plain radiography up to five years later. SuperPore® is a newly-developed superporous β-tricalcium phosphate. Seto et al. reported rapid resorption and new bone remodeling following the implant of β-tricalcium phosphate into benign bone tumors (26). SuperPore® has uniform triple pore structures, comprising of macropores, micropores and interconnecting pores. The compression strength of SuprePore® with 75% porosity was 5 MPa to 7 MPa. Importantly, Superpore® was completely resorbed and re-modeled within six months after transplant. We therefore recommend Superpore® as the filling material to be used for bone defects of the calcaneus.
- Received December 7, 2013.
- Revision received December 21, 2013.
- Accepted December 24, 2013.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved