

Abstract
Aim: To evaluate the survival of patients with unresectable perihilar cholangiocarcinoma (PHC) treated with multimodal palliative approaches. Patients and Methods: thirty-two patients were enrolled in a multimodal protocol including: bilateral biliary drainage; Yridium-192 intraluminal brachytherapy (BT); metal biliary stenting; external-beam radiotherapy (EBRT); systemic chemotherapy (ChT). All patients underwent BT and biliary stenting: this was the only treatment for 14 patients, it was combined with EBRT in 11, and with EBRT and ChT in seven. Mean and median survival, complication rates and duration of hospital stay were calculated for each group. Results: BT with EBRT and ChT obtained the best median (15 months) and one year (71.42%) survival followed by BT with EBRT (14 months and 63.63%, respectively). BT with EBRT in a total dose of 54-60 Gy, with or without ChT, led to a significantly higher median survival rate (14 months) than that for BT alone (seven months). Conclusion: BT with EBRT, with or without ChT, improves survival and should be considered as a suitable alternative to palliative surgery for patients with unresectable perihilar cholangiocarcinoma.
- Biliary tract neoplasms
- brachytherapy
- radiotherapy
- Yridium radioisotopes
- expandable metallic stents
Cholangiocarcinoma (CCA) is a rare tumor of the bile ducts, with high local invasiveness and occasional distant metastases (1-3). Worldwide, it accounts for 3% of all primary gastrointestinal malignancies and 10% of primary hepatobiliary malignancies (4). The most commonly used classification of CCA identifies three groups based on the location along the biliary tree: intrahepatic CCA; perihilar CCA (PHC), also called Klatskin tumor; and distal CCA (5, 6). The intrahepatic CCA type accounts for fewer than 10% of the total cases, whereas the PHC and distal CCA types represent about two-thirds and a quarter of the cases, respectively (6). PHC can be defined as tumors arising above the junction of the cystic duct up to and including the second biliary branches of the right and left bile ducts (6). PHC has been divided into four types by Bismuth and Malt (1) according to the location and extent of the tumor, and this classification system was primarily conceived to serve as a guide for surgical strategy (6).
Due to the natural rapid progression of the tumor and its low chemosensitivity, surgery remains the gold standard for treatment. In past decades, only a minority of patients were surgical candidates, but surgical management of PHC has evolved since its original description. In fact, a large series recently reported in the literature showed resectability rates varying from 50 to 80% (7), with 1-, 3-, and 5-year overall survival rates of 74.4%, 47.3%, and 34.1%, respectively (7, 8). However, when unresectable at the time of diagnosis or metastatic at the first clinical observation, the mortality rate for untreated PHC ranges from 50 to 70% within 12 months (9); therefore, this category of patients can only undergo palliative treatment.
Given that the natural history of PHC is guided by liver complications rather than metastatic disease, local palliative treatments are a rational option. Many therapeutic protocols using radiotherapy [intraluminal brachytherapy (BT) and external beam radiotherapy (EBRT)] and chemotherapy (ChT) combined with biliary decompression have been advocated to provide with a resolution of the jaundice associated with the elective treatment of tumor stenosis (10-17). To date, the role of these therapies, still considered as experimental treatment options, is poorly defined since data from controlled clinical trials are lacking. Studies to support treatment recommendations are insufficient, mainly due to the low incidence of PHC, which has precluded large randomized studies examining the role of radiation and ChT.
The aim of the present study was to evaluate retrospectively the outcome and survival of multimodal treatment (drainage of the right and left biliary systems, Yridium-192 intraluminal BT, positioning of metallic stents and EBRT associated with systemic ChT) in unresectable PHC.
Patients and Methods
Patient population. From April 2003 to April 2010, 32 patients [22 male; mean age=68 years (range: 32-88 years)] with obstructive jaundice due to malignant biliary cancer were retrospectively evaluated.
Selective diagnostic work-up for PHC at our center includes the evaluation of liver function by routine biochemical laboratory tests, measurement of serum tumor markers [carcinoembryonic antigen (CEA) and CA19-9 levels and ultrasonography. All patients subsequently underwent the following diagnostic examinations: magnetic resonance cholangiopancreatography (MRCP) to evaluate stenosis location, morphology and extent (Figure 1A); abdominal computed tomography (CT) or magnetic resonance (MR) to detect hepatic, lymphatic or peritoneal metastases, and to detect arterial or portal infiltration (Figure 1B); percutaneous transhepatic cholangiogram (PTC) (Figure 1C) to define the precise extension of tumor infiltration, or to perform a biopsy for histological confirmation preliminary to the placement of internal biliary drainage (PTBD) to palliate jaundice (Figure 1D).
Resectability was determined by individual surgeons according to the following standard criteria: patients in poor clinical condition, or with bilobar hepatic disease, or with tumor invasion of the common or proper hepatic artery, or infiltration of the controlateral branch of the portal vein or of the hepatic artery (as determined at the time of abdominal imaging), or extra-hepatic disease (lymph node involvement and distant metastases) were considered inoperable.
According to the Bismuth and Malt classification (1), one patient (3.12%) had type I (considered inoperable for cardiovascular disease), one patient (3.12%) type II [judged non surgical due to advanced age (88 years) and immunologic disorders], nine patients (28.13%) type III B, 11 patients (34.38%) type III A, and 10 patients (31.25%) type IV tumors. Patient stratification according to the staging system proposed by Deoliviera et al. (6) is reported in Table I.
The mean total bilirubin value before biliary decompression was 12.35 mg/dl (range=0.48-33.13 mg/dl).
Multimodal treatment. PTC (Figure 1C) was performed for all patients, demonstrating malignant biliary stenosis and, in the same session, an intraluminal forceps biopsy was carried out in the main ductal stenosis to obtain histological confirmation of PHC; the percutaneous procedure was completed by placing unilateral (in five patients: 15.62%) or bilateral (in 27 patients: 84.38%) internal-external biliary drains (Figure 1D). Detailed PTC also defined the exact radiation field of the subsequent intraluminal BT, corresponding to a cylindrical volume of 2 cm in diameter with a length including the whole neoplastic stenosis plus a proximal and distal tumor-free margin of 15 mm; this strategy is indicated for the control of any submucosal tumor frequently undetected at cholangiography (Figure 1E).
Patients' baseline characteristics according to the classification system proposed by Deolivera et al.
One to two days after PTBD placement, BT was performed by inserting, within the right or both the right and left internal biliary drains, Yridium-192 sources in two consecutive weekly sessions (on days 7 and 14) with a dose of 7 Gy each (total dose 14 Gy) or of 4 Gy each (total dose 8 Gy).
All patients underwent PTC, PTBD and BT, in 29 patients (90.63%) with a total dose of 14 Gy and in three patients (9.37%) with a total dose of 8 Gy. The dose of BT was chosen according to the patients' liver function and general clinical condition.
After BT, for all patients, the biliary drains were percutaneously replaced with bilateral bare metallic stents (Wallstent; Boston Scientific, Medi-Tech, Watertown, MA, USA) with diameters ranging from 7 to 10 mm (Figure 1F); in 5 cases (15.62%) unilateral and in 27 (84.38%) bilateral stents were placed. In 18 patients (56.26%), once a decrease in bilirubin level ≤2.0 mg/dl was obtained without liver decompensation, EBRT was also performed two weeks after the end of BT in five week cycles (46 Gy; 25 administrations of 1.8 cGy each). After the EBRT, in 7 patients (21.87%) only, who maintained normal liver function, systemic ChT was also administered: 3/7 (42.86%) received 5-fluorouracil (300 mg/day at week 1 and 5 during EBRT), 1/7 (14.28%) gemcitabine and oxaliplatin (gemcitabine 1000 mg/m2 at day 1 and oxaliplatin 100 mg/m2 at day 2 every 14 days), 2/7 (28.58%) capecitabine (500 mg ×2/day every day) and 1/7 (14.28%) gemcitabine alone (1000 mg/m2 at day 1, 8 and 15 every 28 days).

Klatskin's III a tumor. A: Magnetic resonance cholangiography. B: Abdominal magnetic resonance showing a thrombosis of the right hepatic artery (arrow) and infiltration of the right portal vein (arrowhead), thus confirming tumor unresectability. C: Percutaneous transhepatic cholangiogram confirms the diagnosis and is followed by bilateral internal biliary drainage positioning (D). E: Brachytherapy planning, with a measuring catheter inserted percutaneously within the biliary drainages. F: Two self-expandable bare stents inserted after the completion of brachytherapy treatment.

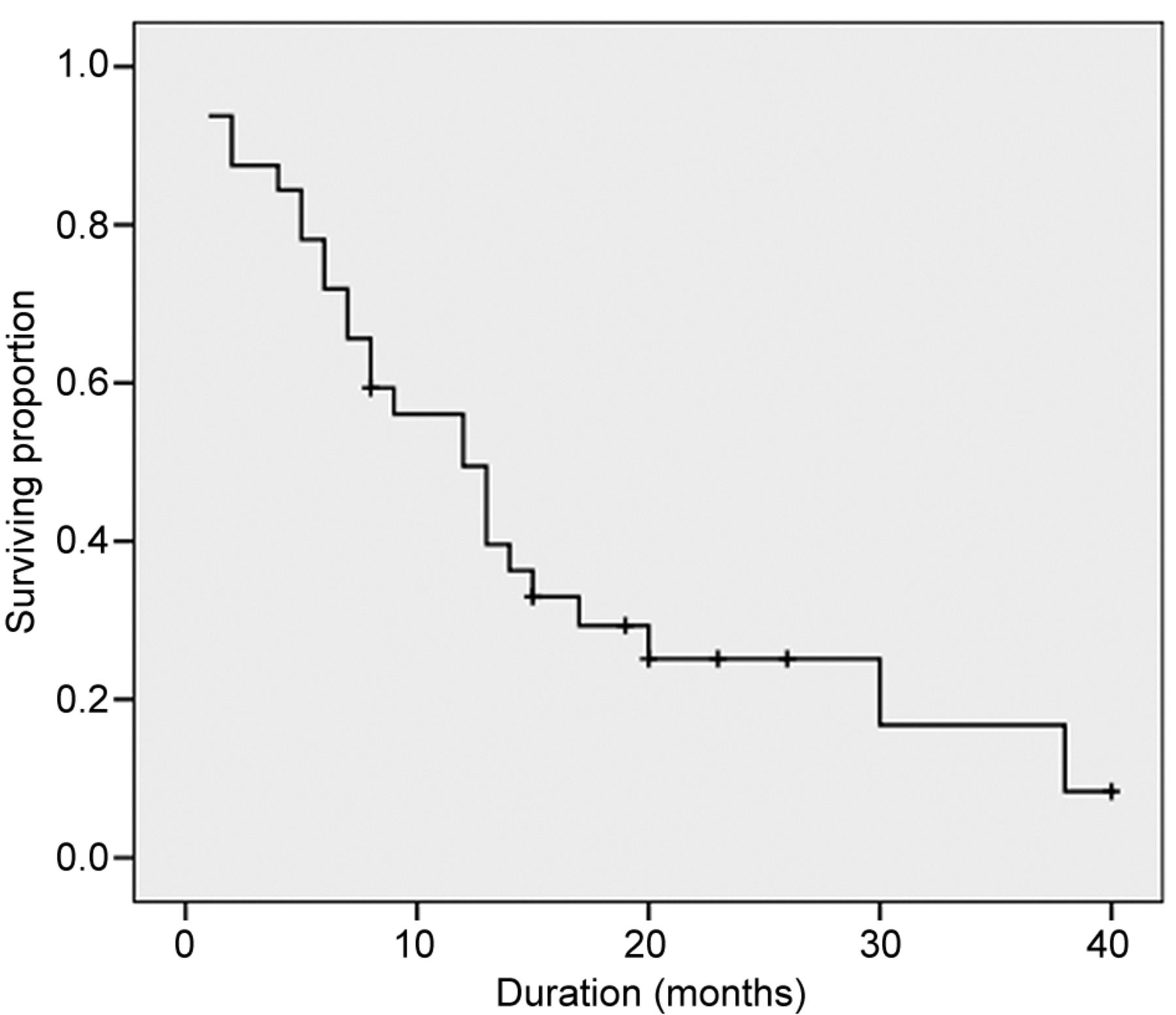
Survival of the entire study population.
Therefore, the patient population was divided into three groups, according to the completion of the protocol: group A (14 patients=43.75%) received only BT without EBRT or ChT; group B (11 patients=34.37%) received BT plus EBRT without ChT; group C (seven patients=21.88%) received BT, EBRT and ChT.
The patients subsequently underwent follow-up with laboratory tests and ultrasound examinations every three months; the mean follow-up was eight months (range=1-16 months).
Statistical evaluation. Statistical analysis was carried out with the SPSS (v. 13.0, SPPS, Chicago, USA). Survival curves were estimated by the Kaplan–Meier method which provided mean and median survival of the overall group and of each individual group. Comparisons of the curves were made using the log rank test and the Breslow test. A p-value <0.05 was considered statistically significant.
Results
All patients had complete remission of jaundice after biliary drainage, BT and stent positioning.
No patient developed acute complications from BT or EBRT during the first two weeks. Generally, ChT was reasonably well-tolerated and all patients completed the intended treatment course.
Severe post-radiotherapy complications (digestive hemorrhage and hepatic abscess development) occurred in one patient (3%), five months after EBRT, leading to the death of the patient.
The median survival of the entire population was 12 months (range=7.76-16.24 months) (Figure 2). Cumulative 6-month and 1- and 2-year mean survival rates were 78.12%, 53.12 % and 15.62%, respectively.
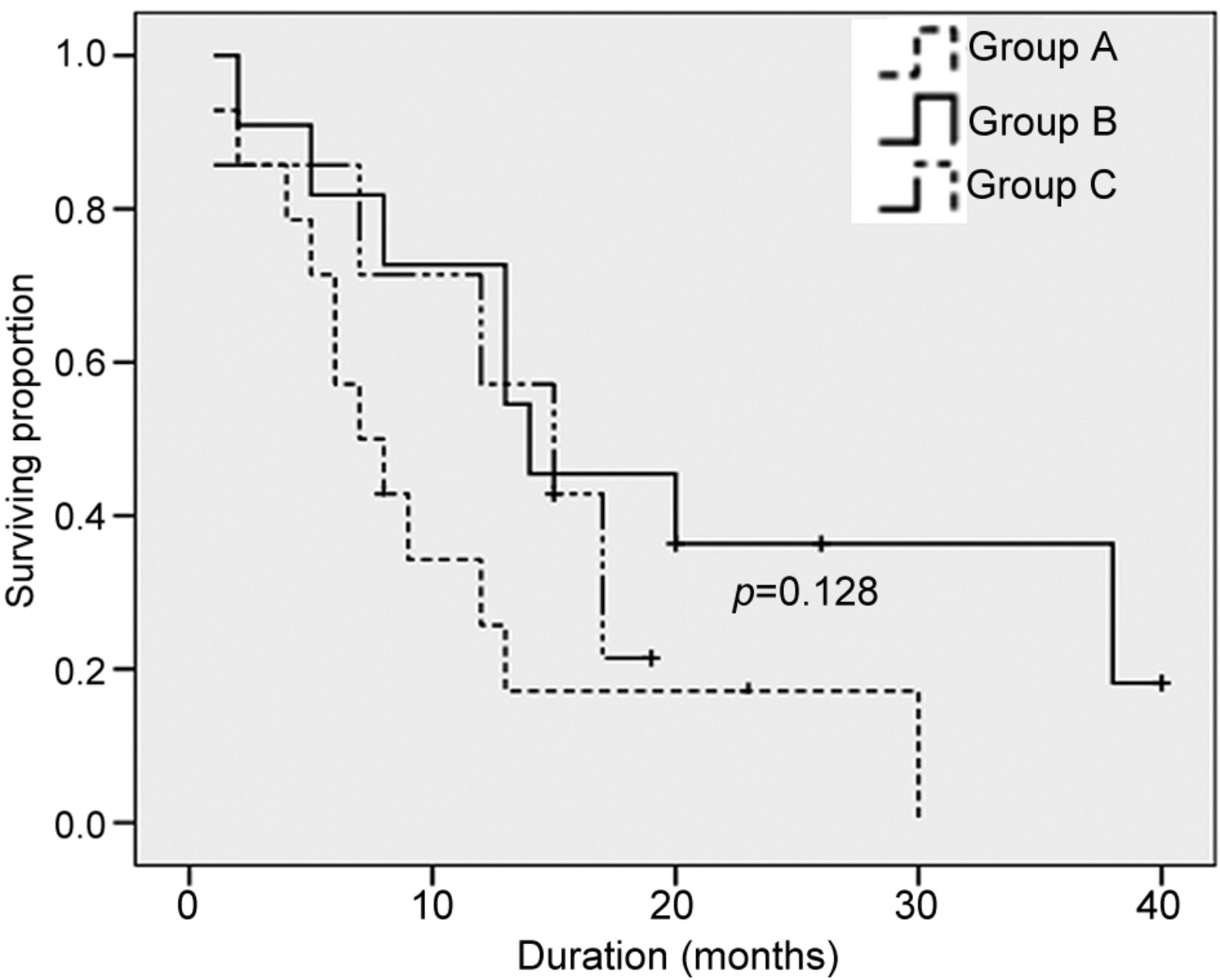
Kaplan-Meier median survival curves for the three groups, according to the therapy protocol (p=0.128): group A (14 patients=43.75%) treated only with brachytherapy (BT) without external -beam radiotherapy (EBRT) or systemic chemotherapy (ChT), group B (11 patients=34.37%) with BT plus EBRT without ChT and group C (seven patients=21.88%) with BT, EBRT and ChT.
The median survival rate for group A (14 patients who received only BT) was seven months (range=3.33-10.66 months); for group B (11 patients who underwent BT with EBRT without ChT) 14 months (range=4.28-23.71 months); and for group C (7 patients who underwent the complete protocol of BT, EBRT and ChT) 15 months (range=7.3-22.69 months): the differences among the three groups were not statistically significant (p=0.128) (Figure 3).
Mean 6-month and 1- and 2-year survival rates were 57.14%, 28.57 % and 7.14% for group A; 81.81%, 63.63% and 27.27% for group B and 85.71%, 71.42% and 0% for group C, respectively.
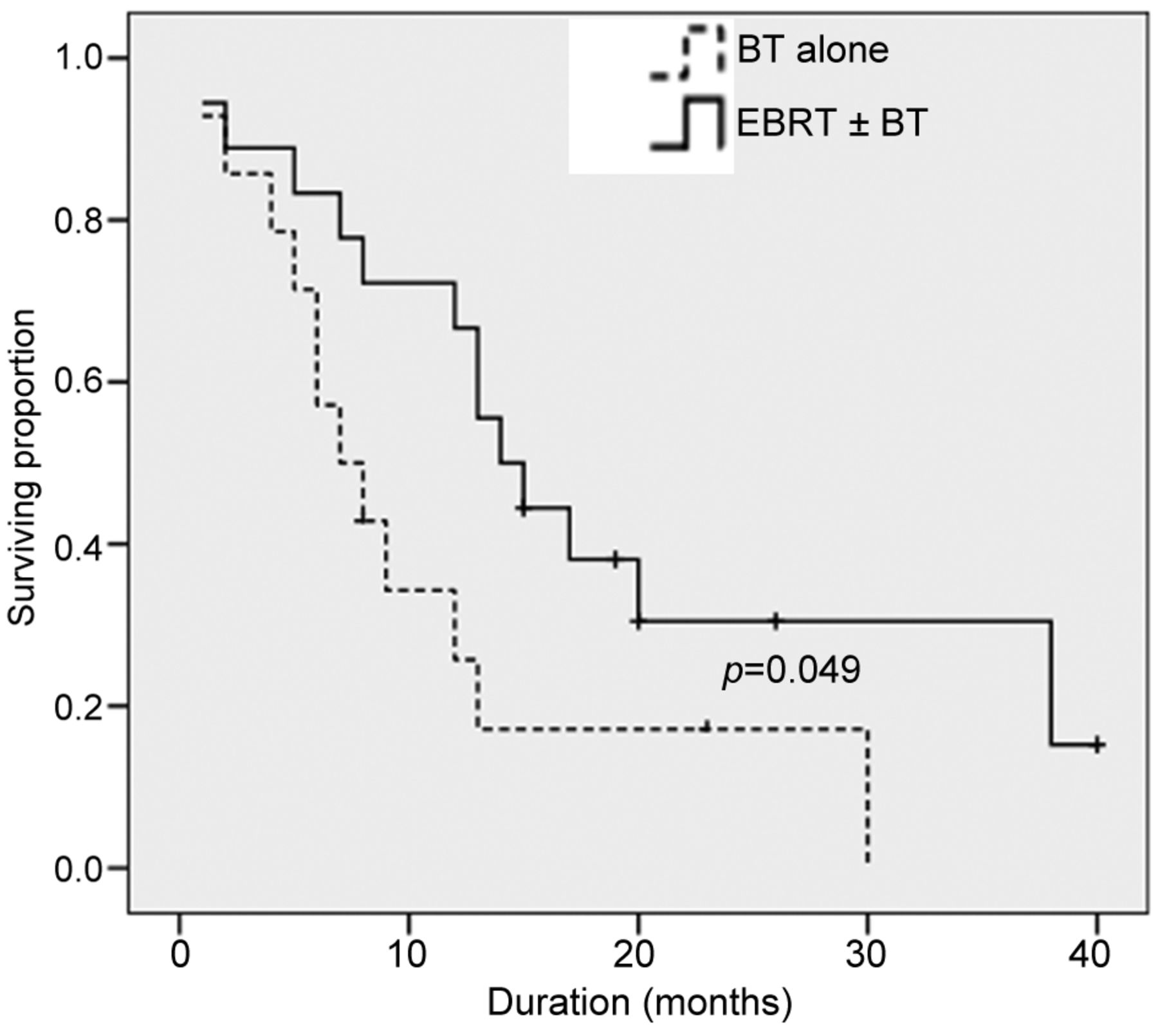
On univariate analysis, the patients who received BT with EBRT (groups B and C) with or without ChT (n=18) had a median survival of 14 months (range=9.84-18.15 months), significantly higher (p=0.049) than that of seven months (range=3.33-10.66 months) for patients treated with BT alone (group A) (Figure 4). By comparing the survival of patients who received BT and EBRT (group A and B: median=12 months; range=7.4-16.59 months) with those who underwent the complete protocol (median=15 months; range=7.3-22.69 months), no statistically significant differences were observed (p=0.77).
Age, gender, type of PHC, BT dose and bilirubin levels before treatments were not found to affect patient outcomes.
Twenty-seven patient deaths (38%) were cancer-related, while three patients (9.38%) died from other causes (two from cardiovascular disease and one from post-radiotherapy complications), and the cause of death was not assessable in one patient (3.12%). One patient (3.12%) was alive at the last follow-up.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier median survival curves for the patients in groups B and C [treated with brachytherapy (BT) and external-beam radiotherapy (EBRT), with or without chemotherapy (ChT)] and those in group A (who received BT without EBRT and ChT) with statistically significant difference between the two groups (p=0.049).
The mean duration of hospital stay (excluding the period of EBRT and ChT) for the entire cohort was 15 days (range 8-17 days), without differences among the groups; EBRT and ChT were performed during day-hospital admission.
Four patients (12.5%) required a percutaneous revision of the metallic stent due to stenosis as a result of tumor in-growth after the completion of the protocol (median=14 months; range=5-19 months); a stent-in-stent procedure was carried out, successfully restoring stent patency.
Discussion
The clinical outcome of patients with PHC is poor. Surgery is the only curative treatment modality, with reported 5-year survival rates of 27 to 44% (9). In the past, only a minority of patients were considered to be surgical candidates with curative intent; the more recent advancements in surgical options have increased resectability rates up to 50-80% of cases (7). In PHC unresectable at the first clinical observation, due to local spread or to distant metastasis, the mortality rate within 12 months, ranges from 50 to 70% (9). For patients with unresectable disease, the goal of treatment is the prevention of locoregional disease progression to enhance survival and the quality of life. In the past, the most common palliative treatment was surgical biliary-enteric anastomosis to control jaundice; in recent years, a percutaneous approach with the placement of metallic covered or uncovered stents has replaced surgery, due to patency rates comparable to those of surgical bypass and with similar patient survival but lower complication rates. In previous studies (16, 17), comparisons of outcomes, survival and duration of hospital stay for surgical palliation, percutaneous bare-metal stent alone or associated with Yridium 192 BT, or combined within a multimodal protocol of BT, EBRT and ChT were carried out. In these series, the group of patients who completed the entire protocol had survival rates (10 months) similar to the surgical group (10.5 months), higher than the groups treated with BT plus biliary decompression (six months) and those treated with metallic stenting alone (2.75 months). The multimodal percutaneous protocol can lead to survival (up to 10 months) similar to that after a surgical bypass, with a shorter hospital stay and a better quality of life.
However, the application of radiation therapy to PHC remains controversial in general, with several studies showing no benefit from the radiation (18, 19). Conversely, many studies (10-14, 16, 17, 20-22) have demonstrated an improvement in survival with the use of radiation therapy as compared to supportive and palliative procedures alone, although long-term survival is rare. However, many previous studies are limited by small sample size, lack of concurrent ChT administration in some patients, possible group imbalance with regard to the extent of disease, adverse histological features and variable radiation therapy techniques.
Compared to the historical data of patients with PHC treated without any kind of radiation (survival of 2.5 months) (17), our results demonstrated an improvement in median survival in the entire patient population treated with BT, reaching a median of 12 months, including those who received EBRT and ChT in addition and those without other therapeutic options.
Our data are also in accordance with a recent study of Shinohara et al. which demonstrated a median survival of 11 months in patients who received BT with or without EBRT, against a median survival of four months in patients who did not undergo radiation therapy (15).
Our study confirms the statistically significant superiority of the combination of intraluminal BT and EBRT, with or without ChT, in improving survival over treatment with BT alone (14 vs. seven months). Similarly, Alden and Mohiuddin (23), in 48 patients, compared ChT-alone to ChT added to EBRT and BT and, similarly, they obtained a median survival rate of 12 months with the combined treatment and of 5.5 months with ChT-alone (p<0.01). A retrospective study of Takamura et al. (21) showed a median survival rate of 11.9 months in 93 patients with unresectable PHC treated with a combination of EBRT and BT (without ChT). More recently, Ghafoori et al. (24), in 37 patients with unresectable PHC treated with a combination of EBRT, BT and ChT, obtained a median survival rate of 14 months with 1- and 2-year survival rates of 59% and 22%, respectively.
There are several advantages when performing intraluminal BT instead of, or combined with, EBRT in the treatment of PHC. EBRT dosage is limited by its toxicity to the normal surrounding tissues, and the field often encompasses portions of the liver, kidneys, spinal cord and bowel, all of which can affect the total dose which can be safely administered. The potential advantages of intraluminal BT include the administration of high radiation doses with rapid dose fall-off over a short distance from the radioactive source, thus sparing adjacent normal tissue and localizing the full dose to the tumor and peritumoral tissue, although the dose to the extratumoral disease may also be limited.
Furthermore, BT, with or without EBRT, has also been reported to provide durable palliation, also favoring the maintenance of stent patency for patients with locally advanced PHC (21, 25). In our study, 32 patients underwent metallic biliary stent placement and only four (12.5%) required stent revision for symptomatic biliary obstruction after the completion of the protocol.
The optimal radiation dose for the treatment of biliary malignancies represents a hot point which still needs to be defined. Alden and Mohiuddin (23) demonstrated a 2-year overall survival rate of 48% for doses >55 Gy and a 2-year overall survival rate of zero when doses of <55 Gy were used. Takamura et al. (21) treated unresectable PHC with EBRT of 50 Gy and BT with a dose of 27-50 Gy (mean dose, 39.2 Gy), obtaining a median survival rate of 11.9 months and an overall survival rate of 4.3% at five years.
In the present study, we demonstrates the improved survival rate of patients receiving a combined radiation dose of 54-60 Gy (using BT plus EBRT) compared to those exposed to doses of 14 or 8 cGy using BT alone.
At present, systemic ChT achieves poor disease control, and its role for patients with advanced PHC has not yet been clearly established. Some small phase II studies [with a predominance of 5-fluorouracil (5-FU) or gemcitabine-containing regimens] showed that these tumors were poorly chemosensitive (26) but no single-regimen had been adopted; until recently, 5-FU-based regimens appeared to produce responses of 10-20%, while gemcitabine-based regimens produced responses of 20-30% (26). More recently, a randomised phase III ABC-02 study showed a survival advantage for combined cisplatin and gemcitabine ChT over gemcitabine monotherapy (median survival of 11.7 vs. 8.1 months) (27).
The role of ChT in combination with radiation therapy for localized bile duct carcinomas remains ill-defined; the use of 5-FU-based ChT in combination with radiation is extrapolated from the survival benefits demonstrated in other gastrointestinal malignancies, including pancreatic cancer (28). The number of patients reported to be receiving combined therapy is too small to draw definitive conclusions regarding the benefit of concurrent ChT delivery and the different types of chemotherapeutics produce conflicting results (24, 29, 30). Results from our series failed to show an improvement in survival in patients who received ChT when compared to those who received radiation therapy alone. However, our data are insufficient to draw definitive conclusions since, in our study as well as in the others (24, 29, 30), the number of patients receiving ChT was very small and the type of chemotherapeutic used was different.
Our study has limitations due to the retrospective collection of the data, which implies slightly different therapeutic regimens, and to the small number of patients; therefore, our results should be interpreted critically. Moreover, the optimal radiation dose for BT has not yet been fully established, and three patients of our series had a sub-optimal BT radiation dose; by increasing the dose of BT to >14 Gy, the survival advantages would probably have been even better.
Our study has a further bias due to the completion of protocol which was achieved only in patients with better clinical conditions and good liver function, which, per se, could have influenced survival. However, in our unselected study population, all patients underwent BT and almost 50% of them underwent BT with EBTR or the complete protocol.
In conclusion, for unresectable PHC, a multimodal treatment consisting of high dose (up to 60 Gy) radiation therapy obtained by combining intraluminal BT and EBRT, followed by percutaneous metallic stent positioning and combined with systemic ChT represents the state-of-the-art regimen. This protocol achieved significant improvement in overall survival, low morbidity and a short hospital stay, and represents a valid substitute for surgical palliation. However, prospective randomized trials are still needed to adequately determine which patients may benefit from this approach.
Footnotes
-
Conflicts of Interest
There are no conflicts of interest.
- Received April 16, 2013.
- Revision received May 4, 2013.
- Accepted May 9, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved