

Abstract
Background: Nonhepatic cancer risk of cirrhotic patients seems to be increased. Major surgery and chemotherapy in cirrhosis are associated with increased mortality and morbidity, which limits treatment. Aim: The aims of this study were analysis of (a) prevalence, (b) outcome after treatment, (c) of survival rate and (d) predictors of survival in a cirrhotic population. Patients and Methods: The study population was assembled retrospectively from a database of hospitalized patients (n=354). The Kaplan-Meier method was used to calculate the survival rate, and Cox regression analysis was performed to identify prognostic parameters. Results: Altogether, 84 neoplasms in 70 patients were observed. A total of 54 were nonhepatic (15.3%) mainly colorectal carcinoma, prostate cancer and tobacco-related neoplasms. TNM stage was the best prognostic parameter (p<0.0001). Low bilirubin (p=0.01), normal albumin (p=0.005) and absence of ascites (p<0.0001) were also related significantly to longer survival. The rate of postinterventional death after specific treatment was high. A proportion of patients received no specific therapy due to reduced physical performance, even in cases of limited disease. Conclusion: Our data confirm the increased risk of cirrhotic patients for developing nonhepatic cancer. Advanced TNM stage was associated with reduced long-term survival. Scoring systems, such as Child's classification and Model of Elevated Liver Disease (MELD) score, were suitable parameters to predict mortality. Oncological management in patients with cirrhosis must be on an individual basis, independent from TNM classification.
- Child's classification
- hepatocellular carcinoma
- liver cirrhosis
- MELD-score
- nonhepatic cancer
- survival probability
- TNM classification
It is well recognized that liver cirrhosis (LC) from any cause predisposes to hepatocellular carcinoma (HCC), but nonhepatic malignancies also seem to occur more frequently and at an earlier age in patients with cirrhosis than in the general population (1, 2). Previous studies in Denmark, Italy and France demonstrated an increased prevalence of gastric, breast and testicular cancer and of all types of cancer associated with tobacco and alcohol abuse (cancer of the lung, larynx, buccal cavity, pharynx, pancreas, urinary bladder, and kidney) in patients with LC (3-5). Furthermore, LC is an independent risk factor for the development of adenomatous colorectal polyps (6). Significant liver dysfunction is a challenging problem in patients undergoing major surgical procedures related to the severity of the pre-existing liver disease. In recent studies assessing clinical outcomes, in patients with cirrhosis undergoing cardiac surgery, postoperative morbidity and mortality rates have been reported to be increased (7, 8). Furthermore, patients with cirrhosis are known to have a high complication and mortality rate of up to 20% after major abdominal operations (9, 10). Previous reports have shown that the higher mortality was not attributable to impaired cardiac function, but to an increased susceptibility to infections, gastrointestinal complications, and bleeding (11, 12). Apart from surgery, the administration of chemotherapy also represents a major problem in LC with simultaneous cancer due to its hepatotoxic side effects which may cause acute liver failure (13). Systematic investigations of the complication rate and long-term results of specific oncological treatment of nonhepatic tumor disease in LC are sparse (14-16)
Therefore, the aims of the present study were (i) to evaluate the prevalence of nonhepatic malignancies (compared with the published estimates of the average population using global cancer statistics for different entities of cancer); (ii) to study the risk of postinterventional complications after specific treatment including oncological surgery, (radio)chemotherapy and ablative techniques such as chemoembolization; (iii) to analyze the survival rate for nonhepatic malignancies in a large series of patients with cirrhosis in a tertiary referral center in Southern-Germany; and (iv) to evaluate the predictors of long-term survival including age, etiology of cirrhosis, Model of Endstage Liver Disease (MELD) score and Child's classification of liver disease.
Patients and Methods
Study population. The study population was assembled retrospectively from a database of hospitalized patients (n=354) of our hospital who had the diagnosis of LC as defined by discharge diagnosis codes (ICD K74.6) during the 4-year period from January 2005 until May 2008. The majority of patients came from the surrounding area of our hospital and were mainly of German origin. Seventy of these patients also suffered from cancer (hepatic and nonhepatic malignancies). LC was established either by histology or by clinical, laboratory, and radiographic findings demonstrating impaired hepatic function and portal hypertension. The entire etiologic spectrum of LC was included. Child-Pugh (CP) classification score was calculated for each patient (CP A, ≤7 points; CP B, 8-10 points; CP C, >11 points). The patient charts were analysed retrospectively with special regard to the type of cancer, tumor staging according to the tumor, node, metastasis (TNM) classification, details of performed specific treatment including oncological surgery, radiochemotherapy and ablative techniques such as radiofrequency ablation, and information about compliance and present alcohol consumption. The complete specific oncological treatment was performed exclusively in the Gastroenterological, Oncological, Radiological and Surgical Departments of our hospital. Preoperative data included age, gender, date of surgery, tumor location, type of resection, date of last follow-up, and the date and cause of death. Postoperative death was defined as a fatal outcome that occurred during the same hospitalization or up to 30 days after surgery. The endpoints were patients' overall survival and the risk of postoperative death. Patients with multiple hospitalizations were counted only once, and their earliest hospitalization was chosen as the index hospitalization. The follow-up period for cancer occurrence began at the date of discharge from the hospital and ended at the date of death. However, since our study was performed retrospectively, the diagnosis of cirrhosis and tumor staging was not verified by autopsy. Since most patients were admitted several times, 624 admissions to our hospital were analyzed. The study has been approved by the appropriate Ethical Committee. Additionally, the prevalence of nonhepatic cancer in our cirrhotic population was compared with the published estimates of the average population using global cancer statistics of 2008 for different entities of cancer [GLOBOCAN series of the international Agency for Research on Cancer (17)].
Clinical characteristics of all patients with liver cirrhosis (n=354) without (n=284) and with synchronous occurrence of cancer (n=84).
Statistical analysis. Statistical analysis was performed using PASW Statistics 17.0 (SPSS Inc., Chicago, IL. USA). Data about specific oncological treatment, postoperative death and long-term survival were analysed with descriptive statistics. For comparisons between the long-term and the short-time survival groups, the Mann-Whitney-U test or, when appropriate, the two-sample t-test was used. To evaluate the dependence of survival on categorical prognostic factors, the Chi-square or the Fisher's exact test was calculated. Besides univariate analysis of potential prognostic predictors of longer survival, an additional multivariate analysis was performed using logistic regression. To evaluate the diagnostic capability of the MELD-scores in differentiation between long- and short-term survival, a receiver operating characteristic (ROC) curve analysis was used. The area under the ROC curve was used to evaluate the overall diagnostic performance of the MELD-scores. The survival analysis was also performed with the Kaplan-Meier estimator. All statistical analyses were made using a two sided 0.05 level of significance.
Number of all malignancies in the cirrhotic population according to cancer site.
Results
Retrospective analysis of all hospitalized patients with liver cirrhosis with and without simultaneous cancer. The clinical characteristics of all patients with cirrhosis [n=354, 158 men, 196 women (non-cancer group: n=284; 109 men, 175 women; cancer group: n=70; 49 men, 21 women)] with and without simultaneous (nonhepatic-, hepatic-) cancer are represented in Table I. Median age was 65.5 yr [range 41-93 years (non-cancer group: 65.2 years; cancer group: 66.8 years.)]. A total of 84 neoplasms were observed in 70 patients of our cirrhotic population [19.8% (70/354)]. Fifty-four were nonhepatic (15.3%), while 30 were hepatic malignancies [hepatocellular carcinoma 7.6% (27/354), cholangiocellular carcinoma 0.8% (3/354)]. In 59 patients (84.2%), one single cancer site was diagnosed, while 11 (15.7%) had two and 1 (1.4%) had three independent malignancies at the same time, respectively (Figure 1, Table II). The etiology of LC was alcohol abuse in 59.6% (non-cancer group: 61.3%, cancer group: 52.9%), cryptogenic in 15.5% (non-cancer group: 14.1%, cancer group: 21.4%), hepatitis B in 3.1% (non-cancer group: 3.5%, cancer group: 1.4%), hepatitis C in 15.3% (non-cancer group: 14.1%, cancer group: 20%) and other specific causes in 6.5% (non-cancer group: 7%, cancer group: 4.3%). On the basis of CP-classification, 40.7% (non-cancer group: 39.4%, cancer group: 45.7%) of patients had stage A cirrhosis, 24.9% (non-cancer group: 21.5%, cancer group: 38.6%) had stage B, and 34.5% (non-cancer group: 39.1%, cancer group: 15.7%) had stage C, respectively. To rule out potential risk factors for cancer occurrence other than LC, information was obtained concerning persistant alcohol abuse and smoking: 51.7% of all patients (non-cancer group: 56.7%, cancer group: 31.4%) reported persistant alcohol abuse, while 53.4% (non-cancer group: 55.6%, cancer group: 44.3%) reported persistant nicotine abuse. For easier comparison of the different cancer sites in our population of patients with simultaneous cancer (n=70), we divided all of the patients into three subgroups: (I) patients with nonhepatic malignancies and a survival time more than 12 months [n=26, ‘long-term survival-group’: mean survival time: 77.3 months (24-168 months)]; (II) patients with nonhepatic malignancies and a survival shorter than 12 months [n=28, ‘short-term survival-group’: mean survival time: 4.2 months (0.1-12 months)]; and (III) patients suffering from primary liver cancer [hepatocellular carcinoma, cholangiocellular carcinoma; n=30, mean survival time: 6.6 months (0.2-24 months)]. On the basis of MELD-score, the average score was 5.8 in group I, 14.5 in group II and 14 in group III, respectively. The follow-up period for cancer occurrence began at the date of cancer diagnosis and ended at the date of death, which was defined as endpoint of this study. Three patients of subgroups I (n=1) and II (n=2) were also suffering from hepatocellular carcinoma which was diagnosed in each case later than the nonhepatic malignant tumor. Since it was the aim of our study to evaluate the prevalence of nonhepatic cancer, the risk of postoperative death and predictors of long-term survival after specific treatment of cirrhotic patients with simultaneous extrahepatic malignancies, only subgroup I and II were of special interest. A large proportion of patients suffering from hepatocellular carcinoma and cholangiocellular carcinoma in our study group (n=14) did not receive special oncological therapy due to extensive cancer disease, advanced age or noncompliance (data not shown). Additionally, patients who received specific treatment, such as operation (n=3), ablative procedures (chemoembolization, n=10) or chemotherapy (n=3) nevertheless had a low survival time (Table III).

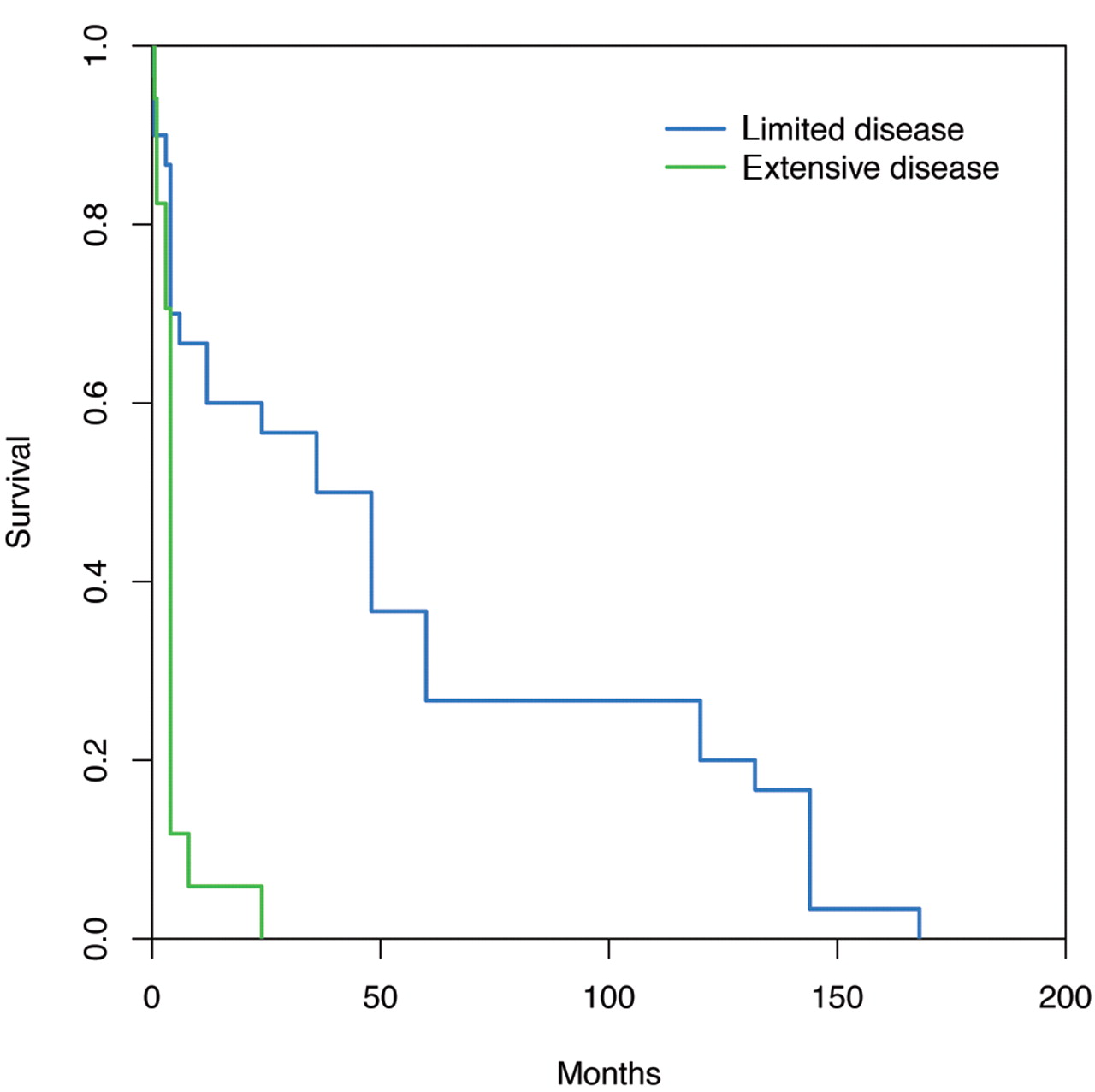
Influence of an extensive disease stage (green line: extensive disease, blue line: limited disease) on the survival probability (cumulative survival, y-axis) which is related significantly to survival time (x-axis, months); univariate analysis: p<0.0001; multivariate analysis: p=0.001.

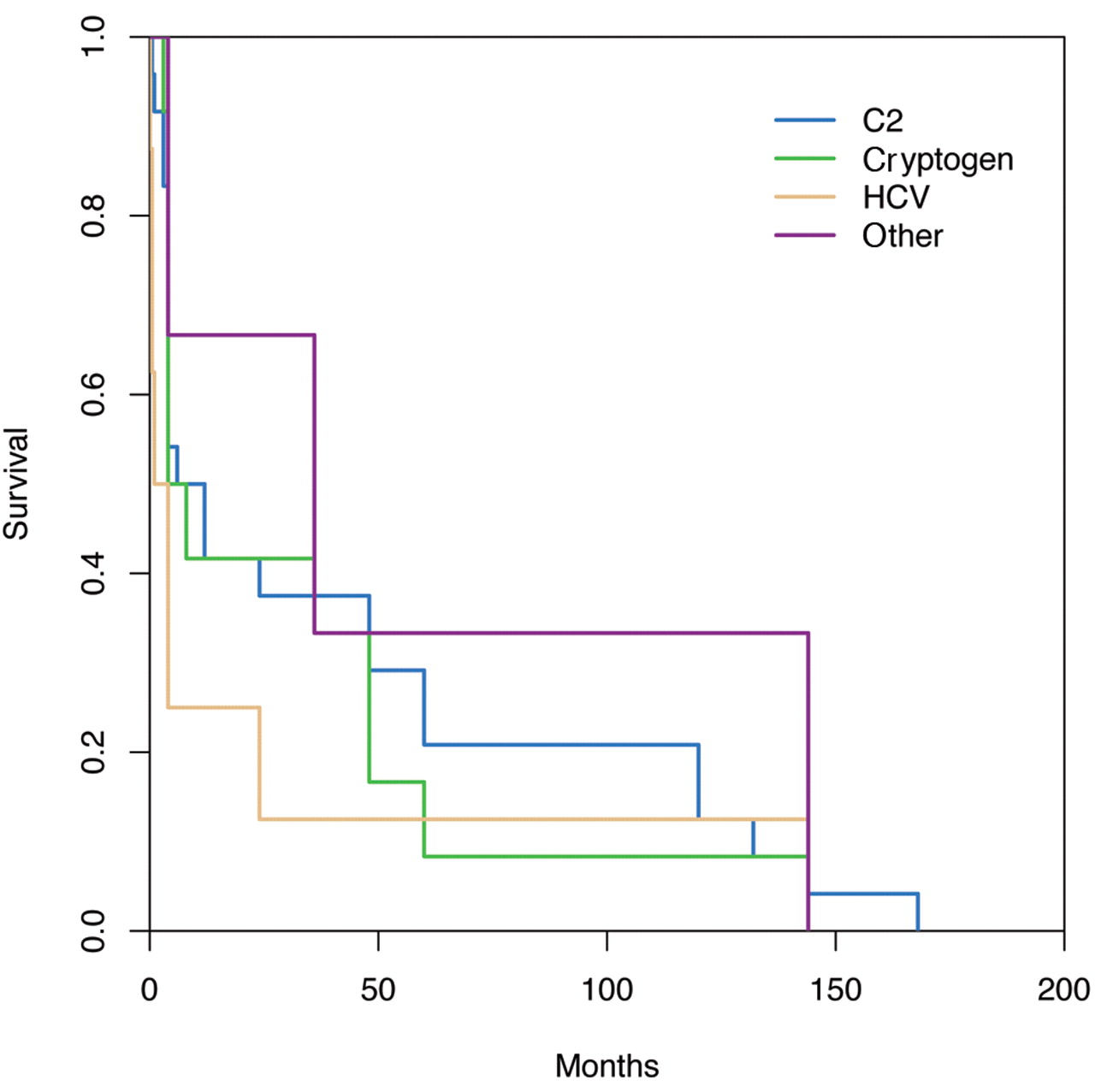
Influence of etiology of LC on the survival probability, demonstrating no significant differences concerning survival time (months); p=0.709 (etiology of cirrhosis: blue line, alcohol abuse; green line, cryptogene; yellow line, HCV, purple line: other).
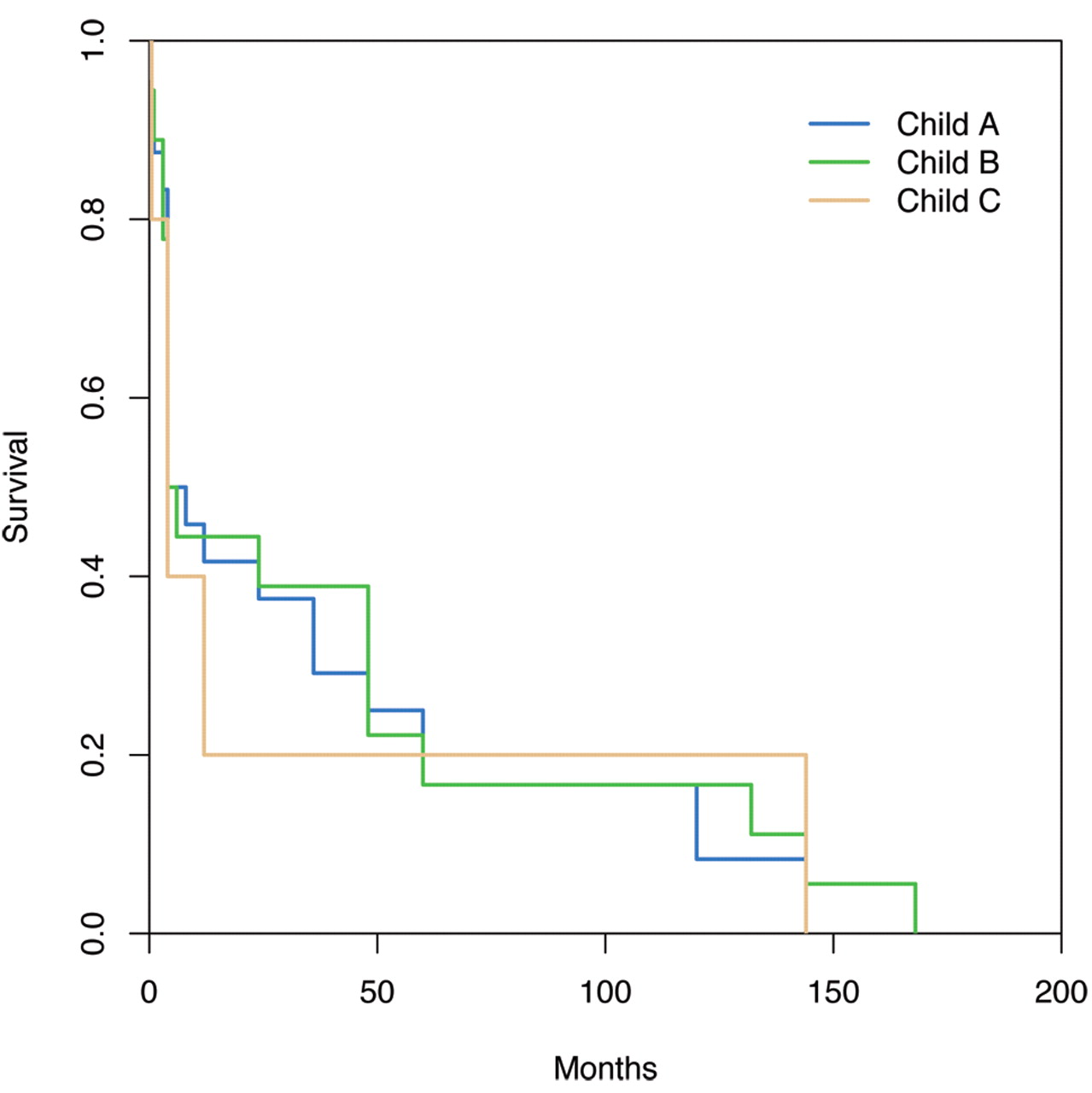
Influence of Child's classification (blue line: Child A, green line: Child B, brown line: Child C) on the survival probability, demonstrating no significant differences concerning survival time (months); p=0.762.
Prevalence of neoplasms and cancer site. The number of all malignant neoplasms in our cirrhotic population is shown in Figure 1. When analyzing the different cancer sites of the 54 nonhepatic malignancies, we found a relatively large proportion of tobacco-related tumors such as lung cancer. Colorectal carcinoma (CRC, n=9) was the most frequent nonhepatic malignant tumor followed by lung (n=6) and prostate cancer (n=6). The exact number of all malignancies in the cirrhotic population according to cancer site is shown in Table II. The rate of intrahepatic metastasis in nonhepatic cancer was very low in our study population (n=2, 3.7%).
Specific treatment in cirrhotic patients with cirrhosis and nonhepatic cancer. As shown in Table III, all patients with long-term survival recieved specific oncological treatment including surgery, chemotherapy, and radiation, alone or in combination. On contrary, a large proportion of patients with short-time survival (n=13) did not recieve specific therapy, only palliative treatment due to reduced physical performance (n=7) and noncompliance (n=6) even in cases of limited disease on the basis of TNM classification. The reason for noncompliance was mostly due to chronic alcohol abuse. The rate of postinterventional death after specific treatment within 30 days of the procedure was relatively high (n=8) and occurred mainly in patients with advanced chronic liver disease (Child's classification B or C; n=5) and after surgical therapy (n=5). Reasons for postinterventional death were as follows: sepsis (n=4), incurable bleeding (n=2) and liver failure (n=2).
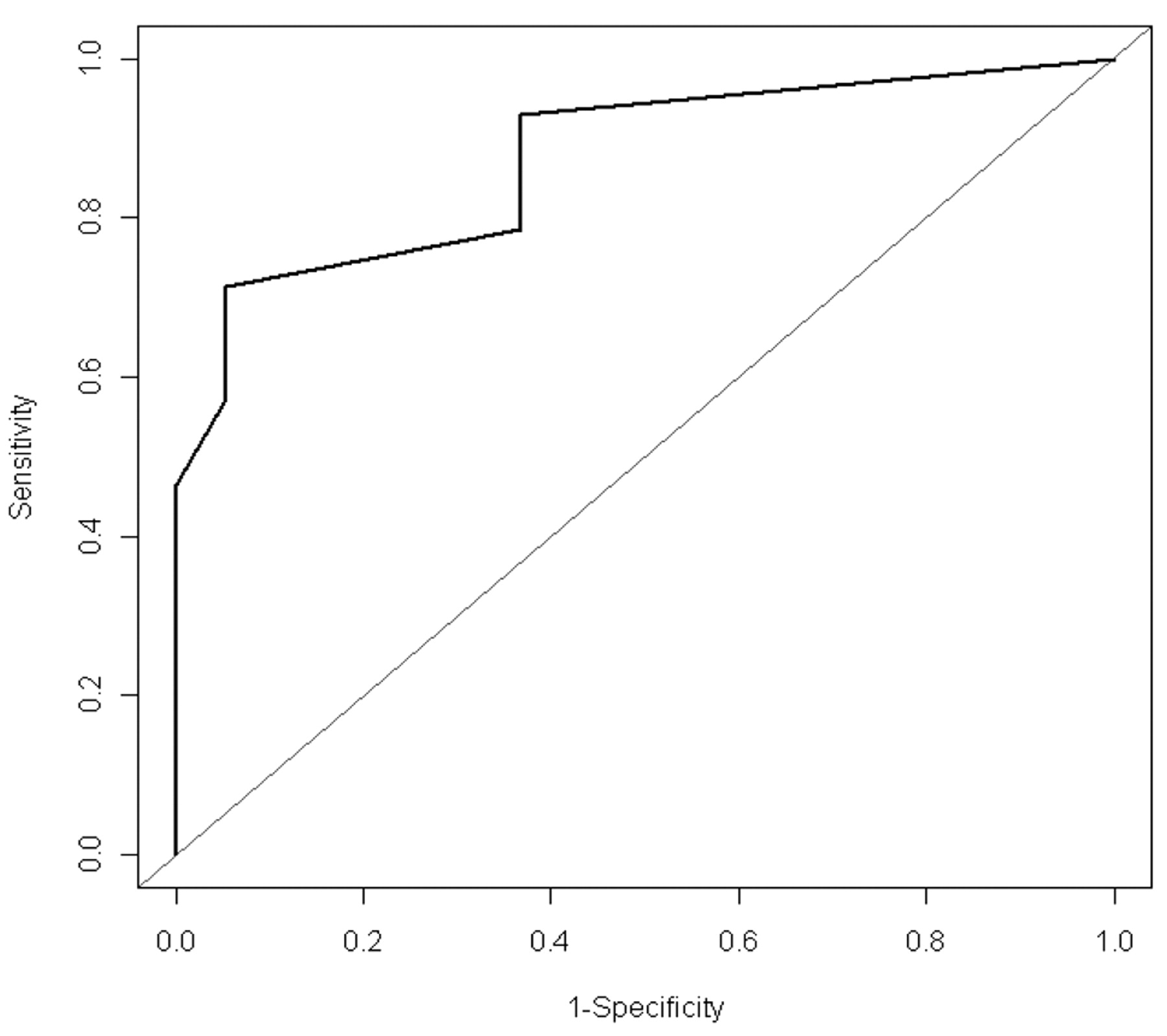
Analysis of potential prognostic predictors of outcome concerning longer survival. In univariate analysis, the mean age of subgroup I (‘long-term survival group’) was significantly lower (60.53 years; p=0.032; t-test) compared to subgroup II (‘short-term survival group’, 68.25 years). Serum bilirubin (p=0.01) and albumin (p=0.005) before intervention were significantly different between the two subgroups while international normalized ratio (INR) was not significantly different (p=0.455; Mann-Whitney-U test). Furthermore, the occurrence of ascites before the beginning of specific treatment was also significantly related to a shorter survival time (p <0.0001) while the presence of portal hypertension had no influence on survival (p=0.159; Fisher's exact test). As expected, the rate of extensive disease was significantly higher in subgroup II compared to subgroup I (p<0.0001, Figure 2). We found no significant differences for gender (p=1.000), etiology of LC [Figure 2 (p=0.709)] and Child's classification of liver disease [Figure 3 (p=0.762)] by using Fisher's exact test. However, when using multivariate analysis, only bilirubin level (p=0.014, Figure 4) and extensive disease (p=0.001) had a significant influence on the probability of short-term survival. Cox regression analysis revealed no significant influence of bilirubin (p=0.292) or INR (p=0.991) on survival time. The diagnostic capability of the MELD-scores in differentiation between long and short survival using a receiver operating characteristic (ROC) curve analysis was good (AUC =0.873, Figure 5).
Characteristics of oncological treatment of the 70 patients with liver cirrhosis and synchronous occurrence of cancer (altogether 84 neoplasms, since some patients suffered from more than one neoplasm).
Discussion
Cancer risk in patients with cirrhosis seems to be modified by factors such as changes in hormonal levels, impaired metabolism of carcinogens, or alteration of immunological status resulting in a higher prevalence of nonhepatic malignancies compared to the normal population. However, previous studies analyzing the outcome of cirrhotics undergoing major cardiac or abdominal surgery have demonstrated increased postoperative morbidity and mortality rates, while chemotherapy is often contraindicated due to side-effects. Therefore, the treatment of nonhepatic cancer including conservative and surgical therapy might be highly problematic in these patients. To examine the prevalence of extrahepatic cancer in LC in Germany, the risk of postinterventional complications and long-term survival, after specific oncological treatment, we conducted a retrospective analysis of a large population of patients with cirrhosis who were admitted to our hospital. Furthermore, we also evaluated potential predictors of long-term survival, when nonhepatic cancer was diagnosed including age, gender, etiology of cirrhosis, MELD score and Child's classification of liver disease.

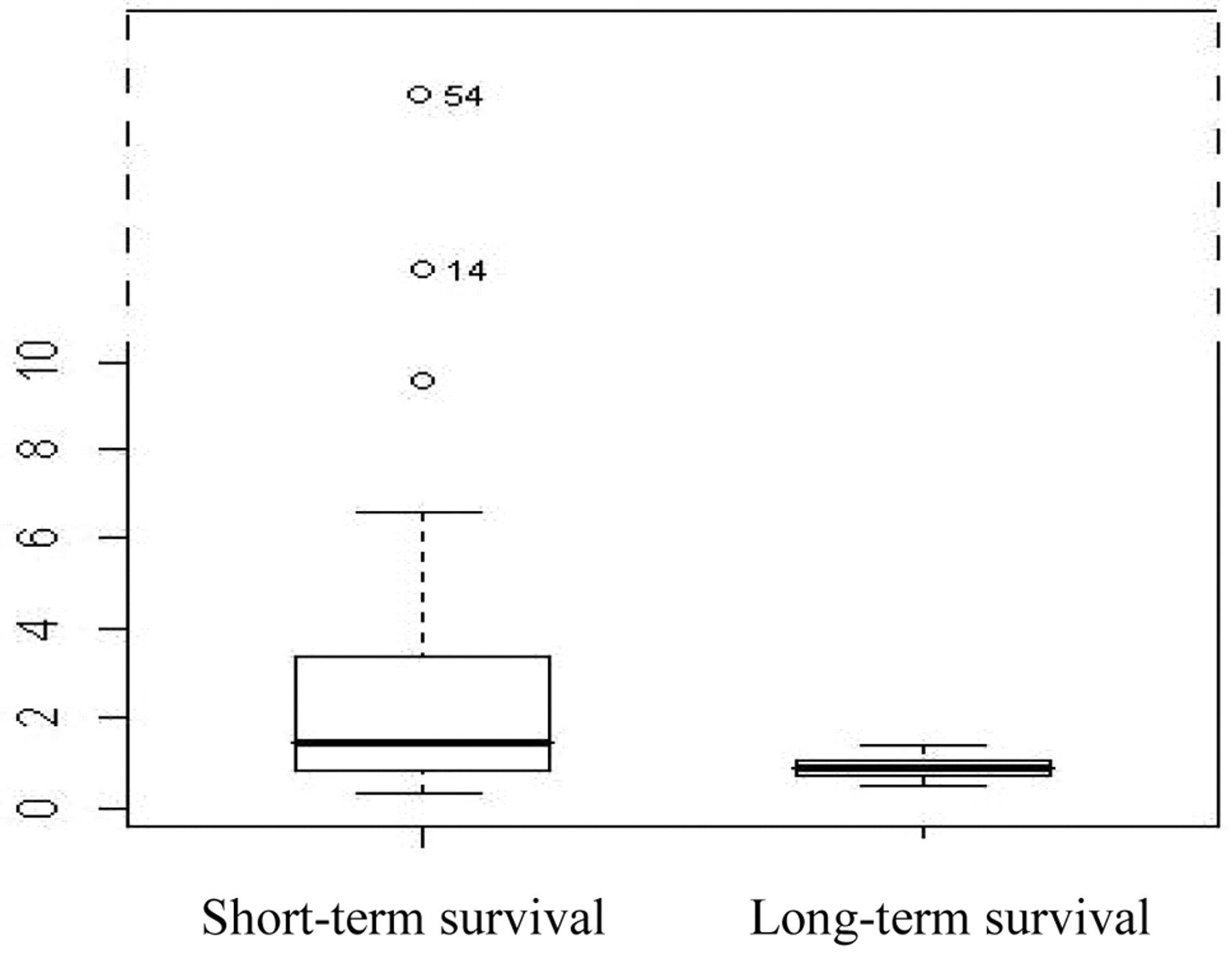
Influence of an increased bilirubin serum level (mg/dl, y-axis) on the survival probability which is related significantly with survival time; univariate analysis: p=0.01; multivariate analysis: p=0.014 [short-term survival=follow up shorter than 12 months; long-term survival=follow up longer than 12 months. Only two bilirubin-values of our population were above 10 mg/dl (14 mg/dl and 54 mg/dl). These values were plotted in a non true-to-scale representation].
Prevalence of neoplasms and cancer site. Whether LC is a risk factor for cancer at sites other than the liver has not been well investigated, except for patients with primary biliary cirrhosis and autoimmune hepatitis (18-21). In 15.3% of all cirrhotic patients in our study population, nonhepatic cancer was diagnosed, while 19.8% developed a neoplasm, when all cases of primary liver cancer were included. We did not find any major difference concerning age, severity and etiology of LC when comparing the cirrhotic non-cancer group with the cirrhotic cancer group, apart from a slightly increased proportion of hepatitis C in patients with simultaneous cancer (20% vs. 14.1%). Furthermore, on the basis of CP-classification, we found a higher proportion of cirrhotics with stage C disease in the non-cancer group compared with those from the cancer group (39.1% vs. 15.7%). The prevalence of heavy alcohol intake and nicotine abuse was remarkably high in our study population (51.7% and 53.4%, respectively). Interestingly, the rate of persistant alcohol abuse and smoking was higher in the non-cancer group (alcohol abuse: non-cancer group: 56.7%, cancer group: 31.4%; nicotine abuse: non-cancer group: 55.6%, cancer group: 44.3%). Therefore, alcohol intake and smoking, which represent major risk factors for carcinogenesis, do not explain the increased cancer prevalence in our study population alone. Similar to the average population, the most frequent nonhepatic malignant tumors in our cirrhotic population were prostate cancer (n=6), CRC [n=9 (men: 7, female: 2)] and lung cancer [n=6 (men: 5, female: 1]. Compared to the average population using global cancer statistics of 2008 (GLOBOCAN series), the prevalence of these cancer sites was higher in our LC population [CRC: 0.45% (worldwide average population) vs. 2.3% (9/354); lung cancer: 0.22% (worldwide average population) vs. 1.7% (6/354); prostate cancer: 0.38% (worldwide average population) vs. 1.7% (6/354)] (17). Additionally, 15.7% (n=11) of patients were suffering from cancer in more than one site. Although part of this increase in cancer risk may be attributable to alcohol and tobacco consumption, our study opens up the possibility that cirrhosis plays a role in the carcinogenesis of types of cancer other than liver cancer. Changes in the metabolism of carcinogens or hormones could affect cancer risk. It is known that LC induces changes in estrogen metabolism, and male patients with cirrhosis have increased endogenous estrogen levels, which may lead to gynecomastia and testicular atrophy (22). Previous studies in female cirrhotics indicate that LC is associated with menstrual irregularity, increased frequency of spontaneous abortion, and early menopause (23). Moreover, the liver plays a central role in the metabolism of lipid- and water-soluble drugs and other chemicals, and patients with cirrhosis have also been reported to experience alterations in immune functions and risk of infections (24). Furthermore, the increased cancer risk in cirrhotic patients might be caused by chronic alcohol consumption which is known to be associated with an increased prevalence of certain cancer sites, such as rectal cancer and adenomatous polyps of the colon (6, 25). Interestingly, the rate of intrahepatic metastasis due to nonhepatic cancer was very low in our study population (Table I). This might be due to our spectrum of malignancies, which includes several types of cancer which do not metastasize into the liver (kidney and thyroid). A potential pathophysiological reason might be the disturbed intrahepatic architecture (including microcirculation) due to cirrhosis which aggravates invasion of tumor cells and metastasis. Furthermore, the phenomenon of infrequent liver metastases has been described before (14). When analyzing the benefit of specific oncological treatment, we found that a large proportion of patients recieved only palliative treatment, even in cases of limited cancer, due to reduced physical performance and noncompliance resulting in a short survival time. Therefore, specific oncological treatment should always be an individual decision in patients with cirrhosis, independent of the usual cornerstones of cancer management as the expected prognosis and the TNM stage. The rate of postinterventional death within 30 days of specific treatment was relatively low and occurred mainly in patients with advanced chronic liver disease (Child's classification B or C, high MELD score).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
ROC curve analysis of MELD-scores for discrimination between long and short survival revealing an AUC of 0.873.
Analysis of potential prognostic predictors of outcome concerning longer survival. However, when cancer is diagnosed, many oncologists and surgeons are afraid of poor outcomes after specific treatment. Previous studies evaluating the postoperative complications and the predictors of long-term survival found a strong trend that the Child's classification, and not the TNM stage of the carcinoma, predicts the risk of postoperative mortality which means that patients with decompensated LC (Child's classes B and C) should not undergo major operations (14-16). Most of our patients with cirrhosis and with nonhepatic cancer (subgroup I and II) belonged to Child's class A (51%), while 38.2% belonged to class B and 10.6% to class C, respectively. Surprisingly, we found no significant difference between the two groups for Child's classification (p=0.762). This might be due to the large variety of cancer entities and the resulting broad spectrum of different treatment options of the study population. This clearly represents the major limitation of our study, apart from the relatively small size of our study population and the restricted geographic area where our patients came from. However, before the beginning of oncological treatment, we found a significant, favourable influence of low bilirubin (univariate analysis: p=0.01; multivariate analysis: p=0.014), normal albumin and the occurrence of ascites (p=0.0001) on the survival rate. Therefore, downstaging Child B and C patients is a useful attempt to improve the outcome of subsequent elective oncological therapy including surgery and chemotherapy. For easier comparison of the different cancer sites in our study population, we divided all nonhepatic malignancies into either limited or extensive disease on the basis of TNM classification. Extensive disease was defined when metastases were diagnosed. When comparing cirrhotics with long-term survival and short-term survival after oncological therapy we found a significant difference concerning tumor spread when the diagnosis of cancer was made. Our data demonstrated that the TNM stage of the carcinoma was the best prognostic indicator of long-term survival when using univariate (p<0.0001) and multivariate analysis (p=0.001). Furthermore, the diagnostic capability of the MELD-score in differentiation between long and short survival using a ROC curve analysis was good (area under the curve, AUC=0.873). Further prognostic information was provided by comparing the mean age of both subgroups which was significantly lower in the ‘long-term survival group’ (60.53 years; p=0.032; t-test) than in the ‘short-term survival group’ (68.25 years). Additionally, we found a slightly larger proportion of highly malignant cancer sites such as cancer of the pancreas or esophagus, in patients with a shorter survival time which might have contributed to the worse outcome of this subgroup but this was not statistically significant. In conclusion, our data confirmed that patients with cirrhosis have an increased risk of developing nonhepatic cancer, especially CRC, prostate cancer and cancer related to tobacco abuse. A definite reason for this phenomenon can not be derived from the present study, since we did not find any clear differences between the cirrhotic non-cancer and the cirrhotic cancer group concerning age, severity and etiology of LC, while the proportions of common risk factors such as alcohol abuse and smoking, were even higher in cirrhotic patients without cancer. Therefore, the responsible hepatologist should bear in mind this additional complication of patients 2ith cirrhosis, which represents an often underestimated problem compared with typical complications of cirrhosis such as hepatocellular carcinoma, bleeding esophageal varices or ascites. Patients with compensated cirrhosis (low MELD score; low serum bilirubin, normal albumin, no ascites) had a higher survival rate and a lower perioperative mortality. Since mean bilirubin levels were lower, while albumin levels were higher in subgroup I compared to subgroup II, low serum bilirubin and normal albumin might be useful prognostic factors for the further course. Similarly to patients without liver disease, an older age and a extended TNM stage are associated with reduced long-term survival. The rate of therapeutical nihilism was very high in our study population due to noncompliance and reduced physical condition which represents frequent problems in cirrhotic individuals due to chronic alcoholic disease. This emphasizes the importance of individually-based decision management, especially for patients with LC, independently of TNM classification. Since oncological therapy, including surgery and chemotherapy, was performed exclusively at our hospital, this study represents a single-center experience which should be confirmed by further prospective studies.
Footnotes
-
Conflict of Interest
None.
- Received March 15, 2011.
- Revision received May 20, 2011.
- Accepted May 23, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved