

Abstract
Background/Aim: This study specifies a strategy to improve radiotherapy by partial synchronization of p53-deficient cancer cells (FaDu and H1299) in mitosis using taxol, with protecting p53 wild-type cells (A549) by the prior administration of cytostatic compounds. Cytotoxic and cytostatic effects of ionizing radiation, cisplatin, doxorubicin and taxol, administrated alone or in combination were investigated in vitro by flow cytometry. Results: A protective effect of doxorubicin but not cisplatin was found after administration of triple sequence with ionizing radiation and taxol. It was found that preliminary administration of doxorubicin induced growth arrest and protected A549 cells from the taxol/radiation treatment, while simultaneously killing FaDu and H1299 cells. Conclusion: The proposed therapeutic strategy allows protection of p53 wild-type cells and selectively increases radiosensitivity of p53-deficient cancer cells.
- Radiation
- chemotherapy
- cancer
- flow cytometry
- cell cycle
- p53
- A549
- FaDu
- H1299 cell lines
Non-small cell lung cancer (NSCLC), representing about 85% of all lung cancer, is one of the most frequent causes of cancer-related death (1). Unfortunately, the majority of patients are diagnosed with NSCLC in advanced inoperable stages and most of those who present with earlier disease will ultimately develop metastatic lung cancer (2). Radiotherapy has long been the standard therapy for locally advanced inoperable NSCLC (3). Although radiotherapy results in a modest improvement in patient survival, most patients experience disease (4). The overall 5-year survival for patients remains poor and the disease is still a clinical challenge (5). Therefore, new therapeutic strategies are needed. One of the strategies to improve local disease control is radiation sensitization. Because different chemotherapeutic agents are able to arrest cells at specific cell cycle checkpoints, researchers have explored their use to synchronize and arrest cells in the radiosensitive phases of the cell cycle (4). Development of NSCLC involves mutations in the tumor suppressor TP53 gene (6), with a mutation frequency of 50% in advanced diseases (7). These mutations were shown to be associated with a poorer survival prognosis and increased resistance to ionizing radiation and chemotherapy (8, 9). At the same time, the lack of wild-type p53 (p53wt, the product of TP53 gene) in cancer cells might be exploited to a therapeutic advantage by selective synchronization of p53-deficient (p53−/−) cancer cells in radiosensitive phases of the cell cycle and by protecting surrounding p53wt cells using a combination of radiotherapy and a sequence of antagonistic drugs (10). It was demonstrated that certain anticancer drugs, for example doxorubicin, could selectively arrest p53wt cells and thereby protect them from antimitotic agents. For example taxol, a potent chemotherapeutic agent, which simultaneously interferes with mitotic spindle function of p53−/− cancer cells, blocks cells at radiosensitive mitosis (11-13), improving the effects of subsequent radiotherapy. However, the sequence required in the combined radiochemotherapy of NSCLC is still under consideration. In this context, the overall goal of this work was to develop a protocol for the preliminary treatment, which increases the proportion of p53−/− cells but not p53wt cells present in radiosensitive mitosis in order to selectively kill p53−/− cells by subsequent radiotherapy. For this purpose, the effects of ionizing radiation, cisplatin, doxorubicin and taxol, administrated alone or in combination for the treatment of p53wt and p53−/− cells were evaluated.
Materials and Methods
Cell culture. Established human cell lines of different tumor entities, namely near triploid bronchial carcinoma cell line A549 presenting wild-type TP53 gene (p53wt), near triploid pharyngeal squamous cell carcinoma cell line FaDu presenting mutated TP53 gene and near hexaploid NSCLC cell line H1299 with TP53-null gene (p53−/−) from the German Collection of Microorganisms and Cell Cultures (Braunschweig, Germany) were used in this study. Cells were cultured in Dulbecco's modified Eagle's medium routinely supplemented with 10% heat-inactivated fetal calf serum (Gibco, Lyon, France) and incubated at 37°C in a humidified atmosphere with 5% CO2 and media replacement every two days.
Effects of irradiation on proliferation of certain cancer cells1.
Cell treatment. The cells were placed in culture medium (2×105 cells/ml) one day before exposure to doxorubicin (100 nM), cisplatin (10 μM), taxol (100 nM) or radiation. Test compounds were purchased from Sigma (Hannover, Germany). Because the stock solutions (×1000) of the test compounds were prepared in dimethylsulfoxide (DMSO; Sigma), the control samples were also made up in 14 mM (0.1%) DMSO. For combined management, cells were treated first with cisplatin (10 μM), doxorubicin (100 nM), or 14 mM (0.1%) DMSO, used as control. Taxol was added to the cell cultures 3 h later. Irradiation (2 Gy) was administrated 24 h after the treatment with taxol.
Radiation source. Radiation exposure of the cell cultures (106 cells/ml, 15 ml per flask) in doses of 0 (sham-treated control cells), 1, 2, 4, 6, 8 and 16 Gy was carried out by means of an X-ray system (YXLON Int. X-Ray GmbH, Germany): 200 kV, 20 mA, 0.5 mm Cu yielding a dose rate of 1.2 Gy per min. Dosimetry was performed with a clinical dosimeter UNIDOS equipped with a Semifles Ionization Chamber (PTW-Freiburg, Germany).
Flow cytometry. After appropriate treatment, cells were fixed and stained with PI (Sigma) and analyzed by flow cytometry (CyFlow; Partec, Münster, Germany) as previously described (14). The fractions of dead cells with sub-G1 DNA content, as well as the fractions of cells in G0+1, S and G2+M phases of the cell cycle, were quantified using the level of measured fluorescence, using the CyFlow software (Partec).
Statistics. The experimental results are expressed as the mean±standard deviation (mean±s.d.) of six independent experiments. Analysis of variance (ANOVA) was applied to assess differences between subgroups; p<0.05 was considered significant.
Results
Radiation effects in p53wt and p53−/− cells. Alterations in the cell cycle distribution were studied by flow cytometry 6, 12, 18 and 24 h after exposure to radiation with 0 (sham-treated control), 1, 2, 6, 8 and 16 Gy. No perturbations of the cell cycle were registered in the A549, FaDu and H1299 sham-treated control cell cultures during the time of investigation (Table I). Differences in the behaviors of p53wt and p53−/− cell lines were evident from 12 h after irradiation (Figure 1). While p53wt A549 cells showed a G1 block, with a strong decrease of the proportion of cells in S phase, in p53−/− FaDu and H1299 cells, a G1 block was not apparent. The percentage of cells in the G0+1 phase was dose-dependently reduced in FaDu and H1299 cells. At the same time, a prominent radiation block in the G2+M phase was found in A549, FaDu and H1299 cell lines except at the lowest dose (1 Gy). The percentage of cells in G2+M phase increased in a dose- dependent manner in A549, FaDu and H1299 cell lines.
Cell cycle effect of tested compounds. Different changes in the cell cycle distribution were registered 24 h after administration of the tested compounds (Table II, Figure 2). Cisplatin (10 μM) caused delay in the S phase, accompanied by decreasing percentage of G0+1 cells, increasing proportion of G2+M and dead cells in A549, FaDu and H1299 cell lines, respectively. Doxorubicin (100 nM) provoked reduction of S cell proportion with an increased proportion of cells in G2+M phase in p53wt A549 cells. A decrease of G0+1 cell proportion in p53−/− FaDu and H1299 cells was accompanied by a remarkable block at the G2+M phase. These changes were accompanied by an increased proportion of dead A549, FaDu and H1299 cells. Taxol (100 nM) induced accumulation of A549, FaDu and H1299 cells by arrest at the G2+M phase, accompanied by a reduction of the proportion of the cells in G0+1 and S phases and an increased proportion of dead cells correspondingly.
Combined effect of radiation and certain chemicals1.
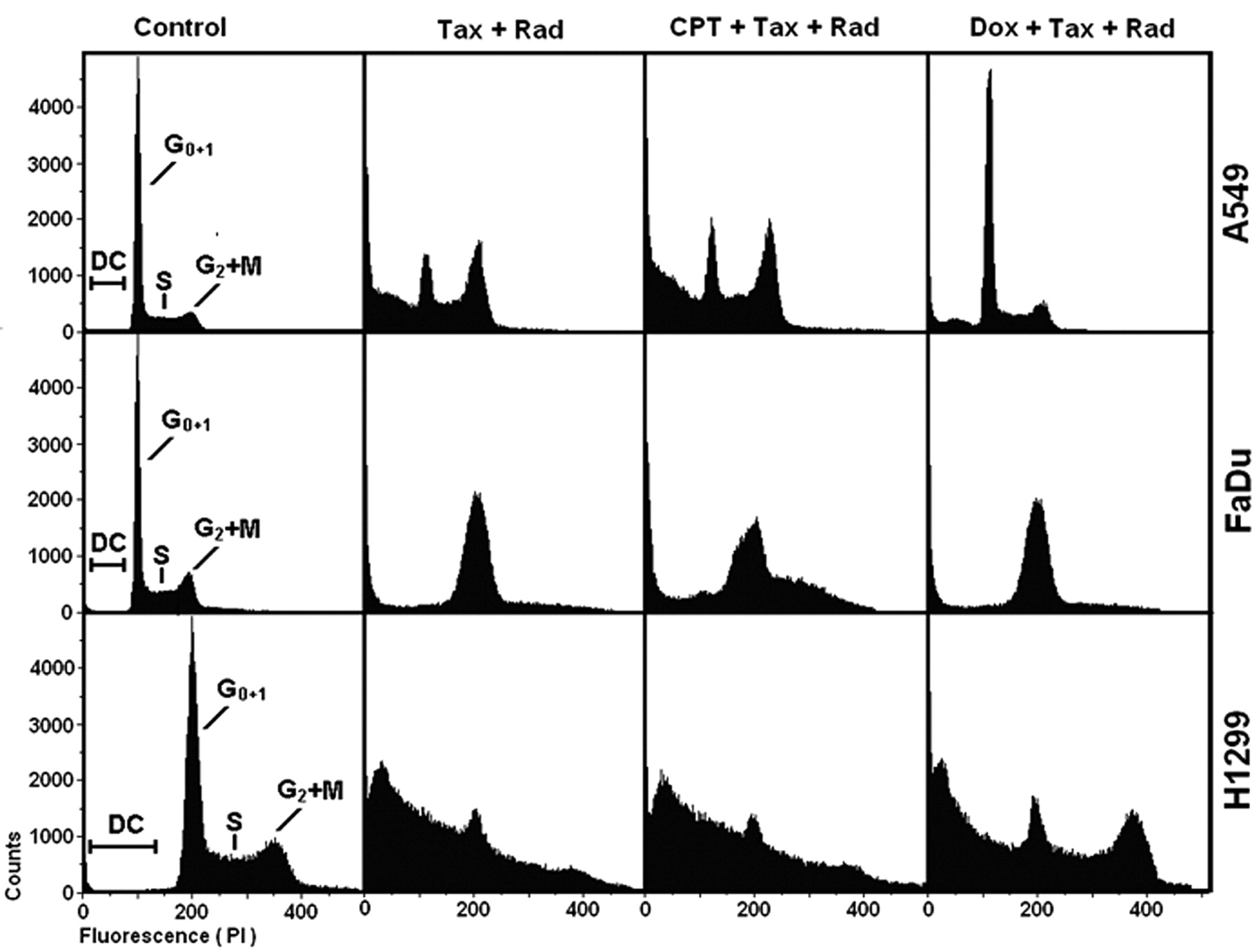
Protective effect of the test compounds from the taxol/radiation treatment. Alterations in cell cycle distribution of 105 cells were investigated by flow cytometry at 24 h after the end of the treatment (Table II, Figure 3). Administration of the combined taxol/radiation treatment resulted in an increased proportion of dead cells in A549, FaDu and H1299 cell lines. While cisplatin did not show any protective effects, pre-treatment with doxorubicin protected p53wt A549 cells, but not FaDu and H1299 cells, from the effects of combined taxol/radiation treatment, reducing the proportion of cells in G2+M phase and dead cells, and increasing the proportion of cells in the G0+1 phase.
Discussion
This study investigated the basic principles of how to selectively kill p53-deficient FaDu and H1299 cells by combined treatment using ionizing radiation and taxol and to protect p53wt A549 cells by using prior administration of the cytostatic compounds doxorubicin or cisplatin. We paid particular attention to the varied cellular responses to ionizing radiation, cisplatin, doxorubicin and taxol administrated alone and in combination. Cell cycle perturbations and apoptosis after the action of radiation in NSCLC cell lines exhibiting either wild-type p53 or lacking p53 expression have been evaluated. This study confirmed earlier findings that ionizing radiation induces different types of cell cycle arrest in p53wt and p53−/− cell lines (14). While p53wt A549 cells expressed a G1 block with a strong decrease of cells in the S phase of the cell cycle, in p53−/− FaDu and H1299 cells, a G1 block was not apparent (as measured 24 h after the treatment, Figure 1). At the same time according to the data obtained, ionizing radiation with 2 Gy itself, induces a rather weak effect on the cell cycle in both A549 and H1299 cell lines if compared with control cells (as measured 24 h after the treatment, Table I). Cisplatin, by forming cytotoxic adducts with DNA dinucleotides and inducing intrastrand crosslinks, has been shown to induce p53-dependent G1/S block, p53 independent delay in S phase transition, and G2/M block (15). The anthracycline antibiotic doxorubicin has been reported to cause a reversible cell cycle arrest at the G1 and G2 phases mainly due to its ability to intercalate into DNA and break the strands of the double helix by inhibiting topoisomerase II (11). Following binding to β-tubulin, the microtubule-targeted tubulin-polymerizing agent taxol causes mitotic arrest and apoptosis in a variety of cancer cells. Such blocked cells were arrested during the next several days of culture and eventually perished (10). Taxol is one of the most successful drugs for the treatment of NSCLC. It is highly active and frequently used for adjuvant therapy after resection of localized disease and in combination with radiation for locally advanced disease and treatment of patients with advanced disease. It was previously reported that taxol – radiation interactions for inoperable locally advanced NSCLC yielded remarkable local tumor responses and durable in-field tumor control using schedule-dependent low-dose taxol for radiosensitization (5). It was shown here that taxol increased the proportion of apoptotic cells after radiotherapy in A549, FaDu and H1299 cell lines independently of their p53 status (Table II). Application of the antagonistic drugs presents unique opportunities for p53-dependent modulation of the cell cycle of the proliferating p53wt cells of the intact surrounding tissues to protect them from the taxol during chemotherapy of p53−/− tumors. It was found that preliminary administration of doxorubicin induced growth arrest and protected A549 cells from the taxol/radiation treatment while simultaneously killing FaDu and H1299 cells (Figure 3).

Dose dependence. Dose dependence of cell cycle distribution. Fractions of dead A549 (p53wt), FaDu (p53−/−) and H1299 (p53−/−) cells (DC) as well as the proportions of cells in G0+1, S, and G2+M phases of the cell cycle 12 hours after exposure to radiation with 0 (sham-irradiated control), 1, 2, 4, 6, 8 and 16 Gy are presented. Significant differences are noted by asterisks (*, p<0.05).
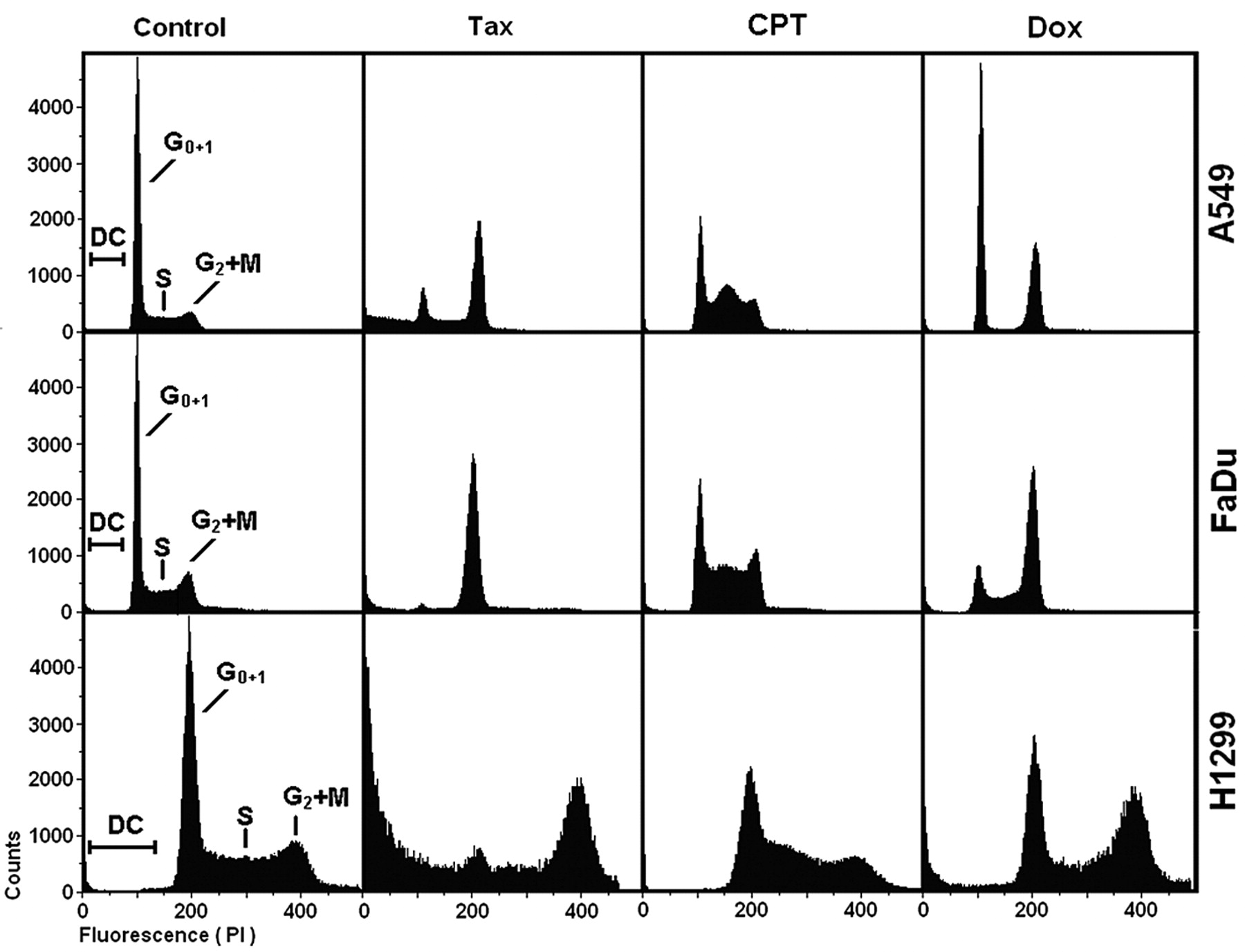
Cell cycle effects of irradiation and tested compounds. Cell cycle distribution of A549 (p53wt), FaDu (p53−/−) and H1299 (p53−/−) cells 24 h after administration of taxol (Tax, 100 nM), cisplatin (CPT, 10 μM), doxorubicin (Dox, 100 nM) or DMSO (14 mM, Control). The positions of dead cells (DC) as well as the cells in G0+1, S, and G2+M phases of the cell cycle are indicated.
{kind=link}
{kind=link}
{kind=link}
Protective effect of tested compounds. Cell cycle distribution of A549 (p53wt), FaDu (p53−/−) and H1299 (p53−/−) 24 h after the end of combined treatment. Cells were treated with cisplatin (CPT, 10 μM), doxorubicin (Dox, 100 nM) or DMSO (14 mM, Control). Taxol (Tax, 100 nM) was added to the cell cultures 3 h later. Radiation exposure (Rad, 2Gy) was administrated 24 h after the treatment with taxol. The positions of dead cells (DC) as well as the cells in G0+1, S, and G2+M phases of the cell cycle are indicated.
Conclusion
These data provide a cellular basis for the synergistic actions of radiation and chemotherapy and may be useful for further clinical investigation of combined therapy for lung cancer. However, the level of protection achieved may differ depending on the disease and treatment protocols. In further studies, combined therapy should be tested in established human tumor xenografts.
Footnotes
-
Grant Support
This research and the authors were supported by the Federal Ministry of Education and Research, Germany, BMBF Contract 03ZIK042.
- Received February 3, 2012.
- Revision received March 9, 2012.
- Accepted March 12, 2012.
- Copyright© 2012 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved