

Abstract
Background: It is unclear whether cisplatin-based concurrent chemoradiotherapy (CCRT) has the same effect on adenocarcinoma as on squamous cell carcinoma. Patients and Methods: We retrospectively analyzed data for 32 patients with stage IIB–IVA cervical adenocarcinoma who were treated with radiotherapy (RT) or CCRT. Fourteen patients were treated with RT, 8 with CCRT using cisplatin alone (CCRT-P), and 10 with CCRT using cisplatin plus paclitaxel (CCRT-TP). Results: Complete response was achieved in 7/14 patients in the RT group, 4/8 patients in the CCRT-P group, and 9/10 patients in the CCRT-TP group. Ten out of the 14 patients in the RT, 7/8 patients in the CCRT-P, and 2/10 patients in the CCRT-TP groups experienced locoregional recurrence. The 5-year overall survival rate in the RT, CCRT-P, and CCRT-TP groups was 7.1%, 25.0%, and 74.1%, respectively (p=0.0094). Conclusion: The present study demonstrated that CCRT-TP achieved much better local control for adenocarcinoma of the cervix, leading to a decrease in locoregional recurrence.
- Cervical adenocarcinoma
- chemoradiotherapy
- cisplatin
- paclitaxel
Squamous cell carcinoma is the most common histological subtype of cervical cancer, whereas adenocarcinoma only accounts for approximately 10%-20% of all cases. However, the incidence of adenocarcinoma is increasing (1, 2). Adenocarcinoma of the cervix has a worse prognosis than its squamous counterpart, particularly when cancer cells spread beyond the uterine cervix (3, 4). This is derived from the observation that adenocarcinoma is less sensitive to radiotherapy (RT) and chemotherapy, and has a tendency to spread into lymphatic drainage even at an early stage (5, 6). Despite the analysis and publication of various prognostic factors for adenocarcinoma, many studies have included heterogeneous patient subpopulations, and have involved small numbers of patients. Recently, Huang et al. reported that a relatively large series of patients with adenocarcinoma/adenosquamous carcinoma of the cervix primarily treated with RT had inferior outcomes compared to those with squamous cell carcinoma (7). With respect to concurrent chemoradiotherapy (CCRT) for adenocarcinoma of the cervix, because adenocarcinoma/adenosquamous carcinoma only represents approximately 10% of patients enrolled in the trials supporting CCRT, it is unclear whether cisplatin-based CCRT has the same effect on adenocarcinoma as does on squamous cell carcinoma (8-12). No large-scale studies have ever addressed this issue.
In the present study, we analyzed data for patients with stage IIB–IVA adenocarcinoma of the uterine cervix who were primarily treated with RT between 1983 and 2009 at our institution. CCRT was not a common practice between 1983 and 1996; however, it has been the standard treatment since 1997. CCRT using cisplatin alone (CCRT-P) was a routine regimen until 2002. Thereafter, we changed the chemotherapy regimen to CCRT using cisplatin in combination with paclitaxel (CCRT-TP) because of poor treatment outcomes. We analyzed the efficacy of CCRT for adenocarcinoma in each of these eras. The present study, although a retrospective analysis that includes a small series of patients, might provide useful information for designing appropriate treatment strategies.
Materials and Methods
We retrospectively analyzed clinicopathological data from the charts of 32 patients with stage IIB–IVA (FIGO 1994 classification) adenocarcinoma of the uterine cervix who were treated with RT or CCRT between 1983 and 2009 at the University of the Ryukyus Hospital. Pelvic lymph node (LN) enlargement was defined as enlargement over a short axis diameter of 1 cm assessed by pretreatment computed tomography or magnetic resonance imaging. Patients with para-aortic LN enlargement were excluded. All the patients were required to have an Eastern Cooperative Oncology Group (ECOG) performance status of ≤2; age ≤70 years; and adequate hematological (WBC count, 3,000-10,000/μl; hemoglobin, ≥9.0 g/dl, and platelet count, ≥100,000/μl), hepatic (bilirubin level, ≤1.5 mg/dl and aspartate aminotransferase/alanine aminotransferase, ≤2.5× the upper limit of normal), renal (creatinine clearance, ≥60 ml/min) and cardiac functions (normal electrocardiographic findings). Patients treated with RT alone were selected by the same eligibility criteria (i.e. FIGO stage, tumor size, pelvic LN enlargement, and laboratory data) for matched cases to both CCRT-P and CCRT-TP. All the patients provided their written informed consent in regards to the treatment. This retrospective study was approved by the Institutional Review Board of our university.
Patient characteristics.
The patients were treated with anterior-posterior and posterior-anterior parallel-opposed ports of external beam radiotherapy (EBRT). The ERBT dose was 50 Gy delivered in 25 fractions. The center shield (4 cm width at the midline) was set up after delivering 40 Gy. High-dose rate intracavitary brachytherapy (HDR-ICBT) was delivered three or four times at a frequency of once per week with a fraction dose of 6 Gy at point A. Low-dose rate intracavitary brachytherapy (LDR-ICBT) was delivered two or three times every two weeks with a fraction of 18-20 Gy at point A. For CCRT-P, the patients received 20 mg/m2 cisplatin for five days every three weeks concomitant with RT (13). For CCRT-TP, the patients received 50 mg/m2 cisplatin every three weeks and 50 mg/m2 paclitaxel weekly (14).
All the patients completed the planned CCRT. Acute and late toxicities were graded according to the Common Terminology Criteria for Adverse Events (CTCAE version 3.0) and the Radiation Therapy Oncology Group/European Organization for Research and Treatment of Cancer (RTOG/EORTC) criteria, respectively. Follow-up examinations were conducted every month for the first year, every other month for the second year, and then every three to six months subsequently. Kaplan–Meier life table analysis and the log-rank test were used to assess the survival rate. p-values <0.05 were considered significant.
Acute toxicities associated with CCRT-TP (CTCAE version 3.0).
Results
Fourteen patients were treated with RT from 1983–1996, eight with CCRT-P from 1997-2002, and 10 with CCRT-TP after 2003. Patients' characteristics are shown in Table I. The median follow-up period was 22 months (range: 7-86 months) for the RT group, 24 months (range: 6-75 months) in the CCRT-P group, and 41 months (range: 9-70 months) in the CCRT-TP group. The median number of chemotherapy courses was two courses (range: 1-5 courses) in the CCRT-P group, and two courses (range: 2-3 courses) in the CCRT-TP group. No statistically significant differences were observed in the distribution of stage, LN status, or other clinicopathological variables.
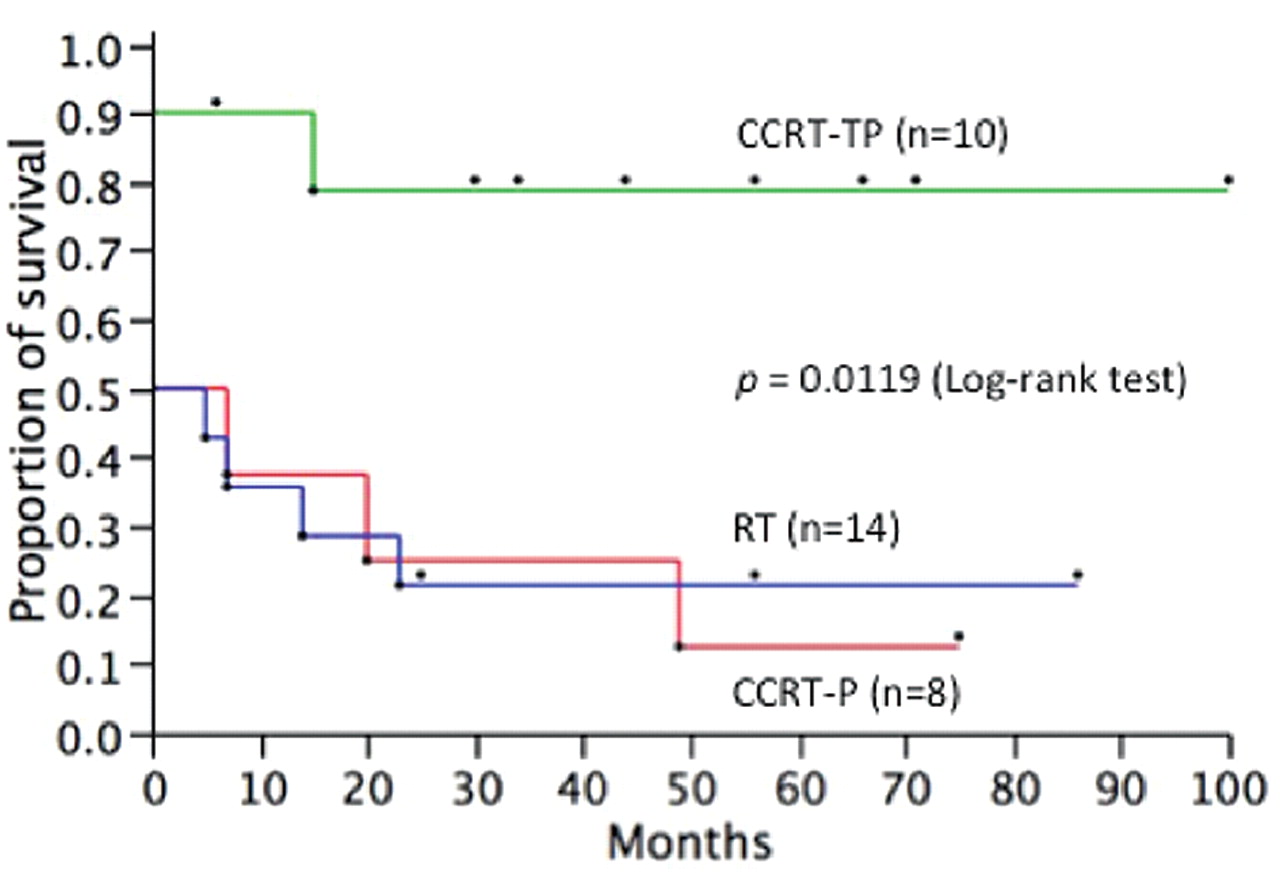
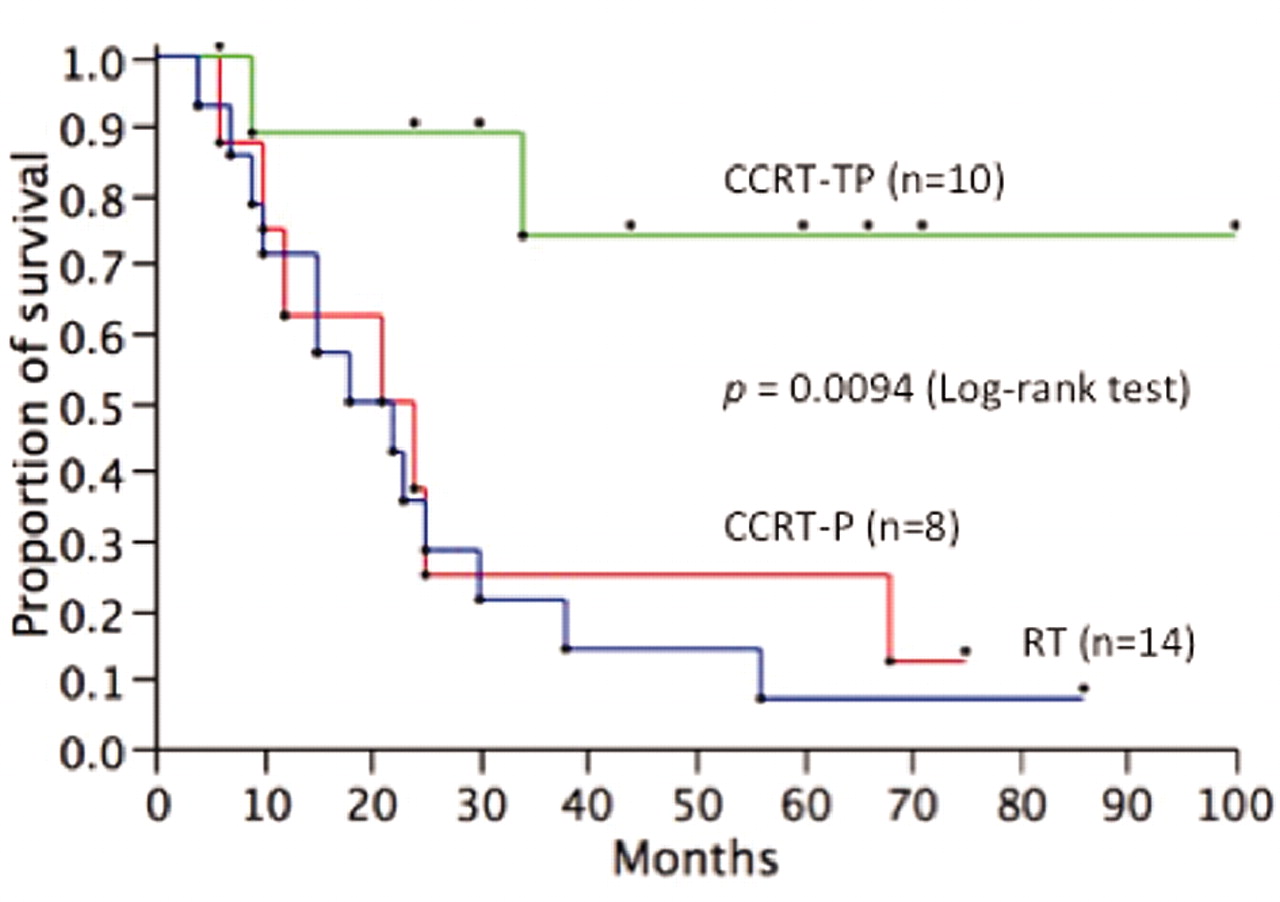
Complete response was defined as no clinically or pathologically viable cancer cells three months after completing CCRT. A clinically and pathologically complete response was achieved in seven out of the 14 patients (50.0%) in the RT group, four out of the eight patients (50.0%) in the CCRT-P group, and nine out of the 10 patients (90.0%) in the CCRT-TP group. Ten out of the 14 patients in the RT group, seven of the eight patients in the CCRT-P group, and 2 of the 10 patients in the CCRT-TP group experienced locoregional recurrence. Seven of the 14 patients in the RT group, 3 of the 8 patients in the CCRT-P group, and 4 of the 10 patients in the CCRT-TP group experienced distant recurrence. The 5-year overall survival (OS) rate in the RT, CCRT-P, and CCRT-TP groups was 7.1%, 25.0%, and 74.1%, respectively (p=0.0094) (Figure 1), their central disease-free survival (DFS) rate was 21.4%, 12.5%, and 78.8%, respectively (p=0.0119) (Figure 2), and the 5-year DFS rate in the RT, CCRT-P, and CCRT-TP groups was 0%, 12.5%, and 37.5%, respectively (p=0.0374). However, the distant DFS rate was 28.9%, 12.5%, and 37.5%, respectively (p=0.319).
The acute toxicities associated with CCRT-TP are shown in Table II. Only two patients (20%) had grade 3 neutropenia. None of these patients had febrile episodes, and there were no septic deaths. Anemia and thrombocytopenia were infrequent. Grade 3 diarrhea was reported in three patients. CCRT-TP was interrupted because of grade 3 diarrhea or sub-ileus in one patient. Regarding late toxicity of CCRT-TP, no grade 3/4 adverse effects were observed during the follow-up period. Two out of the 10 patients (12.5%) suffered grade 2 late intestinal toxicity (n=1) or grade 2 radiation cystitis (n=1) according to RTOG/EORTC scoring criteria.

Overall survival curve for each group (Kaplan-Meier method).
Discussion
The fact that adenocarcinoma of the cervix has a worse prognosis than its squamous counterpart is derived from the observation that adenocarcinoma is less sensitive to RT and chemotherapy. In the US, LDR-ICBT combined with EBRT is often performed. Eifel et al. (15) and Grigsby et al. (16) have reported that the treatment outcomes of adenocarcinoma of the uterine cervix are almost the same as those of squamous cell carcinoma using LDR-ICBT. However, these outcomes were applicable for disease stages IB to IIB. Grigsby et al. pointed out that the 5-year DFS rate after LDR-ICBT treatment of stage III adenocarcinoma of the uterine cervix (25%) was worse than that of the squamous cell carcinoma (59.1%). A report from Japan on a retrospective questionnaire survey of 61 patients with stage IIIb adenocarcinoma of the uterine cervix treated with HDR-ICBT combined with EBRT, which is the community standard treatment in Japan, showed that the 5-year OS rate of all the patients was 20.2% (17). In our series, seven out of the 14 patients (50.0%) achieved a complete response, 11 experienced locoregional recurrence, and seven experienced distant recurrence in the RT group. It is not likely that RT alone can result in good treatment outcomes for cervical adenocarcinoma.
{kind=link}
{kind=link}
Central disease-free survival curve for each group (Kaplan-Meier method).
With respect to cisplatin-based CCRT for adenocarcinoma of the cervix, because adenocarcinoma/adenosquamous carcinoma is only represented by approximately 10% of patients enrolled in trials supporting CCRT for cervical cancer (8-12), it is unclear whether cisplatin-based CCRT has the same effect on adenocarcinoma as it has on squamous cell carcinoma. No large-scale studies have ever addressed this issue. In a retrospective study, Huang et al. showed that the 5-year relapse-free survival rate forpatients treated with RT alone (n=45) and for those treated with CCRT (n=49) was 41.7% and 44.9%, respectively, in 94 patients with advanced-disease (stage IB/IIA bulky or greater) (7). No significant differences were found in disease-specific, local relapse-free, or distant relapse-free survival between the two groups. The study demonstrated that cisplatin-based CCRT did not improve the outcome of adenocarcinoma/adenosquamous carcinoma patients. In our patients, a complete response was achieved only in four out of the eight patients (50.0%), locoregional recurrence occurred in seven patients, and distant recurrence occurred in three patients in the CCRT-P group. The 5-year OS and central DFS rate were 25.0% and 12.5%, respectively, implying that CCRT-P did not improve the outcome of patients with adenocarcinoma of the cervix. The efficacy of paclitaxel as a chemotherapeutic agent in the treatment of gynecological malignancies has been well-documented, especially for adenocarcinomas of ovarian origin; the combination of paclitaxel and cisplatin has been evaluated as well in patients with recurrent and advanced cervical cancer (18). Therefore, we shifted our chemotherapy regimen to CCRT-TP.
Paclitaxel arrests cells in the radiosensitive G2M phase of the cell cycle and has been shown to be a radiosensitizer (19). Four out of seven cervical cancer cell lines have demonstrated radiosensitization with paclitaxel (20). Chen et al. reported the results of a phase I study of escalating doses of paclitaxel as a radiation sensitizer in combination with cisplatin (14). The results revealed a well-tolerated dose range starting at 10 mg/m2 weekly and advancing to 50 mg/m2 weekly in combination with 50 mg/m2 cisplatin every three weeks. A 93% response rate was observed in this study of previously untreated patients. In 2002, because of poor treatment outcomes, we shifted the chemotherapy regimen of CCRT for adenocarcinoma of the cervix to CCRT-TP. In our series, a complete response was achieved in nine out of the 10 patients (90.0%) in the CCRT-TP group, which was much better than that observed in the patients in the RT and CCRT-P groups. Only two out of the 10 patients experienced locoregional recurrence and four out of the 10 patients experienced distant recurrence. The 5-year OS, central DFS, and DFSrates were 74.0%, 78.8%, and 37.5%, respectively, which were significantly higher than those in the other groups, although the 5-year distant DFS rate was not significant. CCRT-TP seems to be a promising strategy for therapy of adenocarcinoma of the cervix.
For CCRT-TP, we used 50 mg/m2 cisplatin every three weeks and 50 mg/m2 paclitaxel weekly as a chemotherapy regimen according to the phase I study by Chen et al. (14), and the adverse effects were tolerable. To date, several phase I/II trials of cisplatin–paclitaxel and concurrent RT have been reported. Pignata et al. reported results of a phase I study of weekly cisplatin–paclitaxel and concurrent RT in 18 patients with cervical cancer, concluding that the maximum tolerated dose (MTD) of paclitaxel is 50 mg/m2/week with 30 mg/m2/week cisplatin and concurrent pelvic RT, while diarrhea is the dose-limiting side-effect (21). The Gynecologic Oncology Group (GOG) reported 35 patients with stage IB2, IIA, IIB, IIIB and IVA carcinoma of the cervix (all cell types) in a phase I/II study of RT with concomitant paclitaxel and cisplatin chemotherapy; 13 patients comprised the phase I component, and the MTD was determined to be 40 mg/m2 cisplatin and 40 mg/m2 paclitaxel administered weekly for six cycles with EBRT (22). A phase I study in Japan also reported that CCRT with weekly administration of 30 mg/m2 cisplatin and 50 mg/m2 paclitaxel can be considered a tolerable and safe dose for the treatment of locally advanced cervical carcinoma in Japanese women (23). Prasad et al. conducted a phase I trial of CCRT with weekly paclitaxel and cisplatin (30 mg/m2/week) and found the MTD of paclitaxel to be 40 mg/m2 (24).
The present study, although a retrospective analysis, with a small series of patients, demonstrated that CCRT-TP achieved much better local control for adenocarcinoma of the cervix, leading to a decrease in locoregional recurrence. These results might provide useful information for designing appropriate treatment strategies. Prospective trials in larger series of patients undergoing paclitaxel–cisplatin chemoradiotherapy, as well as other novel therapies, are urgently needed.
Footnotes
-
Conflict of Interest
We have no conflict of interest as to this article.
-
Financial Disclosures
There are no finances from any Authors.
- Received February 21, 2012.
- Revision received March 11, 2012.
- Accepted March 12, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved