

Abstract
Background/Aim: The aim of the present study was to define prognostic factors and to evaluate liver resection as an additive tool in metastatic melanoma. Patients and Methods: In a case-control study, 32 patients with hepatic melanoma metastasis were analyzed between 1998-2012. Sixteen patients who underwent liver resection (6 patients with multimodal therapy) were matched to 16 patients scheduled for non–surgical approaches. Univariate and multivariate analyses were performed. Results: Following primary resection and liver resection, respectively, survival was better for patients who underwent surgery in addition to multimodal therapy with 219 and 28 months, when compared to patients scheduled for non-surgical approaches with 64 (p=0.04) and 8 months (p=0.6). Following primary resection, primary tumor site, metastatic time <70 months, combination of multimodal therapy and surgery were of prognostic value (p<0.05). Conclusion: Liver resection should be considered a suitable additive tool in multimodal therapy of resectable metastatic melanoma.
- Melanoma
- hepatic metastasis
- liver resection
- multimodal therapy
- survival
- case-control study
Incidence and mortality of melanoma have both dramatically increased in the past decades (1, 2). Widespread metastatic melanoma occurs in approximately 30-50% of all melanoma patients with distinct differences being noted for histological subtypes (3-5). Cutaneous melanoma primarily metastasizes to regional lymph nodes and soft tissues, with liver lesions found in only 14-20% of all cases (6, 7). In contrast, liver metastases are found in 95% of patients with ocular melanoma and in nearly 40% as first and only site of metastasis (8-10).
Multimodal therapy concepts in hepatic metastatic melanoma have recently changed with immunotherapy and targeted drugs being more effective than chemotherapy (11-13). Despite an improved mechanistic understanding of tumor biology and fundamental advances in therapeutical approaches, occurrence of liver metastases from both ocular and cutaneous melanoma is still associated with an extremely poor prognosis. Overall survival has been reported to be 6-8 months with 1–year survival rates of approximately 10-15% in patients with metastatic melanoma to the liver (5, 6, 14).
In parallel with multimodal drug therapies, surgical techniques and recent innovations in perioperative management have dramatically improved over time. As a result, decreased postoperative morbidity and mortality of patients undergoing major liver resections have been noted. A part from technical aspects having made liver resections safely applicable to old and even multi-morbid patients, an emerging number of studies suggest liver resections as an oncologically reasonable tool even in non–colorectal and non–neuroendocrine cancers (15-17).
There are only few retrospective studies available on surgical approaches for melanoma stage IV, mostly reporting single-centre experiences (6, 8, 9, 18-22). Comparative studies investigating potential benefits of liver resection integrated in multimodal therapy concepts for melanoma liver metastasis are currently lacking. The present study represents the first case–matched control study investigating the role of surgery in hepatic metastatic melanoma in comparison to non-surgical approaches. Our study indicates that liver resection should be considered a suitable additive tool in multimodal therapy of resectable metastatic melanoma.
Patients and Methods
Patient selection and study population. Patients with melanoma stage IV who were treated at the University Hospital of Leipzig between 1998 and 2012 were retrospectively identified from our clinical tumor registry. The study was approved by the local ethical commission board from the University of Leipzig.
Among these patients, 16 underwent liver resection with or without systemic therapy for metastatic melanoma (surgical therapy (ST)). In this case–matched control study, these patients were individually matched (1:1) with 16 patients who were treated non-surgically (non–surgical therapy (NST)).
Each case patient of the surgical group was matched to each control patient on the following criteria: - Patient age at diagnosis of melanoma and development of liver metastasis, - Year of tumor diagnosis, - Stage of primary tumor and primary tumor type, - Time interval between the primary tumor and occurrence of liver metastases.
All patients underwent staging examinations to determine suitability and eligibility for surgery including physical examination, serum laboratory tests, abdominal ultrasound, computed tomography (CT) (chest and abdomen) or magnetic resonance imaging (MRI). Fluorodesoxyglucose positron emission tomography (FDG–PET/CT) scanning was also performed, if available. Diagnosis of liver metastasis was confirmed by fine–needle cytology or biopsy, as indicated. Patient management was stipulated at our two–weekly institutional multidisciplinary case management conference before intervention or surgery.
A surgical intervention by liver resection was limited to patients without relevant co–morbidities and confined metastases to the liver; the possibility to curative resection was based on the imaging examinations. Synchronous extra–hepatic site metastases were no contraindication for study inclusion. A non–surgical procedure was considered for patients with miliary disease, extended and unresectable liver metastases, extrahepatic site metastases or patients' refusal to surgical treatments.
Data collection. The following data were collected for each patient in both groups: age, gender, anatomical primary tumor location (ocular versus cutaneous), primary tumor characteristics (Breslow thickness, Clark level), treatment of the primary tumor (surgical, radiation/systemic therapy, lymph node dissection), time interval between the primary tumor and liver metastases, location, number and size of intrahepatic metastases, details of any adjuvant therapy (chemo–, immuno–/bio–and radiotherapy), tumor recurrence and overall survival.
The following parameters were collected only in the surgical group: resection margins (microscopically complete removal – R0, margins microscopically positive – R1 and grossly visible tumor – R2), surgical procedure of metastatic lesions (major resection (≥4 segments) versus minor resection (<4 segments) and perioperative complications according to the Clavien-Dindo-Classification.
Overall survival was calculated as the time from primary melanoma operation to diagnosis of hepatic metastasis. Following occurrence of liver metastasis, overall survival was calculated as the time between treatment (ST – liver resection; NST – Systemic treatment) until last follow-up or death.
Statistical analysis. Data are presented as median (range) unless otherwise specified. The Student's t-test, χ2 and Wilcoxon–Mann–Whitney test were used where appropriate. To explore prognostic factors for the survival of patients, a univariate Kaplan-Meier analysis was performed and the log-rank test with two–sided test was applied to test statistical significance between survival curves for each potential risk factor. A stepwise multivariable Cox regression model was applied. All data were analyzed by using the SPSS software (SPSS Inc., Chicago, Illinois, USA, version 18.0).
Results
General and oncological characteristics. We here investigated the outcome of 32 patients (females=12, males=20) with a median age of 59 years (range=28-76) suffering from hepatic melanoma metastasis. Twelve and 20 patients had been diagnosed with ocular melanoma and cutaneous melanoma, respectively. Median Breslow thickness was 3±0.5 mm and the Clark-Level was III in 6 patients, IV in 17 patients and V in 9 patients. Primary tumor had been treated surgically in all cases of primary cutaneous melanoma with wide local excisions being performed with (n=15) or without (n=5) extended lymph node dissection. Treatment of primary ocular melanoma was enucleation in 9 patients and external beam irradiation in 3 patients.
Median time interval between the primary tumor and the occurrence of liver metastases was 82 months (range=1-236 months) with a median number of 3.4±0.8 metastatic lesions being localized unilobular in the liver. The most common site of synchronous extrahepatic disease was the subcutaneous soft tissue (n=7 patients), the lung (n=5 patients), the brain (n=3 patients), gastrointestinal tract (n=1 patient) and the spine (n=1 patient). Sixteen patients were treated surgically (liver resection), out of which 6 patients were additionally enrolled in multimodal therapy regimes. Herein, 4 patients were treated with a combination of dacarbazine/interleukin−2/ interferon and/or cisplatin, in 2 patients bioimmunotherapy was undertaken after surgery. Systemic therapy without operation was applied in 16 cases with immunotherapy and/or chemotherapy. There were no significant differences regarding general and oncological characteristics between the ST and NST groups (Table I).
Surgical characteristics. Eleven out of 16 patients (69%) in the ST group underwent major liver resection with hemi-hepatectomy and trisectionectomy being performed in 5 (31%) and 6 patients (38%), respectively. Atypical liver resection and segmentectomy were performed in 3 (19%) and 2 patients (13%). Local R0 (margin-free) resection could be achieved in 13 (81%) patients. Median operation time was 265±66 min and intensive care unit (ICU) and hospital stay were 1.5±1 days and 18±3 days, respectively (Table I). Postoperative complications were classified according to the Clavien-Dindo-Classification with an overall postoperative morbidity of 25%. One patient suffered from a grade II complication, two patients from grade IIIa and one patient from a grade V complication. The 30–day mortality in the surgery group was 6.2%.
Clinicopathological and tumor characteristics of the total study population (n=32 patients).
Survival analysis. Median overall survival was 72 months (range=2.9-91.9 months; median follow-up was 9.1 years (range=0.2-27.9 years) following primary resection and 11 months (range=5.2-13.4; median follow-up was 5.4 years (range=0.2-17.1 years) following liver resection, respectively. One-, 3- and 5-year survival following resection of the primary tumor was 93.8%, 84.4% and 53.1%, respectively. Following liver resection, 1-, 3- and 5-year survival was 28.1%, 15.6% and 3.1%, respectively. Following non-surgical therapy in the NST group, 1-, 3- and 5-year survival was 15.6%, 6.2% and 0%, respectively. Median overall survival was 17 months (range=1.6-32.3 months; median follow-up was 61.1 months (range=13.4-123.1 months) following liver resection in the ST group and 8 months (range=1.2-14.4 months; median follow-up was 69.3 months (range=2.3-205.1 months) following non-surgical therapy in the NST group, respectively.
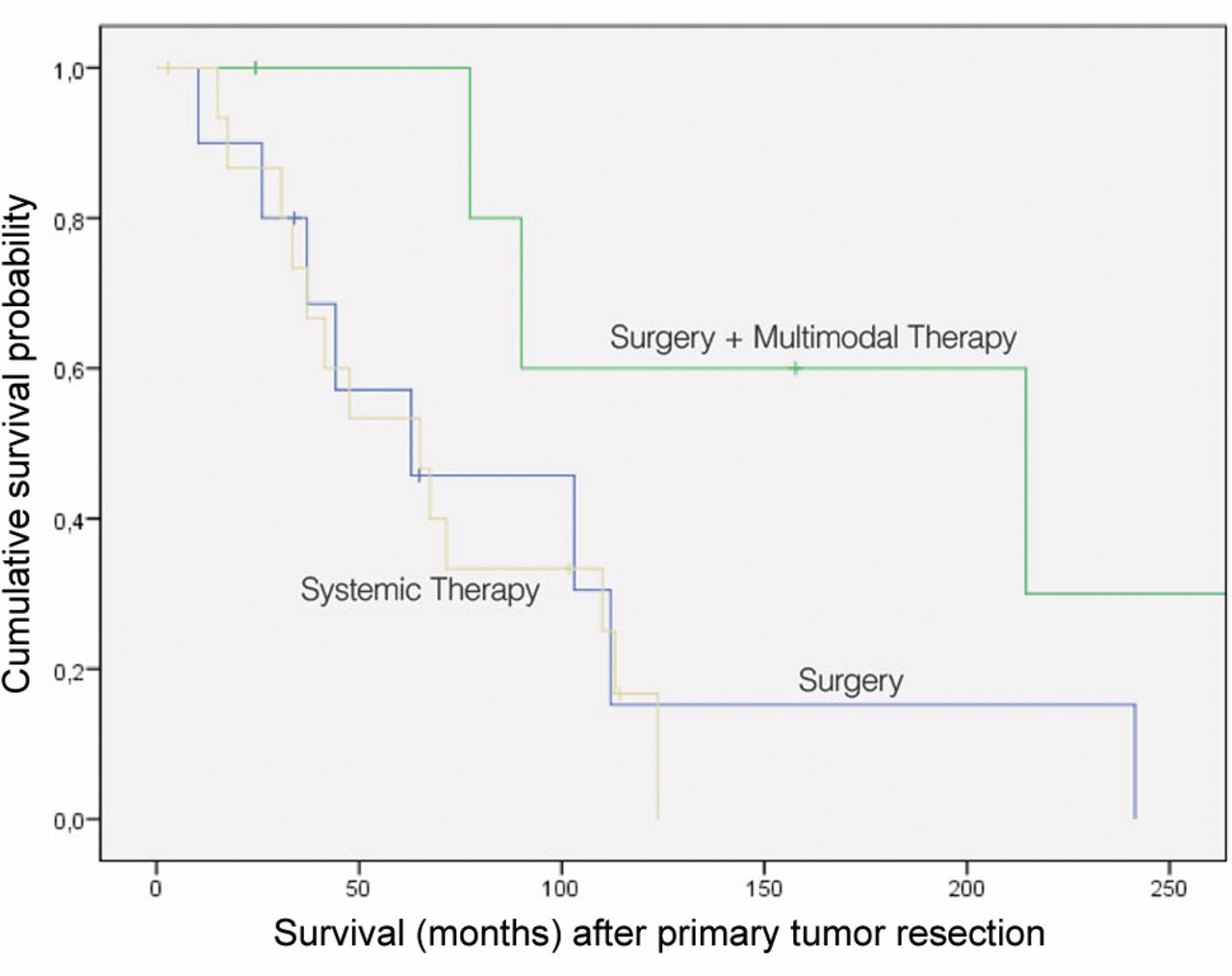
The Kaplan–Meier method showed that localization of primary tumor (p=0.01), interval between resection of the primary and metastasectomy (p=0.023) and surgery in combination with multimodal treatment (p=0.028) were of prognostic impact in our patient cohort following resection of the primary tumor. Survival analysis using a Cox regression model confirmed localization of primary tumor (p=0.015), interval between resection of the primary tumor and metastasectomy (p=0.027) and surgery in combination with multimodal treatment (p=0.044) (Table II) (Figure 1) Following hepatic resection, the Kaplan–Meier method showed trends towards improved survival for patients with <4 metastases, surgery in combination with multimodal treatment and patients receiving >4 courses of systemic therapy (all p=0.05) (Table II) (Figure 2).
In the ST group, prognostic value was confirmed for localization of primary tumor (p=0.029), interval between resection of the primary tumor and metastasectomy (p=0.04) following resection of the primary tumor. Additionally, the Kaplan–Meier method showed that age was of prognostic value (p=0.006). Survival analysis using a Cox regression model confirmed all values that were shown to be of prognostic value in univariate analysis. Following hepatic resection, the Kaplan–Meier method showed that the number of metastases (p=0.04) and resection margins (p=0.02) were of prognostic impact, however, this was not confirmed in multivariate analysis (Table III).
Recurrence. In the ST group, 4 of 16 patients had synchronous extra-hepatic disease at the time of liver surgery, whereas 9 of 16 patients (56%) developed metachronous metastasis after hepatic resection with a median time of recurrence of 12 months (range=1-59 months). Among these patients, the liver was the most common site (n=7), followed by the lung (n=6), gastrointestinal tract (n=4), lung, soft tissue (n=2) and brain (n=1). The remaining 3 patients (ocular, n=2 patients; cutaneous, n=1 patient) did not develop recurrence during the follow-up period. There were no differences regarding the rate of recurrence noted for histological subtypes (ocular vs. cutaneous). Thus, among these 16 patients, negative resection margins (p=0.002) and a history of adjuvant chemotherapy (p=0.02) such as a metastasic time <70 months (p=0.04) were statistically significant for a decreased risk of development of recurrence in univariate analysis.
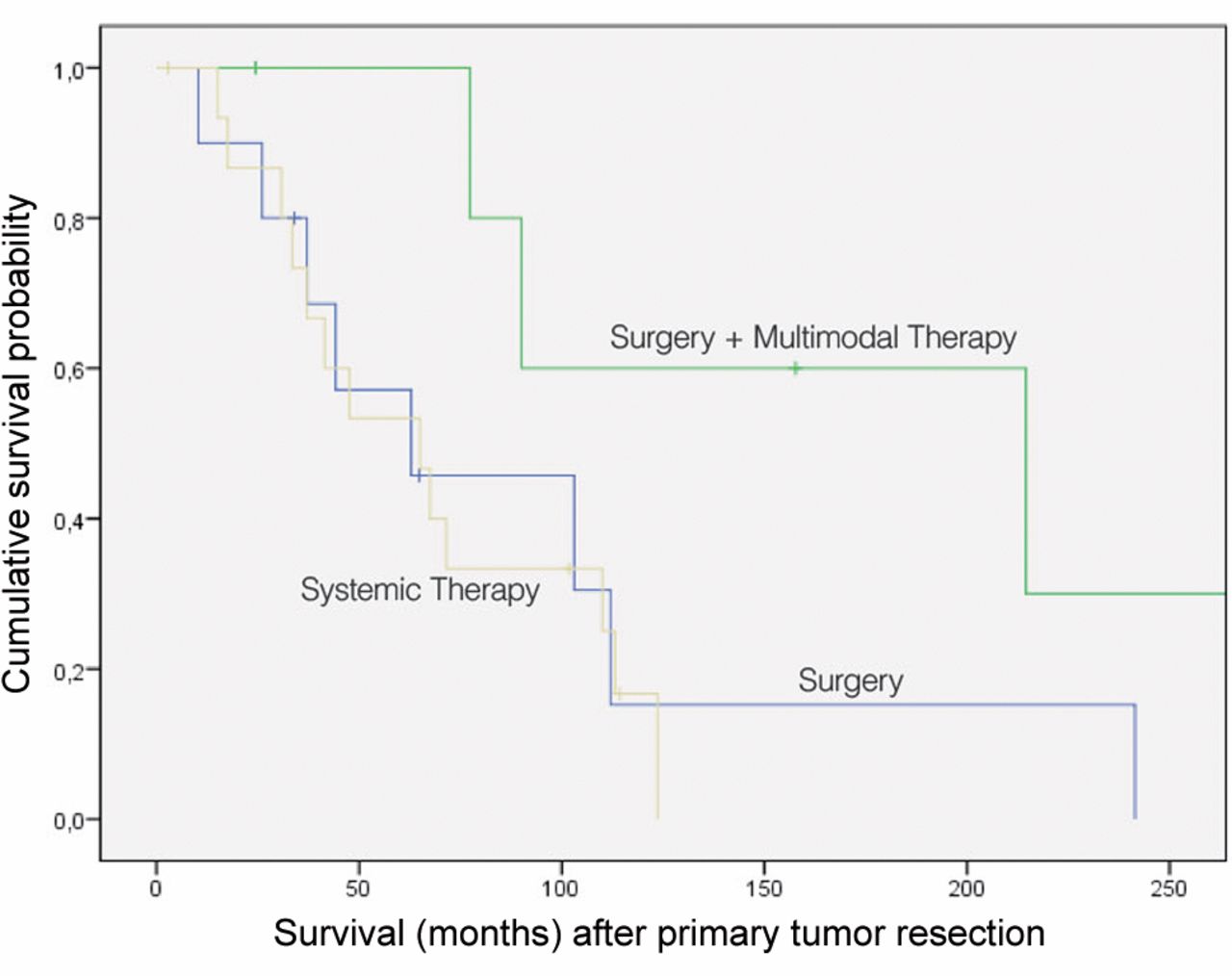
Kaplan–Meier survival curve representing follow-up after primary resection according to Surgery (n=10 patients), surgery and multimodal therapy (n=6 patients; p=0.02) and systemic therapy (n=16 patients).
Discussion
To our knowledge, this is the first case–matched pair analysis in stage IV melanoma with liver metastases comparing surgical and non-surgical treatment strategies. As prospective studies evaluating the role of surgery in multimodal concepts in melanoma stage IV are hard to be established due to the distinct heterogeneity of patients, matching patients' criteria appears to be a suitable way to evaluate the impact of liver resection for metastatic disease. We could demonstrate a reasonable overall survival for these patients with a significant improved survival for patients undergoing liver resection in combination with multimodal therapies, when compared to patients solely receiving systemic therapy.
Systemic therapy represents first-line treatment for melanoma stage IV with a new generation of drugs and promising investigational approaches (1, 13, 23, 24). The number of chemotherapy courses has been noted to be of prognostic value, which underlines the importance of systemic approaches. However, there is emerging evidence that surgical resection may represent a helpful tool in multimodal concepts. In accordance with retrospective case series, our case–control study demonstrates liver resection to be safely applicable for patients with resectable liver metastasis (6, 8, 9, 18-22). Despite a trend towards a higher number of liver metastasis in the ST group, liver resection seems to improve overall survival for selected patients if R0 resection can be achieved. Of note, surgery appears to represent an additive tool in multimodal palliative therapy with no benefits noted for patients who underwent surgery alone.

{kind=link}
{kind=link}
Kaplan–Meier survival curve representing follow-up after liver resection according to surgery (n=10 patients), surgery and multimodal therapy (n=6 patients; p=0.05) and systemic therapy (n=16 patients).
Given a potential role of surgery in multimodal palliative treatment strategies, patient selection appears to be essential (19, 22-24). Prognostic factors might help define groups of patients, which benefit most from surgical therapy. Patients with melanoma stage IV and ocular origin tend to have better survival when compared to patients with cutaneous origin. In accordance with previous reports, the time interval between first operation and metastasectomy, as well as the number of metastases were of prognostic value (8, 18, 2-23). Younger patients seem to benefit most from aggressive surgical approaches (23). Patients' age and factors related to tumor biology, histology, time interval between initial operation and number of metastasis, might help to decide whether to operate or not (8, 18, 20-23).
In conclusion, this is the first case-matched controlled analysis in melanoma stage IV indicating survival benefits for patients scheduled for liver resection additional to multimodal therapy concepts. Recall bias is certainly a common concern and a major limitation in case-control studies; however, it has also been documented for prospective cohort, as well as randomized controlled trials. Resection remains an individual decision and the necessary therapeutic approaches should be discussed in interdisciplinary boards. However, prognostic models and algorithms might indeed help in deciding which patients benefit most from liver resection as an additive tool in multimodal therapy for melanoma stage IV.
Predictors for survival of the surgically-treated study populations and non-surgically treated study population (N=32 patients).
Predictors for survival of the surgically-treated study population (N=16 patients).
Footnotes
-
* These Authors contributed equally to this study.
- Received July 2, 2014.
- Revision received August 12, 2014.
- Accepted August 19, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved