

Abstract
In patients with breast cancer (BC), axillary lymph node sampling (ALNS) is a reliable procedure with low morbidity, alternative or complementary to sentinel lymph node biopsy (SLNB), which may improve the detection rate of axillary node metastases as compared to SLNB alone in staging the axilla. The aim of this study was to assess the usefulness of ALNS in conjunction with SLNB in improving the sensitivity of SLNB alone at frozen section examination. One hundred and twelve women (median age 56 years, range 29-71 years) with BC underwent SLNB using a combined radioisotope and isosulfan blue dye technique. Two groups of age- and tumor size-matched patients were prospectively randomized: Group A (SLNB alone, 55 women) and group B (SLNB plus ALNS, 57 women). Intraoperative examination showed SN involvement in 32 (28.6%) patients: group A=14 (25.5%), group B=18 (31.6%), whilst the final pathology showed axillary node involvement in 7 further cases (group A=5, group B=2). The sensitivity and accuracy were 73.7% vs. 90.0% (p=0.23) and 90.9% vs. 94.7% (p=0.49), group A vs. B, respectively. Multivariate analysis showed that age >65 years and body mass index independently correlated with the amount of axillary drainage in both groups, which was 47.5±11.3 and 49.6±12.2 ml (A vs. B, p=NS), respectively. In conclusion, in our preliminary study, ALNS in conjunction with SLNB is a low-risk procedure, useful to reduce the false-negative rate of SLNB and to improve the accuracy of intraoperative evaluation of the axillary nodes in patients with BC.
- Breast cancer
- sentinel node
- sentinel node biopsy
- axillary node sampling
- axillary lymphadenectomy
- axillary clearing
Breast cancer (BC) remains a major public health problem in developed countries and, despite recent advances, the management of BC remains difficult, especially in patients with axillary lymph node metastases (1). Axillary dissection still represents the most accurate means of determining axillary node status, but at the expense of significant morbidity, both physical and psychological, such as pain, lymphedema, numbness, loss of strength, as well as in terms of worsening of own body image (2, 3).
In recent years, new advances in exploring the axilla for the determination of axillary node involvement have been suggested. Since the sentinel lymph node should represent the first area to receive lymph flow and thus usually the first to harbor a metastasis from BC, sentinel lymph node biopsy (SLNB) has been proposed as an alternative to standard AN clearing (4). The high accuracy of SLNB and concerns regarding morbidity after standard axillary node dissection have translated into widespread use of this technique, especially in the management of patients with early BC (5, 6). Several studies have shown that the sensitivity of SLNB examination ranges between 85% and 98% for the detection of axillary node metastases using standard histology (7, 8). Axillary lymph node sampling (ALNS), is a reliable alternative procedure in staging the axilla with low-morbidity, widely practiced, especially in the United Kingdom, and which may improve the detection rate of axillary node metastases by 10-15% as compared to SLNB alone (9, 10).
The aim of this study was to assess the usefulness of ALNS in conjunction with SLNB in improving the sensitivity of SLNB alone at frozen section examination.
Patients and Methods
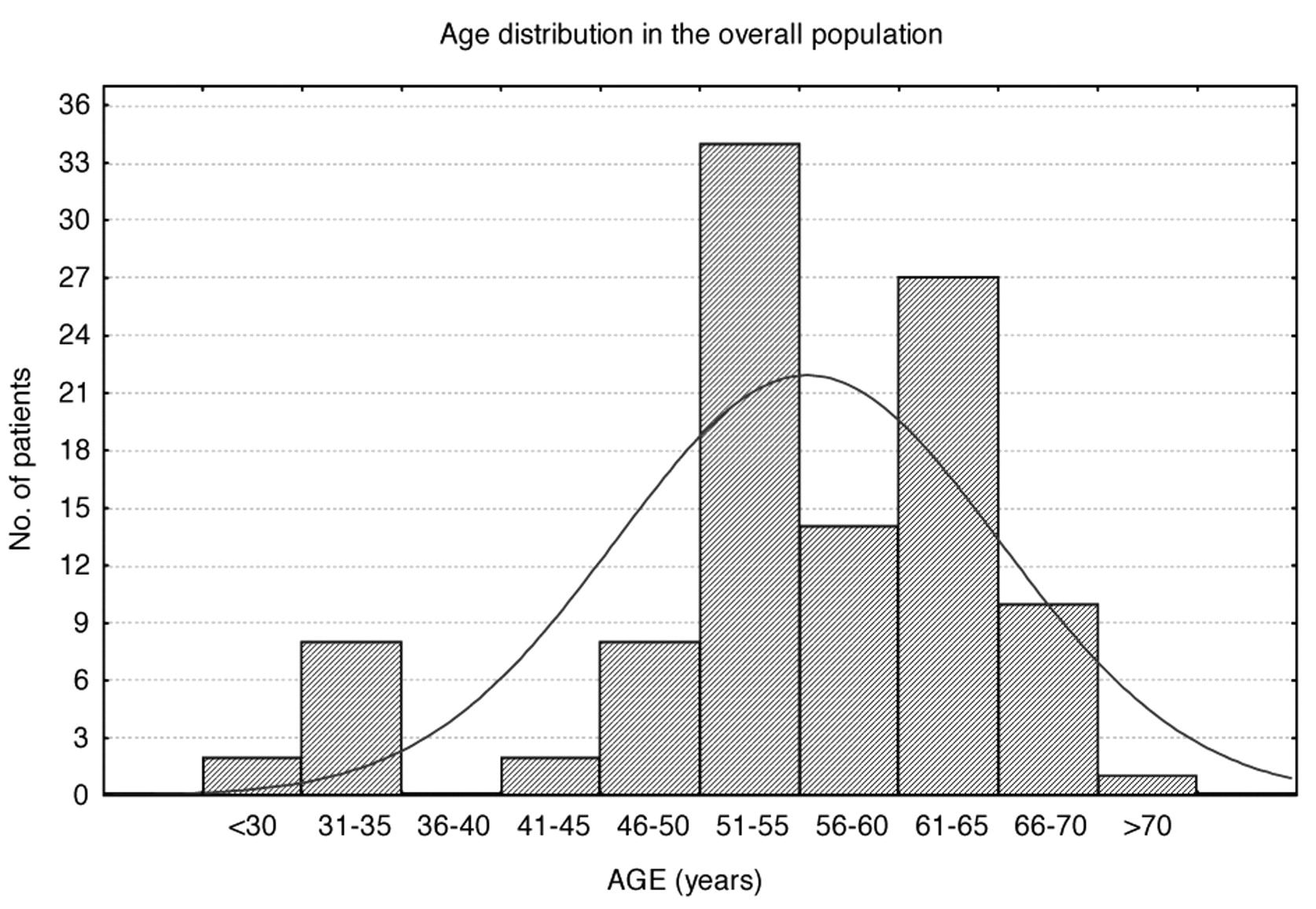
Study design. One hundred and twelve consecutive women (median age 56 years, range 29-71 years) with core-biopsy or fine-needle aspiration biopsy (FNAB)-proven pT1-2 BC, undergoing curative surgery, were enrolled in the study (Figure 1). For all patients, a combined radioisotope (99mTc-sulfur colloid) and isosulfan blue dye technique was used and the SLNB was guided by both the appearance of blue dye in the nodes and the gamma probe, according to the American Society of Clinical Oncology (ASCO) guideline (5). Written informed consent was obtained from all the participants and the study had full ethical approval by the Institutional Review Boards.
The following parameters were recorded: age of the patients (years), body mass index (BMI), preoperative serum levels of tumor markers carcinoembryonic antigen (CEA) and cancer antigen 15-3 (CA 15-3), side and size (maximum diameter measured by the pathologist) of the tumor, histological type (infiltrating ductal vs. other types) and nuclear grade, estrogen-receptor (ER) positivity (>20%), axillary node status (N0 vs. N1), number of nodes removed, total amount of axillary drainage.
Two groups of age- and tumor size-matched patients were prospectively randomized by lottery into group A (SLNB alone, 55 women) and group B (SLNB plus ALNS, 57 women). All patients with metastatic sentinel nodes at intraoperative histology underwent axillary node dissection at levels I and II .
Histology and immunohistochemistry. The removed axillary nodes were bisected and two frozen sections were obtained (hematoxylin-eosin stain, 40 μm between levels) using standard laboratory procedures (11). At a later date, three additional sections (4-6 μm-thick) were cut from each face of the paraffin-embedded node slab for permanent histology (12). The immunohistochemical assay was performed on 4 μm sections cut from the blocks and immunohistochemistry for ER carried out (13-15). The histological grade was defined according to the modified Bloom-Richardson classification (16).
Measurement of serum tumor markers. CEA and CA 15-3 serum levels were determined by automated testing using a two-site enzyme-linked immunosorbent assay (ADVIA Centaur XP Immunoassay System, Siemens, München, Germany) according to the manufacturer's instructions. A cut-off limit of 10 ng/ml (CEA) and 30 U/ml (CA 15-3) was used, as previously reported (1, 17).
Axillary drain. At the end of the surgical procedure, both in patients who underwent ALNS and in those who underwent SLNS plus ALNS, two 14-F Redivac drains were inserted, into the chest wall and the axilla, respectively. The total amount of axillary drainage was measured daily by the nursing staff. Criteria suggesting the removal of the axillary drain were a reduction of more than 50% in respect of the day before, and 15 ml or less per 24 hours, as previously reported (18).
Statistical analysis. Comparisons between the parameters of the two groups of patients were performed by unpaired Student t-test for normally distributed data (i.e. age, BMI, CEA, CA 15-3 serum levels, tumor size, total amount of drainage), while proportions (i.e. side and histological type of the tumor, ER positivity, AN status) were analyzed by chi-square (χ2) test, or the Fisher exact probably test when one or more frequencies were less than 5. The Mann-Whitney U-test was used for the comparison of qualitative variables in case of a non-normal distribution (i.e. nuclear grading). The Pearson's correlation coefficient (R) was also calculated. A two-sided error level of p<0.01 was considered statistically significant. Variables significantly associated with increased amount of axillary drainage in univariate analysis were entered into a multivariate analysis. Sensitivity was defined as: true-positives (TP)/(TP + false-negatives), specificity as: true-negatives/(true-negatives + false negatives) and accuracy as: (TP + true-negatives)/overall patients.
Results
Overall, as expected, there was a relationship (R=0.31, p<0.01) between size of the tumor and baseline CA 15-3 serum levels, independent of age (Figure 2). No further significant correlations were found.
Table I reports the main characteristics in each group and the relative p-value, showing that there were no significant differences between groups among each parameter considered, except the number of removed ANs. In particular, the total amount of axillary drainage did not differ, suggesting that both techniques achieved the same low-morbidity result. Univariate and multivariate analysis showed that age >65 years and BMI independently correlated with the amount of axillary drainage in both groups, which was 47.5±11.3 and 49.6±12.2 ml (A vs. B, p=NS), respectively.
Intraoperative frozen section examination showed sentinel node involvement in 32 out of 112 (28.6%) patients: group A=14 (25.5%), group B=18 (31.6%), whilst the final pathology showed axillary node involvement in 7 further cases (Group A=5, Group B=2). Thus, the overall positive axillary node rate was 34.8%. No false-positive results were found and the specificity was 100%. As reported in Table II, the sensitivity and accuracy were (group A vs. B) 73.7% vs. 90.0% (p=0.235) and 90.9% vs. 94.7% (p=0.806), respectively.
Discussion
Tumor size and AN status have long been considered the most reliable prognostic factors in predicting survival of patients with BC, leading to correct adjuvant treatment (19, 20). However, over 90% of women with tumors smaller than 1 cm have no axillary node involvement, and thus axillary clearing would not be useful in the majority of the cases (3, 21, 22).
The sentinel node is defined as a lymph node on a direct drainage pathway from a primary tumor (23), and SLNB was firstly described by Cabanas in patients with penile carcinoma in 1977 (24). The technique was extensively applied to patients with stage I melanoma and then extended to the BC population as a less invasive and highly accurate procedure alternative to AN dissection in staging of the axilla (25-27). The major concern with SLNB is the existence of false-negative (FN) cases and the sentinel node identification rate, which may lead to understaging (28). A recent meta-analysis showed that using lymphatic mapping and SLNB, the average FN and sentinel node identification rates were 7.3% and 96%, respectively (29). It has been suggested that FN results could be related to: (i) tumor cells that occasionally pass through to non-sentinel axillary nodes, while tracers used to identify SN remain in the first node on the direct drainage pathway; (ii) the existence of different lymphatic pathways from a primary tumor; or (iii) the presence of heavy tumor infiltration causing lymphatic flow blockage (30, 31).
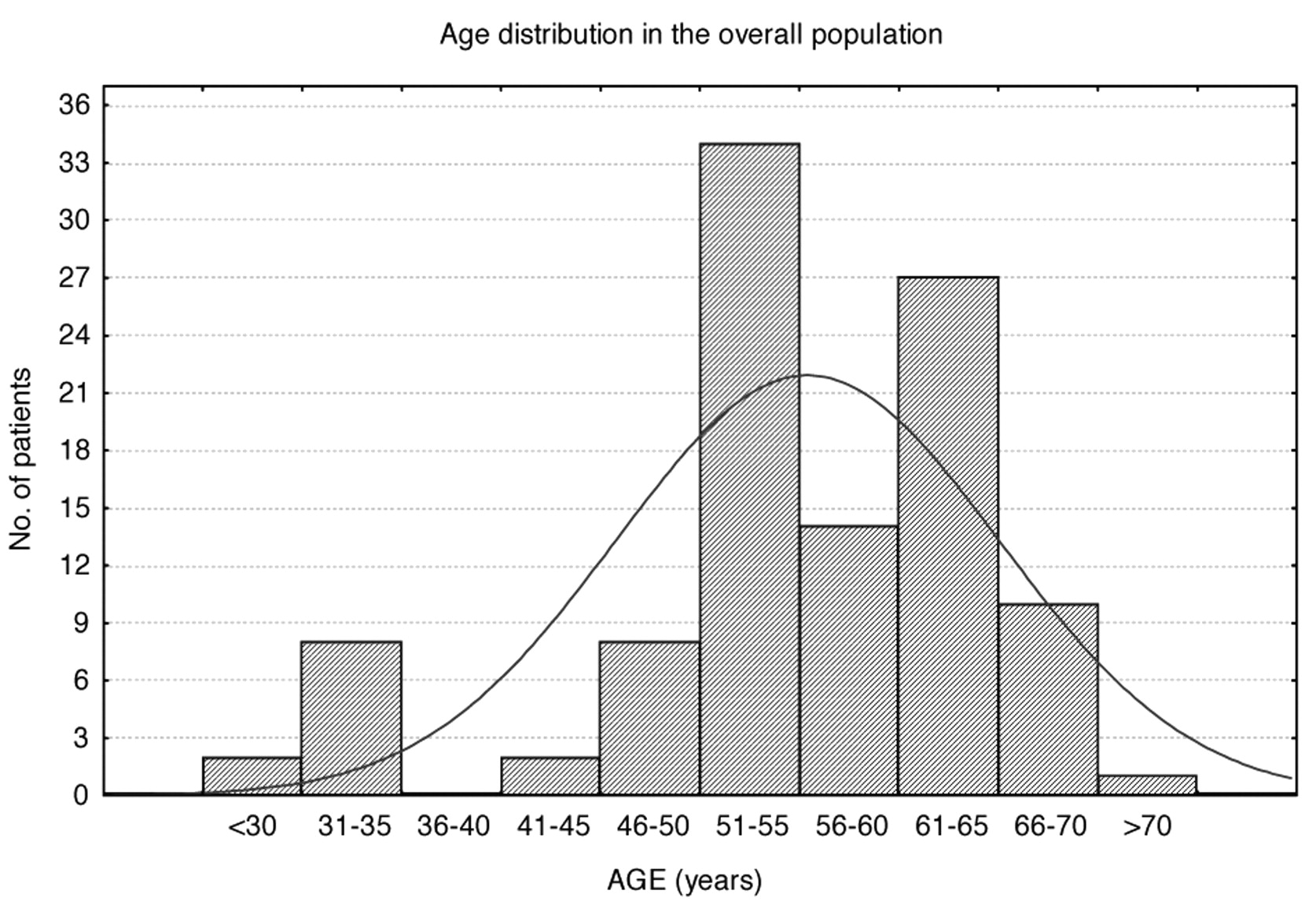
Age distribution of the patients.
In patients with small tumors, SLNB can be supplemented by ALNS; the usefulness of ALNS and blue dye SLNB in combination have been reported in several studies (9, 28, 32, 33). Axillary sampling procedure seems to be as accurate as axillary node dissection, with no difference in the axillary recurrence rate between women staged by the two methods. Thus, five- or three-node sampling is useful to predict the status of nonsentinel nodes and to avoid axillary node dissection in patients without sentinel node metastases (34, 35). Although ALNS alone reduces but does not completely eliminate FN of SLNB, its accuracy may reach 95-98%, with an equivalent long-term survival compared to axillary node dissection (2, 36).
Hoar and Stonelake reported a 14.3% FN rate for SLNB alone, whilst that for SLNB plus ALNS was reduced to 3.6% (37). They conclude that SLNB is inaccurate and ALNS is recommended. Goyal et al. found that the FN rate in patients with grade 3 tumors was 9.6% compared with 4.7% in those with grade 2 tumors (p=0.022), and that the FN rate in patients who had one sentinel node harvested was 10.1%, compared with 1.1% in those who had multiple (three or more) sentinel nodes removed (38). We did not find similar correlations, but the sensitivity of SLNB plus ANS was higher than that of SLNB alone (90.9% vs. 73.7%, p=NS).

{kind=link}
{kind=link}
Baseline serum levels of carcinoembryonic antigen (CEA, ng/ml) and cancer antigen 15-3 (CA 15-3, U/ml) in the overall population as related to age.
Main characteristics of the patients (N=112) and p-value between groups (Student's t-test, χ2 test*; Mann-Whitney U-test**).
Several studies report the usefulness of preoperative axillary ultrasonography, fine-needle aspiration cytology and other imaging techniques, such as 99mTc-sestamibi scintimammography (SSM) and 18F-fluoro-2-deoxyglucose (FDG)-positron-emission tomography/computed tomography (PET/CT) in the preoperative staging of the axilla (39-42). In a previous study, we found 90.7% accuracy for SSM and ultrasonography together, with 100% specificity when ultrasound-guided fine-needle aspiration cytology was used, suggesting that in some patients SLNB can be avoided and axillary node dissection should be the primary procedure (43). Diagnostic performance of PET/CT does not seem to be superior to that of ultrasonography and contrast-enhanced CT (44).
Results of intraoperative vs. permanent histology in groups A and B, and p-value between groups (Fisher exact probably test).
In conclusion, in our preliminary study, ALNS in conjunction with SLNB is a low-risk procedure useful to reduce the FN rate of SLNB and to improve the accuracy of intraoperative evaluation of the axillary nodes in patients with BC.
Footnotes
-
* Presented in part at the 59th Annual Cancer Symposium of the Society of Surgical Oncology (SSO), San Diego, CA (USA), March 23-26, 2006.
- Received December 6, 2010.
- Revision received January 25, 2011.
- Accepted January 25, 2011.
- Copyright© 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved