

Abstract
Background: Few data are published on docetaxel toxicity in obese patients. Patients and Methods: All obese patients (n=100) treated for early breast cancer during three consecutive years at our Institution, were retrospectively investigated. The same number of non-obese patients was randomly selected and used as controls. We assessed the factors predictive of the relative dose intesity (RDI) reduction, including body composition. Results: A total of 18% (n=18) of obese patients and 5% (n=5) of non-obese patients required reduction of docetaxel RDI due to toxicity (p=0.008). In a multivariate analysis, body mass index (BMI) and age were predictive of a reduction in RDI. Among the 89 patients with a determination of body composition, patients with a higher fat mass more frequently had a reduction in docetaxel RDI (p=0.002). In multivariate analysis, fat mass was the only independent factor predictive of a reduction in docetaxel RDI. Conclusion: Obese patients treated for early breast cancer more frequently required a reduction in docetaxel RDI. Fat mass seems to be the best factor predictive of a reduction in docetaxel RDI.
- Early breast cancer
- docetaxel
- obesity
- fat mass
- dose intensity
- toxicity
Breast cancer is a common disease: 1.4 million women were diagnosed worldwide in 2008 (1). Adjuvant chemotherapy based on regimens using anthracyclines (doxorubicin, epirubicin) and taxanes (paclitaxel, docetaxel) has significantly improved survival for women with early breast cancer (2). These regimens are highly codified, and the dose intensity, is crucial for efficacy.
Nevertheless, these regimens are associated with haematological and non-haematological toxicities that remain unpredictable and which may alter the dose intensity of the treatment. Doses of chemotherapy are usually based on the body surface area (BSA), mostly calculated with the Dubois formula (3), which considers only weight and size. However, several studies have shown that the use of BSA for reducing the inter-individual variability of pharmacokinetic factors [clearance, area under curve] is efficient only for a small number of chemotherapy agents and not for epirubicin or docetaxel (4). Other factors may impact on the pharmacokinetics of drugs, including body composition (fat mass, lean body mass) (5), which may predict tolerance to chemotherapy (6, 7). In the era of personalised medicine, one of the main issues is the ability to adjust the dose of chemotherapy in cases of obesity.
The rate of obesity, defined by a BMI greater than 30 kg/m2, has been increasing in recent years both in developed and developing countries. With a prevalence of approximately 20% in the United States, the United Kingdom and Australia, obesity has reached epidemic proportions in Western countries (8). Regarding breast cancer, obesity is both a risk factor in post-menopausal women (9) and an indicator of a poor prognosis (10). Even if increasing numbers of obese patients are treated for breast cancer, few data exist on the adaptation of doses of chemotherapy for this sub-population. In daily practice, some physicians reduce doses for obese patients because of a fear of excessive toxicity (11), but without actual evidence-based data. Recently, the American Society of Clinical Oncology (ASCO) published guidelines on the adaption of chemotherapy doses for obese patients (12). The recommendation is not to reduce chemotherapy doses for obese patients because of the lack of evidence of increased toxicity in this population and the risk of reducing the efficacy of the treatment. Nevertheless, among the studies that contributed to these recommendations, none included chemotherapies with taxanes such as docetaxel.
In our daily practice, docetaxel appears to be less well-tolerated in obese patients, but to date, no study has evaluated the safety of this drug in obese patients. The aim of this retrospective study was to assess the toxicities of adjuvant chemotherapy for early breast cancer in obese patients. We also analyzed the potential for using body composition in the prediction of chemotherapy toxicity.
Patients and Methods
Study population. Every obese patient (BMI ≥30 mg/m2) who received adjuvant or neoadjuvant sequential chemotherapy for early breast cancer between 1 January 2008 and 31 December 2010 at the Henri Becquerel Center (France) was included. For comparison, the same number of non-obese patients (BMI <30 kg/m2) treated identically was randomly chosen from among all non-obese patients treated over the same period. The data on co-morbidities were collected (arterial hypertension, diabetes, cardiac diseases, respiratory insufficiency, and venous thromboembolism).
This retrospective study was approved by our Institutional Scientific and Ethic Committees, in accordance with the Declaration of Helsinki.
Tumour evaluation. The tumors were staged according to the Seventh TNM classification (2009) (13). A diagnosis of breast cancer was histologically-verified for each patient after breast biopsy or surgical excision. The tumours were considered hormone-dependent if hormone receptors were present in more than 10% of the tumor cells. The tumours were considered human epidermal growth factor receptor 2 (HER2) positive if the immunochemistry score was +++ or if HER2 was amplified by chromogenic in situ hybridization (CISH).
Chemotherapy. All patients were planned to receive a sequential chemotherapy of three cycles of FEC 100 (5-fluorouracil at 500 mg/m2, epirubicin at 100 mg/m2, and cyclophosphamide at 500 mg/m2) followed by three cycles of docetaxel (100 mg/m2) when treated with adjuvant chemotherapy and three to four cycles of FEC 100 followed by three to four cycles of docetaxel when treated with neoadjuvant chemotherapy. The chemotherapy was administered intravenously every 21 days.
The chemotherapy doses were calculated based on BSA, using the Dubois formula with the actual body weight: BSA (m2)=0.007184 × height (cm)0.725 × weight (kg)0.425. The BSA was limited to 2 m2, as is standard at our Institution.
In cases of excessive toxicity, treatment adaptations during chemotherapy were decided by our multidisciplinary staff and usually consisted of dose reductions, change of regimen (FEC recovery after docetaxel toxicities), or chemotherapy disruption.
Supportive care. Supportive care during chemotherapy followed the guidelines of daily practice at our Institution. Treatment with granulocyte colony-stimulating factors (G-CSF) was administered as recommended by the European Organisation for Research and Treatment of Cancer (EORTC) in 2007 (14). Erythropoietin-stimulating agents (ESA) were initially indicated in cases of symptomatic anaemia (Hb <10 g/dl), as recommended by ASCO in 2007 (15), but the use of ESA gradually stopped, as recommended by the FDA in 2008 and ASCO in 2010 (16).
To prevent docetaxel-related hypersensitivity or fluid retention, the patients received pre-medication with six doses of corticosteroids (equivalent to 50 mg of prednisolone) starting at 12 h before and ending at 24 h after docetaxel infusion.
During epirubicin and docetaxel infusion, the patients wore a frozen helmet to reduce the risk of alopecia, and during docetaxel infusion, the patients wore frozen gloves to reduce the risk of ungual toxicity.
Toxicity evaluation. At baseline and at the end of the chemotherapy, a complete biological assessment was carried out, including evaluation of liver function, renal function and albumin level.
The tolerance to chemotherapy was evaluated before each cycle. A clinical examination and a complete blood count were performed before each cycle. The haematological toxicities were evaluated from the complete blood count performed systematically the day before chemotherapy or in the case of fever, and were graded according to the national cancer institute common terminology criteria for adverse events (NCI CTCAE) version 4.0 (17). The cardiac toxicity was monitored by radioisotopic methods or by echocardiogram at baseline and every two cycles of FEC 100.
Non-haematological toxicities were not systematically determined because of the risk of bias in the evaluation of such toxicities when assessed retrospectively. Nevertheless, the type of toxicity that led to a reduced dose intensity of chemotherapy was determined.
Information on unplanned hospitalisations was also collected.
Dose intensity evaluation. All events modifying the dose intensity were collected, i.e. dose reductions, delayed chemotherapy, changes in regimen or chemotherapy disruptions.
The dose intensity was evaluated by calculating the relative dose intensity (RDI) (18). RDI=Received dose intensity (mg/m2/week) / planned dose intensity (mg/m2/week) for each drug. These data were collected from our centralized database. The reason for reductions of the dose intensity were also recorded.
Body composition evaluation. Since mid-2009, computed tomographic (CT) scanning is routinely performed at our Institution after a diagnosis of invasive breast carcinoma. When available, the analysis of body composition was performed with this initial staging CT scan and was performed on a cross-section centered on the third lumbar vertebra (L3) using dedicated LITIS EA 4108 software developed in our laboratory. This software was developed to allow for automatic contouring of muscles and fat (sub-cutaneous and visceral) based on specific Hounsfield units (HU) for each tissue: −29 to 150 HU for muscle, −190 to −30 HU for sub cutaneous fat and −150 to −50 HU for visceral fat (19). This automatic contouring was manually corrected by the same reader before calculating the area of each tissue (cm2) on the L3 cross section (Figure 1). The calculation of fat-free mass (FFM) and fat mass (FM) was performed on the muscle and fat on the L3 cross section using the following formulae (19): FFM (kg)=0.30 × [muscle L3 cross-sectional area] + 6.06 and FM (kg)=0.042 × [fat L3 cross-sectional area] + 11.2
Twenty-five of these patients underwent two independent fat contourings to ensure the reproducibility of the analysis.
Follow-up. The duration of follow-up was calculated from the date of diagnosis to the date of the last follow-up visit.
Statistical analysis. The non-obese patients were randomly chosen with the R software (http://www.r-project.org/) using a model of a draw without replacement. Comparisons between the different groups of patients were performed using the Chi-square test, t-test or Mann-Whitney test. Multivariate analysis of predictive factors was performed according to a multiple regression model with the backward method. Statistical analyses were performed using the medical software MedCalc® (Ostend, Belgium).
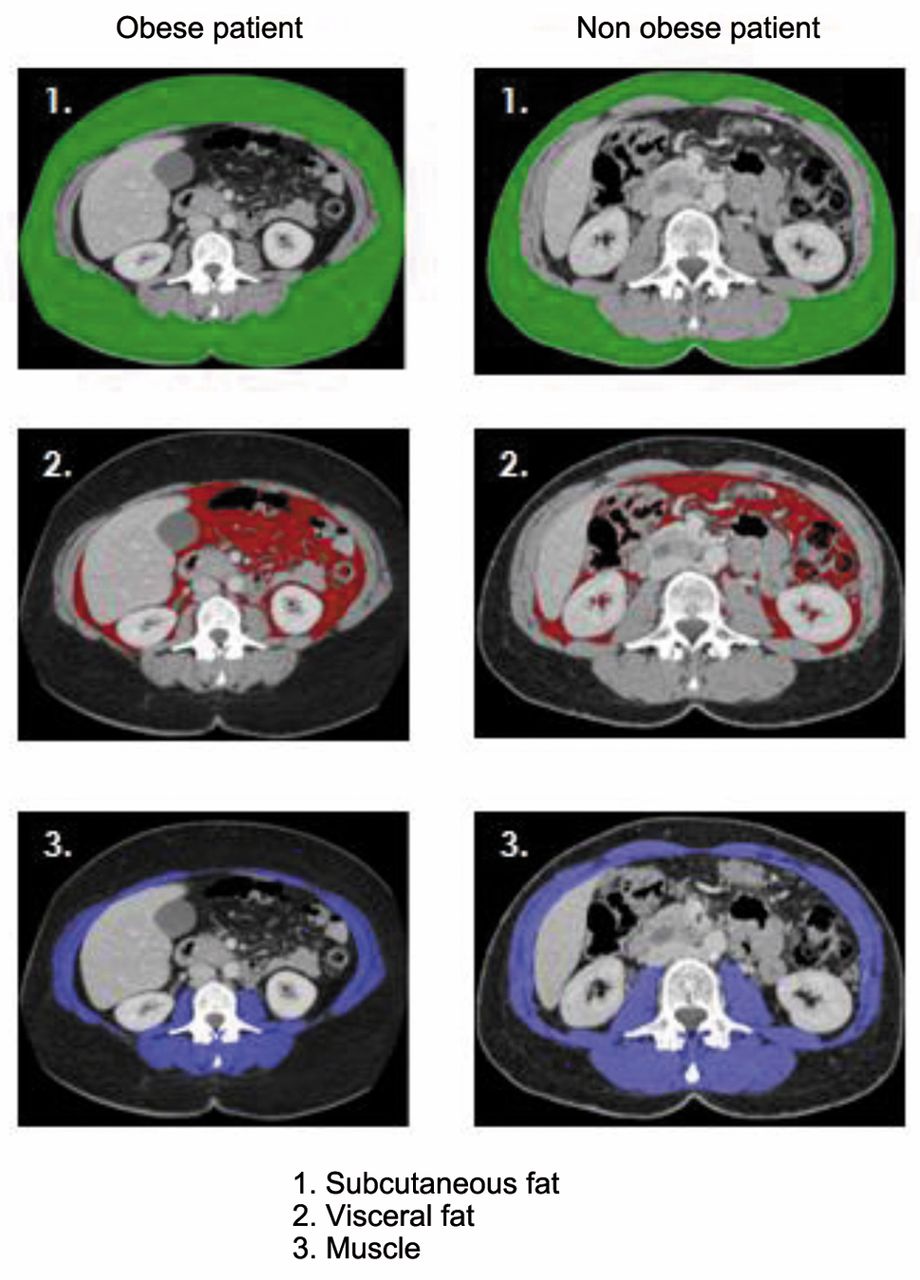
Body composition analysis with a computed tomographic scanning.
Results
Patients' characteristics. Between 1 January 2008 and 31 December 2010, 469 patients were treated with adjuvant or neoadjuvant sequential chemotherapy (FEC100 followed by docetaxel) for early breast cancer at our Institution. Among them, 100 were obese (21%), and 369 (79%) were non-obese. From the non-obese patients, 100 were randomly chosen for the comparisons performed in this study.
Clinical characteristics. The clinical characteristics were not different between the two populations, except for weight, BMI, BSA, and the number of co-morbidities. There was no difference between the two populations in age and time-to-follow-up (Table I).
Among the obese patients, 71 had a BSA≤2 m2, and 29 had a BSA>2 m2 (15 patients between 2.01 and 2.10 m2, 9 patients between 2.11 and 2.20 m2 and 5 patients between 2.21 and 2.30 m2). There were 57 patients with a BMI between 30 and 34 kg/m2, 35 patients with a BMI between 35 and 39 kg/m2 and eight patients with a BMI>40 kg/m2. None of the non-obese patients had a BSA>2 m2.
Biological characteristics. There was no difference between the two groups in the following biological characteristics: Albumin, renal function and alteration in liver function (data not shown).
Tumor characteristics. The two groups were significantly different regarding tumor grade; grade II was more frequent in the obese population, and grade III was more frequent in the non-obese population. Inflammatory breast cancer (T4d stage) was also more frequent in the obese population. There was no difference between the two groups in regards to other histological criteria (Table I).
Body composition. Among the 200 patients, 89 patients (50 obese and 39 non-obese) had a CT scan at baseline. The characteristics of these sub-groups were not different compared with the total population of obese and non-obese patients included in this study (data not shown). Two independent contourings for 25 patients showed good reproducibility of the body fat evaluation (coefficient of correlation of 0.99, p<0.001). The body composition analysis confirmed that obese patients had both higher lean body mass and higher fat mass than non-obese patients (Table I).
Treatment characteristics. The total doses of chemotherapy were higher for epirubicin in obese patients (600 vs. 507 mg, p<0.0001) and for docetaxel (580 vs. 498 mg, p<0.0001). Obese patients more frequently received neoadjuvant chemotherapy (25 vs. 14%, p=0.07) than non-obese patients, but this trend was not significant. This difference may be explained by the higher number of obese patients with T4d tumours, which were treated with neoadjuvant chemotherapy. The median number of chemotherapy cycles was six for both obese and non-obese patients. Four patients did not receive the planned number of cycles: three obese patients (two patients received five instead of six cycles, and one patient received four instead of six cycles) and one non-obese patient (five instead of six cycles).
Chemotherapy. FEC 100 toxicities: Grade III-IV neutropenia was significantly more frequent in non-obese patients; it was the only toxicity that was significantly different between the two groups. However, there was no difference between the two groups in febrile neutropenia. No other haematological toxicity was different between obese and non-obese patients (Table II). Three obese patients had cardiac toxicity (left ventricular ejection fraction <50%): two patients during trastuzumab treatment without clinical symptoms and one patient with late toxicity with clinical symptoms who did not receive trastuzumab. No cardiac toxicity was found in the non-obese population. Overall, this difference in cardiac toxicity was not statistically significant. No toxic deaths occurred during the cycles of FEC 100.
Baseline patients' characteristics.
Chemotherapy toxicities.
Factors predictive of reduction of the docetaxel dose intensity in the entire population (n=200).
Factors predictive of reduction of the docetaxel dose intensity in the population with a computed tomographic scanning (n=89).
FEC 100 dose-intensity: In the present study, 622 cycles of FEC100 were administered to the entire patient population. Only one dose reduction (of 25%) was required (at cycle 2 due to haematotoxicity), and no change in regimen, cure delay, or chemotherapy disruption was observed. Thus, there was only one patient (who was obese) with a reduction of the epirubicin dose intensity (epirubicin RDI <1).
Docetaxel toxicities: No significant difference was observed in haematological toxicities (Table II) between the two groups. No toxic deaths occurred during docetaxel cycles.
Docetaxel dose-intensity: In this study, 587 cycles of docetaxel were administered. Among the entire population, 23 patients (11.5%) required reduction of the docetaxel dose intensity (docetaxel RDI<1). Reductions of the docetaxel RDI were significantly more frequent in obese patients than in non-obese patients (18 vs. 5%, p=0.008). Reductions of the docetaxel RDI were never related to cure delay but were always due to dose reductions, changes in regimen or chemotherapy disruptions (Table II).
In the obese population, the reduction of the docetaxel dose intensity was due to 10 dose reductions (10 to 25%), five changes in regimen (FEC100 recovery in the five cases) and three chemotherapy disruptions. In the non-obese population, reductions were due to two dose reductions (10 and 25%), two changes in regimen (FEC 100 recovery in the two cases) and one chemotherapy disruption.
The reported causes for reduction of the docetaxel dose intensity were mainly mucositis or cutaneous toxicities. In the obese patients, we found 10 cases of cutaneous toxicity (associated with mucositis in four cases), three cases of arthralgia, two cases of rectocolitis, one case of febrile neutropenia despite G-CSF, one infection and one weight loss. In the non-obese patients, we found four cases of cutaneous toxicity, including one case associated with mucositis and one case of infection. For the obese patients, these toxicities and the related reduction of dose intensity occured at cycle 1 for 14 patients and at cycle 2 for four patients. For the non-obese patients, they occured at cycle 1 for four patients and at cycle 2 for one patient.
At our Institution, the doses of chemotherapy are calculated with a BSA that is capped at 2 m2. In this study, 29 (14.5%) out of the 200 patients had a BSA>2 m2, all of these patients were obese. Because of capping, we achieved a median empirical reduction of 5% (0.5 to 15%) for patients with a BSA >2 m2. Nevertheless, six additional reductions of the docetaxel dose intensity were observed in these 29 patients. When comparing the 71 obese patients with a BSA ≤2 m2 and the 29 obese patients with a BSA >2 m2, no differences in rates of reduction of docetaxel dose intensity were observed (20.3 and 26.1%, respectively, p=0.9).
Factors predictive of reduction in docetaxel dose intensity. Predictive factors in the entire population (n=200): In the univariate analysis, there were four factors predictive of a docetaxel RDI less than 1: Advanced age, higher BMI, higher BSA and higher body weight. The number of co-morbidities and alteration of hepatic function tests were not predictive of a docetaxel RDI less than 1 (Table III).
In the multivariate analysis, two factors were predictive of diminution of the docetaxel RDI: Age (p=0.04) and BMI (p=0.02).
Patients with a CT scan (n=89): We performed an analysis of the subgroup of patients for whom a CT scan was available (50 obese and 39 non-obese). In the univariate analysis, there were five factors predictive of a docetaxel RDI less than 1: higher fat mass, higher BMI, higher BSA, higher number of comorbidities and higher body weight. Age, FFM and alteration of hepatic function were not predictive of a docetaxel RDI less than 1 (Table IV).
In the multivariate analysis, the FM was the only factor predictive of a docetaxel RDI less than 1 (p=0.004), whereas BMI was not retained by the model. The docetaxel RDI according to the FM is represented in Figure 2.
Discussion
In the present study, we performed a retrospective comparison of the dose intensity of chemotherapy in 100 obese and 100 non-obese patients receiving a sequential treatment of an epirubicin regimen (FEC) followed by docetaxel for the treatment of early breast cancer. We showed that the tolerance to chemotherapy and the dose intensity of chemotherapy with an epirubicin-based regimen or with docetaxel in obese and non-obese patients were different.
After the FEC100 regimen, the rate of grade III-IV neutropenia was more common in the non-obese population (25% vs. 10%, p=0.009), but the rate of febrile neutropenia did not differ between the two groups. These data are consistent with the studies of Jenkins et al. (20) and Rosner et al. (21), which showed that haematological toxicities were not higher in obese patients treated with FEC60 or CAF (cyclophosphamide, adriamycin and 5-fluorouracil), respectively. In our study, cardiac toxicity occurred in three patients (1.5%), all of whom were obese, but the difference between obese and non-obese patients was not significant, perhaps due to the small number of patients. These results are also consistent with data from the retrospective study of Fumoleau et al. (22), which showed that BMI was a factor predictive of cardiac toxicity associated with epirubicin (1.8% in obese patients vs. 0.9% in non-obese patients, p=0.03) in the treatment of early breast cancer. Overall, only one patient (1%) had an epirubicin RDI less than 1 in the obese population, which suggests that the tolerance to FEC100 in obese patients allows for maintenance of the dose intensity of this protocol. These findings are consistent with the ASCO recommendations of 2012 (12). ASCO recommends the use of full doses of chemotherapy and the use of actual body weight to calculate chemotherapy doses for obese patients (as is performed for non-obese patients) because there is no evidence of increased toxicity in the short-term or long-term in this population.

{kind=link}
{kind=link}
Docetaxel relative dose intensity according to fat mass.
In contrast, docetaxel was less tolerated in obese patients, 18 obese patients had a docetaxel RDI of less than 1, compared to five non-obese patients (p=0.008). Furthermore, this difference in tolerance may have been underestimated due to capping of doses for the 29 obese patients with a BSA >2 m2 and also because this was a retrospective study. The reasons for lowering the dose intensity (for obese or non-obese patients) were often cutaneous toxicities and mucositis. This finding of increased toxicity of docetaxel in obese patients, which led to a decrease of the dose intensity, was in opposition to the ASCO recommendations, previously mentioned (12). Indeed, the recommendations are not to reduce the dose of chemotherapy in obese patients. However, these recommendations are based on studies that examined first-generation chemotherapy regimens such as CMF (23, 24) or anthracyclines (20, 21) but not taxanes. Moreover, most of these studies were limited to haematological toxicities, but other side-effects can also affect the dose intensity of chemotherapy, as shown in our study. We found only one study with data on docetaxel dose intensity in obese patients treated for early breast cancer. De Azambuja et al. (25) studied retrospective data from the BIG 02-98 trial (26). This study included 365 obese patients who received docetaxel (75 or 100 mg/m 2). No significant difference was found in docetaxel dose intensity between obese and non-obese patients (95 vs. 96%, p=0.72). However, docetaxel toxicity was different with a dose of 75 mg/m2 from that with a dose of 100 mg/m2, as seen in our study. Unfortunately, the number of patients treated with the more toxic docetaxel dose of 100 mg/m2 (27) is not known. Furthermore, the characteristics of the patients included in this type of trial are often different from those of patients in daily practice, particularly in terms of co-morbidities, which are more frequent in daily practice.
Therefore, we question whether BSA is an accurate tool for calculating the docetaxel dose for obese patients and why obese patients tolerate docetaxel less than non-obese patients.
Chemotherapy is used at a ‘threshold dose’ to achieve optimal efficacy while maintaining acceptable tolerance. Renal clearance and AUC are two parameters correlated with efficacy of docetaxel and tolerance to docetaxel (28). Adjusting the dose of docetaxel by using the BSA should reduce the inter-individual variability of docetaxel pharmacokinetics. However, this method is not able to reduce inter-individual variability of clearance (4) and AUC (29) of docetaxel. In addition, Sparreboom et al. examined 162 obese patients for whom the body weight was used to calculate the BSA, and this increased the AUC of docetaxel by 33% (p=0.004) compared with non-obese patients (5). Overall, using the BSA is not the optimal method for calculating the dose of docetaxel required for obese patients.
An alternative method for calculating the dose of docetaxel would take into account body composition. Indeed, a few studies have shown that body composition was an independent determinant of chemotherapy tolerance (6, 7). In the present study, a high FM, evaluated by CT scan, appears to be an independent factor for predicting docetaxel toxicity. Several hypotheses could explain this result. The volume of drug distribution (Vd) is a pharmacokinetic parameter that is more often altered in obese patients (30, 31). FM increases more than lean mass in these patients (32). The increase of the ratio between FM and lean body mass leads to an increase in the Vd of lipophilic drugs such as docetaxel. Sparreboom et al. (5) showed that the Vd of docetaxel in obese patients was two-fold higher than the Vd of docetaxel in non-obese patients. An increase in the Vd may lead to docetaxel accumulation in the fat, with the risk of its late release. In fact, increased Vd results in an increased half-life and thus increases the toxic effects of docetaxel. Conversely, at a constant dose, an increase in Vd is responsible for a decrease in plasma concentration and may reduce docetaxel efficacy. In summary, an increase of FM could increase the risk of toxicity but also reduce the efficacy of docetaxel. We can, therefore, speculate whether the results of the main clinical trials for the treatment of early breast cancer are applicable to an obese population. We have found only one published study which suggests that the docetaxel regimen is less effective in obese patients (28). In phase III clinical trials of adjuvant chemotherapy in early breast cancer, the BMI of the patients was not always reported, but the patients included in clinical trials have fewer co-morbidities and may have lower BMIs than patients in daily practice.
Conclusion
This study confirms that the FEC 100 regimen is well-tolerated in obese patients doses of FEC should not be reduced in this population. However, this study also shows that docetaxel is less tolerated in obese patients and is associated with a significant decrease in dose intensity. Using the BSA is not a suitable method for calculating the dose of docetaxel required. In contrast, we have shown that the evaluation of FM by CT scan may be a promising tool for predicting tolerance to docetaxel. Additional studies examining obese patients are needed to evaluate tolerance to docetaxel and the efficacy of docetaxel in this population, and to identify a better method for dose calculation of docetaxel by exploring the pharmacokinetics of this drug.
Footnotes
-
Conflicts of Interest
None declared.
This retrospective study was approved by the Committee of Clinical Research Centre Henri Bacquerel on January 15, 2013, with the registration number No. 150113.
- Received September 29, 2013.
- Revision received October 27, 2013.
- Accepted October 29, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved