

Abstract
Extraskeletal chondrosarcoma (ECS) is a rare malignant neoplasm of bone or soft-tissue origin, characterized by the presence of spindle cells admixed with well-differentiated cartilage or chondroid stroma. A case of ECS is reported in a 102-year-old woman who presented with a painful swelling of 2 cm in the left buccal vestibular area. Orthopantomography was insignificant. Biopsy and histopathological examination revealed a tumor composed of an undifferentiated small round cell component that surrounded a myxoid matrix of malignant cartilage. Immunohistochemical studies showed the tumor cells to be positive for nuclear S-100 protein immunostaining, focally positive for vimentin and synaptophysin, and negative for epithelial membrane antigen, desmin, chromogranin, Leu-7, glial fibrillary acid protein, actin muscle-specific, cytokeratin, carcinoembryonic antigen, and CD99 (MIC2). The proliferative index (MIB-1) was 20%. The tumor was treated by surgery with wide margins. There was no evidence of disease at one-year follow-up. This report presents a very rare case of ECS of the left buccal mucosa of the maxilla, and describes the histological characteristics and the immunoprofile.
- Chondrosarcoma
- extraskeletal tumor
- myoxoid tumor
- buccal mucosa
Extraskeletal chondrosarcoma (ECS) is a malignant tumor with cells that produce a cartilage matrix; it usually arises in the peripheral long and flat bones (1, 2). It was first described by Stout and Verner in 1953 (3), and was classified as a distinct clinicopathological entity by Enziger and Shiraki in 1972 (4). It accounts for approximately 10-20% of malignant bone tumors (2). It is also known as soft-tissue chondrosarcoma because of its tendency to occur at extraskeletal locations; approximately one third of tumors have been found in soft tissue.
Chondrosarcomas are categorized, based on their osseous location, as central, peripheral, or juxtacortical (periosteal) lesions. Central chondrosarcomas are intramedullary in origin, although large tumors may erode the cortex and invade the surrounding soft tissue. Peripheral chondrosarcomas are subdivided into those secondary to a pre-existing osteochondroma and those arising from the bone surface (juxtacortical).
Histologically, they are subdivided into numerous types, including conventional intramedullary, clear cell, juxtacortical, myxoid, mesenchymal, de-differentiated, and extraskeletal. The conventional intramedullary chondrosarcoma is the most frequent type, and most commonly involves the long bones or pelvis in up to 65% of cases.
ECS are very rare neoplasms, less common than their intraosseous counterparts and represent approximately 2% of all soft-tissue sarcomas (5-7). The histological types of lesions that account for ECS are myxoid, mesenchymal, and very rarely, low-grade. ECSs occur commonly in middle-aged adults, the mean age at presentation being approximately 50 years; they usually develop in the deep parts of proximal extremities and in limb girdles (4, 8). There is some disagreement regarding gender distribution, with some studies indicating equal prevalence among both sexes (6), while others report a male predilection (8-10). Clinically, ECS appears as a painful mass, with swelling and neurological problems, depending on the tumor location.
ECSs metastasize primarily to the lungs, but osseous and soft-tissue metastases have also been reported (8, 9). We present a case of ECS and analyze its histological and immunohistochemical profile.
Case Report
A 102-year-old Caucasian woman presented with a 7-month history of swelling and pain in the left maxillary area. Clinical examination revealed a firm swelling approximately 2×2 cm, in the vestibular portion of the left maxillary area, with surrounding soft-tissue changes. Orthopantography was not significant (Figure 1). A biopsy was taken, and the histopathological examination indicated ECS. The patient underwent surgery of the left vestibular buccal mucosa. No signs of recurrence were noted at one-year follow-up.
Orthopantomogram. Detail of the initial orthopantomogram, absence of the tumor mass of the left maxilla.
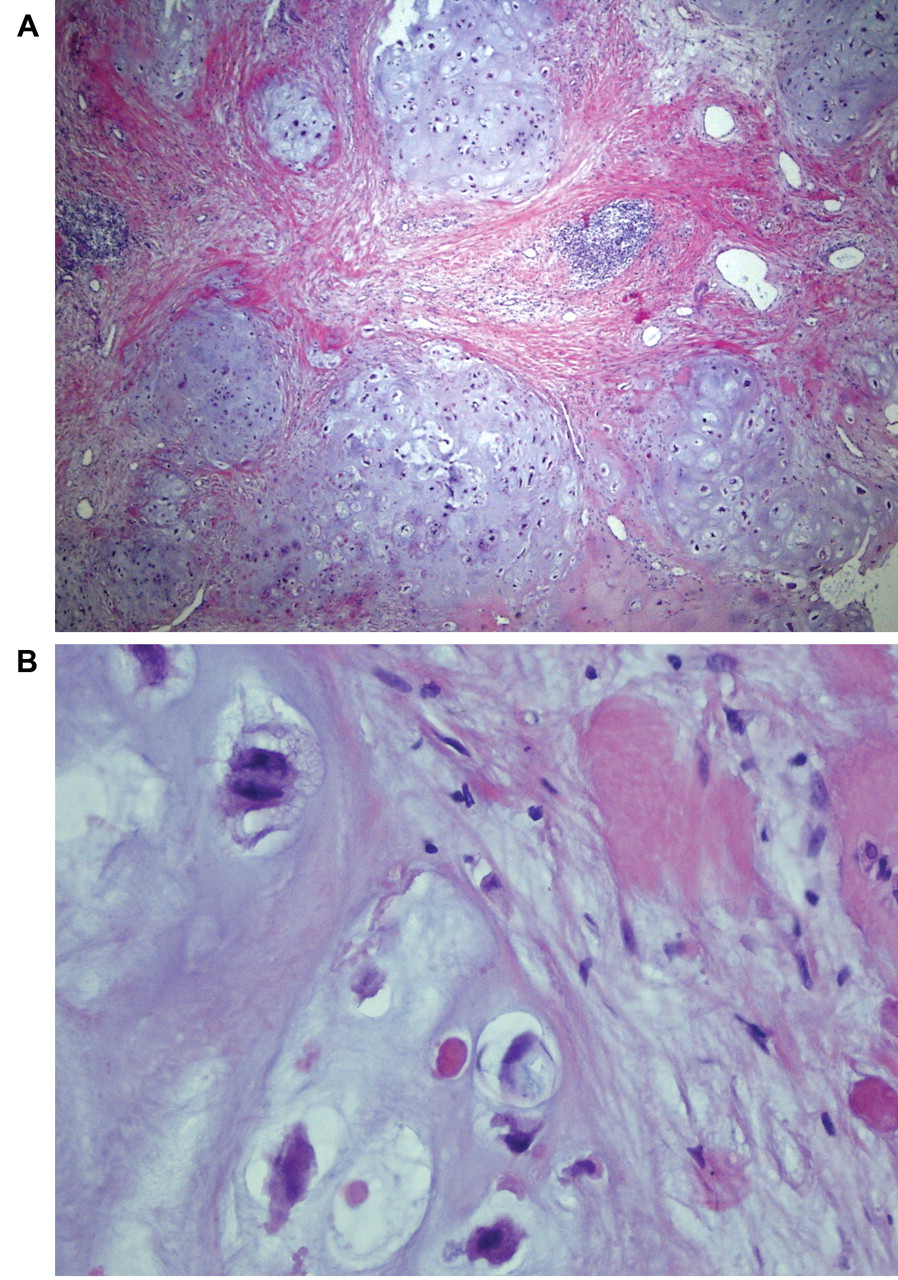
Histopathological examination of the excised lesion confirmed the presence of an ECS: homogeneous stroma, primarily hyalinized and focally chondroid, predominated. Within the stroma, epithelial cells, arranged in strands and small islands, were widely dispersed; cellular atypia and infiltrative growth were identified (Figure 2A). Areas of atypical cartilage with hyperchromatic and occasionally binucleated cells were seen. However, there appeared to be very few mitoses, and necrosis was absent (Figure 2B). On the basis of these findings, a diagnosis of ECS was rendered.
Immunohistochemistry. Immunohistochemical studies were performed on 4-μm thick sections following the avidin-biotin-peroxidase complex system. Appropriate positive and negative controls were used for each antibody listed in Table I. Immunohistochemical analysis determined the presence or absence of stain in a focal or diffuse pattern. Focal reactivity was defined as fewer than 25% of cells reactive for a specific antibody.
Results
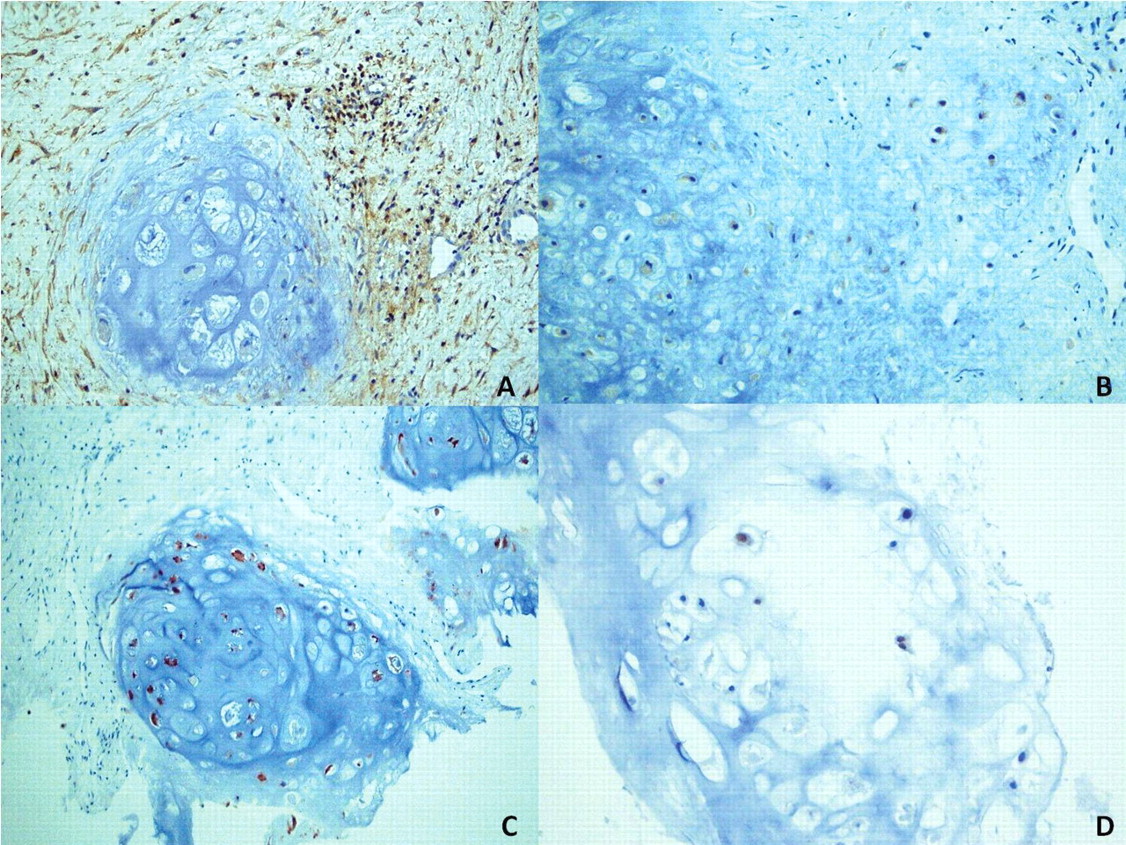
The tumor cells were positive for the S-100 protein nuclear immunostaining. Vimentin and synaptophysin were focally expressed; a lack of immunoreactivity was found for epithelial membrane antigen, desmin, chromogranin, glial fibrillary acid protein, smooth-muscle actin, cytokeratins AE1-AE3, carcinoembryonic antigen. Stroma, but not the tumor matrix exhibited reactivity for Leu-7 and CD99. The proliferative index MIB-1 was 20% (Figure 3A-D).
Discussion
Soft-tissue sarcomas are a group of rare malignancies originating from the mesenchymal tissue. This type of cancer has historically been described as slow-growing and late to metastasize, with 10-year survival rates ranging from 65 to 78% (11, 12).
The histopathological and clinical features of ECS are distinctive regardless of the site of origin. In the head and neck, it often produces symptoms early, and they may differ from those occurring in the deep and soft tissue. Our case had the histological features characteristic of classical ECS, cellular foci devoid of myxoid matrix, and reminiscent of chondroblastoma.
The histological differential diagnosis for ECS distinguishes it from a variety of lesions, including chondrosarcoma with fibrosarcomatous metaplasia, osteosarcoma, chondroblastoma, synovial sarcoma, and Ewing's sarcoma. The presence of multiple foci of hyaline cartilage, whether well-differentiated or atypical, within a cellular proliferation of small undifferentiated cells, is considered diagnostic for ECS. However, cartilage may not be identified in the initial biopsy specimens (1% to 50%) (13-15); the cartilage may be absent or inconspicuous, and in such a situation a misdiagnosis may be rendered.
Immunohistochemistry may be useful in refining the diagnosis of ECS. The hyaline cartilage seen in ECS may resemble the primitive chondroid of chondroblastoma; however, evidence of anaplasia and atypical mitoses among the lesional cells is more consistent with ECS. Similarly, osteosarcoma of the jaw frequently has chondroblastic differentiation, causing confusion with chondrosarcoma (16, 17). However the absence of neoplastic osteoid tissue, neoplastic bone, and of alkaline-phosphatase-expressing tumor cells made chondroblastic osteosarcoma very improbable. The latter type of tumor often contains chondroblastic areas with highly pleiomorphic chondrocytes (18); distinguishing ECS from chondroblastic osteosarcoma is often difficult.
Immunohistochemical profile of current case of Extraskeletal myxoid chondrosarcoma.
Rarely, ECS may resemble malignant mesenchymoma (19), a tumor that reflects the divergent differentiation potential of primitive mesenchymal cells. Malignant mesenchymoma is characterized by the presence of at least two well-defined forms of sarcoma, of differential histogenetic stem-cell origin, other than fibrosarcoma or malignant fibrous histiocytoma (20, 21). As opposed to ECS, most cases of malignant mesenchymoma occur in middle-aged or elderly patients.
The immunohistochemical profile of this case (Table I) showed consistent positivity for S100, immunoreactivity in chondroid foci for vimentin and synaptophysin; these three antibodies were the most immunoreactive in this study. Neuroendocrine differentiation is common in chondrosarcoma, and has been reported in tumors with histological and molecular features of chondrosarcoma (21-23). Synaptophysin is a 38-kD transmembrane calcium-binding glycoprotein typically found in neuronal presynaptic vesicles (22) and is expressed by neuroendocrine- and neuroectoderm-derived cells (23-26). Immunoreactivity for chromogranin was lacking. Chromogranins are a group of acidic proteins present in neurosecretory granules (27) and expressed by most types of neuroendocrine tissues and their tumors (28). Its expression depends on the number of neuroendocrine granules present in the cells. Specimens were negative for EMA, a distinct membrane protein; tumor tissues were also immuno-negative for cytokeratin, as has been reported elsewhere (29, 30).
In this case, clinical information, including tumor location, and the described, immunostaining support a diagnosis of ECS. The low proliferative index as shown by Ki-67 (20%), i.e. low mitotic activity, appears to be associated with a good outcome.
The undifferentiated stromal cells of ECS typically express CD99 and vimentin, whereas S100 is usually more focally expressed in areas of cartilaginous differentiation (17). Because CD99 is also expressed in Ewing's sarcoma, the only distinguishing feature is the cartilaginous differentiation.
Grading was proven to be of prognostic value, although unfortunately differential diagnosis between low-grade chondrosarcoma and benign chondroid lesions is quite difficult, requiring the integration of clinical, radiological and histopathological information (31).
Chondrosarcomas are divided into three histological grades, depending on cellularity, nuclear staining (hyperchromasia) of the tumor cells, and size of the nuclei. McGrory et al. (32) suggest that ECS is an intermediate grade neoplasm with a tendency toward recurrence and metastasis: about half of all cases develop metastasis, with the most common metastatic sites being the lung, soft tissues, lymph nodes, bones and brain (32). As identified via multivariate analysis, Meis-Kindblom et al. (30) concluded in their review that the survival of patients with ECS is adversely affected by metastasis, but not by local recurrence (30).
Surgery is the principle treatment for soft-tissue sarcoma; the only curative option for ECS is early wide local resection, with or without radiation for localized disease (33, 34). To our knowledge, little has been reported in terms of examining responses to systemic therapy for disseminated disease in such cases (35).

A: Histological features of the tumor showing a lobulated myxoid pattern with absence of necrosis and rare atypical mitoses. The center of the tumor exhibits cartilaginous differentiation with the cytomorphological features of a chondroid tumor of low-grade of malignancy (hematoxylin and eosin, original magnification ×200). B: Photomicrograph demonstrating detail of the tumor, with round and spindle-shaped cells in a myxoid stroma (hematoxylin-eosin stain, original magnification ×400).

{kind=link}
{kind=link}
{kind=link}
A: Immunohistochemistry of CD99 showing positive immunoreactivity in the stroma, but not in tumor matrix (original magnification ×40). B: Immunohistochemistry shows focal positivity for synaptophisin (original magnification ×20). C: Immunohistochemistry showing positive immunoreactivity for S100 (original magnification ×20). D: Immunohistochemistry shows immunoreactivity for MIB-1 (original magnification ×20).
Grade I and II chondrosarcomas of the jaws and facial skeleton are usually treated by local resection, using 1.5 cm margins of bone and soft tissue. Neither chemotherapy nor radiotherapy is indicated as primary treatment. Conversely, grade III chondrosarcomas are treated with aggressive resection margins, of 3 cm in bone and 2 cm in soft tissue, followed by chemotherapy (24). Distant metastasis is usually rare; however, it can occur in high-grade, advanced, or recurrent cases of chondrosarcoma when it is usually to the lungs, sternum and vertebrae. The prognosis of chondrosarcoma of the jaws is poor compared to the one located found in the long bones. The cause of death is usually distant metastasis to lungs and bones (30).
Certain clinical features, such as tumor size, tumor location (proximal or at the extremities), the patient's age, and the presence of metastases, appear to be significant adverse prognostic factors for survival, although this has not been definitively ascertained. Five- 10- and 15-year survival rates of ECS are estimated as being up to 90%, up to 70% and up to 60%, respectively.
Conclusion
To our knowledge, very little has been published, to date, about ECS in the head and neck area. ECS is a low grade tumor, with a slow-growing course that is late to metastasize. However, an aggressive clinical course can occur, depending on the size of the tumor, whether it has high cellularity, anaplasia or rhabdoid features. Therefore a follow-up is clinically recommended, and the histological and immunohistochemical features are fundamental, since they are correlated with prognosis.
- Received April 25, 2012.
- Revision received June 25, 2012.
- Accepted June 26, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved