

Abstract
Background: The prognostic values of the International Prognostic Index (IPI) and the Follicular Lymphoma International Prognostic Index (FLIPI) have widely been demonstrated in diffuse large B-cell lymphoma and follicular lymphoma. No attempts to assess their applicability in MALT lymphoma have been made so far. Patients and Methods: A total of 143 patients with MALT-lymphoma were analysed. Parameters of both IPI and FLIPI were retrospectively assessed and correlated with relapse and time to relapse as markers of clinical course. Results: According to IPI, 96 patients (67%) were classified as low, 22 (15%) low-intermediate, 17 (12%) high-intermediate and 8 (6%) as high risk. FLIPI identified 99 patients (70%) at low risk, 35 (24%) at intermediate and 9 (6%) at high risk. After a median follow-up time of 39.5 months, 123 patients were alive and 46 patients had relapsed (median time to relapse 27 months). IPI significantly correlated with time to relapse, with the typical differentiation into low, low-intermediate and high risk groups. FLIPI divided patients into three groups, but the low and intermediate risk groups showed a similar clinical course. In terms of additional progonostic factors, univariate analysis suggested autoimmune disease and multifcoal disease as correlated with relapse. Multiple regression analysis, however, identified only extragastric disease as predictive of relapse (p=0.001). Conclusion: Our data demonstrate that both IPI and FLIPI are able to discriminate prognostic subgroups in patients with MALT-lymphoma. However, the low and intermediate group of the FLIPI did not appear to prognostically differ.
- MALT lymphoma
- IPI
- FLIPI
- prognostic index
Mucosa-associated lymphoid tissue (MALT) lymphoma is among the more common types of lymphoma and accounts for 7% of all newly diagnosed lymphomas (1). MALT lymphoma arises in the stomach in a high percentage of patients (2), but it can affect organs throughout the whole body, including the intestinum, lung, salivary glands, thyroid and liver (3). The course of the disease is usually characterized by minor growth for a prolonged period of time, the potential for late dissemination and frequent relapses (3-5). Numerous treatment options have been proposed for patients with MALT lymphoma (6-8), ranging from ‘watchful waiting’ to more aggressive systemic approaches. Due to the heterogeneous course of the disease and differences between MALT lymphomas arising in different organs, there is no clear cut standard approach apart from eradication of Helicobacter pylori (HP) in localized gastric lymphoma.
In recent years, various investigators have tried to define factors predictive of the clinical course in patients with MALT lymphoma. In individuals with HP-positive gastric MALT lymphoma, restriction of the disease to mucosa and submucosa is thought to be a positive predictive factor (9), while the presence of t(11;18)(q21;21) or an underlying Sjogren's syndrome identifies the majority of non-responders to antibiotic treatment (10-12). While the presence of an underlying autoimmune disease apparently adversely influences the response of gastric MALT lymphoma to HP Eradication (13, 14), it does not appear to affect the overall outcome in patients with MALT lymphoma irrespective of origin (14). Judging from the current literature, gastric MALT lymphomas appear to run a more indolent clinical course, as extragastric MALT lymphomas have been suggested to be multifocal in a higher percentage, to have a significantly higher rate of relapses along with a significantly shorter time to relapse (15).
As opposed to aggressive lymphoma and follicular lymphoma, no prognostic index has been defined or validated for its applicability in MALT lymphoma. In diffuse large B-cell lymphoma, the International Prognostic Index (IPI) has repeatedly been demonstrated to be a valid predictor for the clinical course. While initial retrospective data from British Columbia have questioned the applicability of the IPI in patients treated with rituximab, the recently published RICOVER study has confirmed its validity in patients treated with rituximab plus chemotherapy (16). In analogy to diffuse large B cell lymphoma, the Follicular Lymphoma International Prognostic Index (FLIPI) has become a widely accepted prognostic tool in follicular lymphoma (17). None of these indices, however, has been tested in patients with MALT lymphoma. In view of this, we therefore retrospectively assessed these two prognostic indices and correlated them with relapse and time to relapse as markers of clinical course in patients with MALT lymphoma.
Patients and Methods
All patients with histologically verified MALT lymphoma referred to our institution between 1997 and 2007 were retrospectively evaluated. Only patients with histology compatible with the WHO definition of MALT lymphoma (18) were included in the analysis. All patients underwent extensive staging according to our standardized protocol (3), consisting of ophthalmological and otorhinolaryngological examination with sonography (MRI) of lacrimal and salivary glands, gastroscopy with multiple biopsies, endosonography of the upper GI-tract, colonoscopy and CT scan of thorax and abdomen.
Parameters of both IPI [age >60 years, extranodal involvement ≥2, elevated lactate dehydrogenase (LDH), performance status according to the Eastern Cooperative Oncology Group ECOG ≥2, disease stage defined according to the Ann Arbor citeria ≥3] and FLIPI (age >60 years, elevated LDH, Ann Arbor stage ≥3, nodal involvement ≥5, hemoglobin level ≤12 g/dl) were assessed in a standardized form (19) and correlated with relapse and time to relapse as markers of clinical course. Only patients in whom all parameters for calculation of both prognostic indices were available were included in the analysis. The grouping for both indices, as has repeatedly been published (19/20) was also used in our analysis, classifying patients with 0 or 1 risk factor into the low risk group, with 2 into the low intermediate, with 3 into the high intermediate and with 4 or 5 into the high risk group according to the IPI. According to FLIPI, patients were divided into a low (0-1), intermediate (2-3) and high (4-5) risk group.
In addition, we have also (re-)assessed the influence of MALT-lymphoma associated parameters on the clinical course, i.e. gastric vs. extragastric disease, multifocality, genetic changes, plasmacytic differentiation and monoclonal immunoglobulin production. Statistical analysis was carried out with SPSS 14.0. Partial correlation was assessed with the Pearson coefficient (CF); univariate analysis was performed with the chi-square test and reassessed with multiple regression analysis. Estimated time to relapse curves were calculated with the Kaplan-Meier method and tested for significant differences with the log-rank test.
Results
A total of 173 consecutive patients were evaluated for inclusion in the analysis; 30 patients had to be excluded due to incomplete parameters necessary for IPI/FLIPI characterization at the time of diagnosis. The remaining 143 patients (86 female, 57 male) with histologically verified MALT lymphoma of various origin were reassessed and were included in the analysis. In all these 143 patients, the respective parameters for both IPI and FLIPI were determined at the time of diagnosis by retrospective evaluation. The median age at diagnosis was 62 years [inter-quartile range (IQR): 48-73 years] and the median follow-up time was 39.5 months (IQR: 22-64). Treatment, however, was extremely heterogeneous in these patients, and included HP eradication for localized gastric lymphoma, radiation and various systemic treatments consisting of monotherapy with alkalyting agents and nucleoside analogues, as well as combination chemotherapies (data not shown). A total of 32 patients had received rituximab as a part of their management, while surgery did not play a major part of management, and had been performed in only 5 patients.
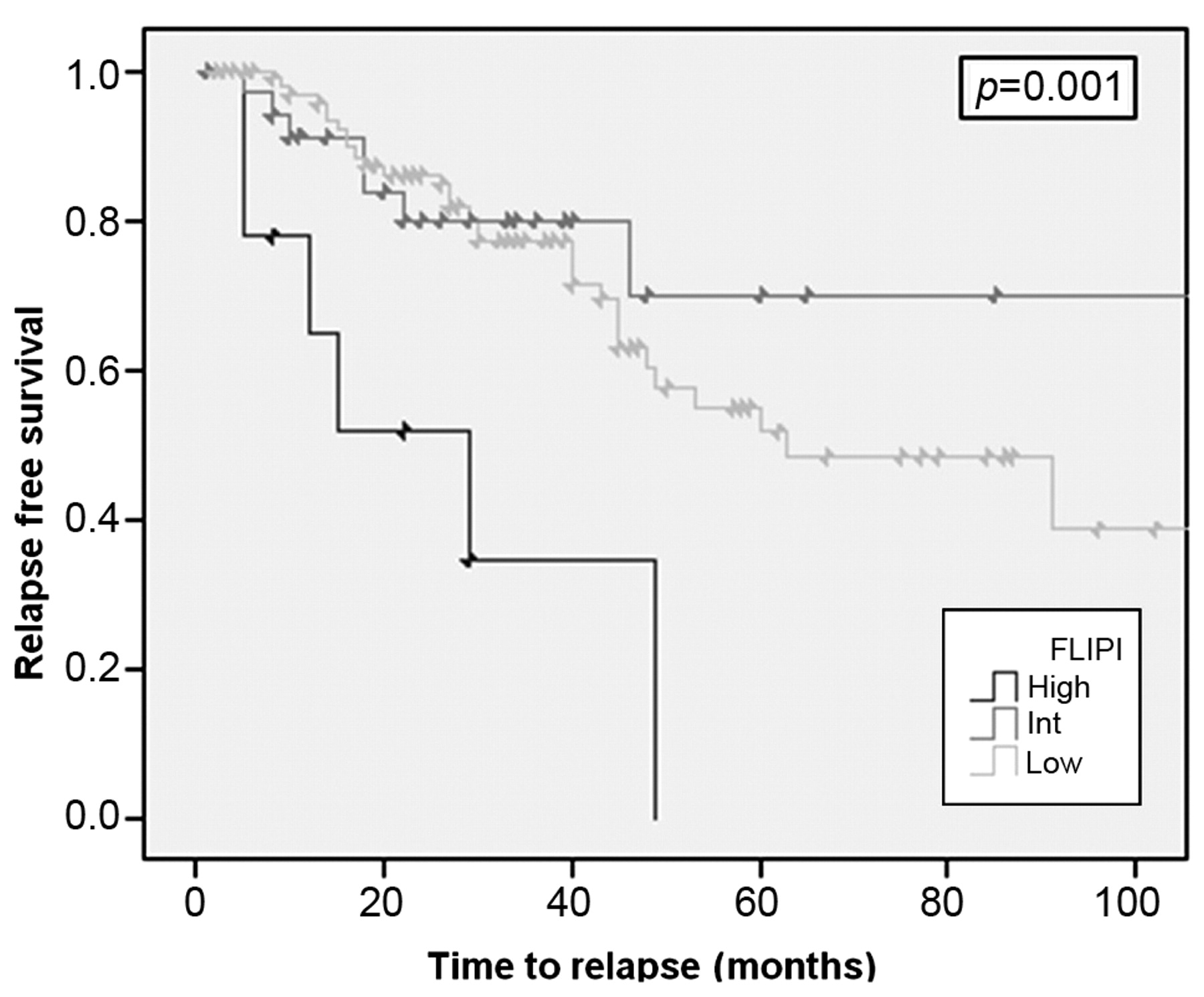
According to the IPI, 96 patients (67%) were classified into the low risk group, 22 (15%) into the low-intermediate group, 17 (12%) into the high-intermediate group and 8 (6%) into the high risk group. Application of FLIPI classified 99 patients (70%) as having low risk, 35 (24%) as having intermediate risk and 9 (6%) as having high risk. Not surprisingly, IPI and FLIPI were significantly inter-correlated (CF: 0.806, p=0.001) due to overlaping parameters, and both correlated with time to relapse (see Figures 1 and 2).
According to the IPI groups, patients in the low risk group had an estimated median time to relapse of 44 months; this was 35 months in the low-intermediate group, 28 months in the high-intermediate and 29 months in the high risk group. The FLIPI groups had an estimated median time to relapse of 42 months (low-risk), 43 months (intermediate) and 18 months in the high.-risk group. When assessed as a single group, patients with low and intermediate risk together fared significantly better than those in the high risk group (see Figure 3), although the number of patients in the latter was relatively small.
Thus, application of IPI appears to define three distinct subgroups in terms of clinical outcome, while application of FLIPI distinguishes only two subgroups, without the apparent need to distinguish between low and intermediate risk group as defined for follicular lymphoma.
When the indices are broken down into single parameters, some striking features of MALT lymphoma become apparent from our analysis. One of the parameters included in both indices, namely LDH, was only elevated at diagnosis in 3/143 patients (2%). In addition, only 11/143 patients (8%) had a performance status ≥2 according to the ECOG definition and 31/143 patients (22%) had anemia defined as a hemoglobin level ≤12 g/dl at diagnosis of MALT lymphoma. According to the Ann Arbor classification, 34 patients (24%) showed a stage ≥3. An extranodal involvement greater than 2 was very common due to the nature of this disease, however, nodal involvement ≥5 was not seen in this series.

Estimated time to relapse according to IPI.
Plasmacytic differentiation, as defined by the presence of sheets of light chain-restricted plasma cells was found in 37/128 of patients (29%), in whom this feature was assessed and production of a paraprotein (monoclonal gammopathy) was present in 37 patients (out of 94 patients available for this feature, 39%). The majority of our patients (92, 64%) suffered from extragastric disease, which was significantly correlated with the estimated time to relapse (p=0.038) on univariate analysis, while 51 patients (36%) had gastric MALT lymphoma. Disseminated/multifocal disease was detected in 45 patients (31%) and was demonstrated to be significantly correlated with relapse (p=0.047) but not with the estimated time to relapse (p=0.187). In total, 98 patients (69%) had MALT lymphoma restricted to one single organ. The number of patients suffering from an underlying autoimmune disease was 51 (36%) and correlated with relapse (p=0.018) on univariate analysis.
After a median follow-up time of 39.5 months, 128 patients are still alive at the time of writing and 46 patients have relapsed with the median time to relapse being 27 months (IQR: 14.5-47 months). Multiple regression analysis, however, identified only extragastric disease as a predictive factor for time to relapse (p=0.001), which was nevertheless significantly correlated with multifocality in our patient cohort (p=0.043). Interestingly, no other combination of parameters as assessed here was able to discriminate between distinct subgroups compared IPI/FLIPI.
Discussion
MALT lymphoma is commonly thought to run a highly indolent clinical course (5). Recently, studies have indicated that some localizations such as the ocular adnexa are best managed with a watch and wait policy (21). Apart from prognostic factors for response to HP eradication in gastric MALT lymphoma, there are currently no predictive indices to identify patients at high risk for a more aggressive clinical course who might probably benefit from early or more intensive treatment.

Estimated time to relapse according to FLIPI.

{kind=link}
{kind=link}
{kind=link}
Estimated time to relapse according to FLIPI: low plus intermediate versus high risk group.
To our knowledge, this is the first series to assess the predictive value of IPI and FLIPI in patients with MALT lymphoma. However, one of the main caveats in interpreting our series is the fact that treatment modalities were extremely heterogeneous, due to the different localizations of the disease, as well as the fact that no standard systemic approach to MALT lymphoma has been defined so far. In view of this, definition of a clinical index for MALT lymphomas will of course not alter the immediate clinical decision making, but might serve as potential parameter to be included for further definition in future prospective trials. Keeping these limitations in mind, our data nevertheless demonstrate that both IPI and FLIPI are able to predict the clinical course for a large cohort of patients with MALT lymphoma of different origin, albeit only to a certain extent. The majority of patients in this series, however, were classified into the low risk (n=96) and low-intermediate (n=22, adding up to a total of 118/143, 82%) risk groups according to the IPI, and low risk group (n=99) according to the FLIPI.
When assessing the parameters included in both indices, however, certain features of MALT lymphoma need to be kept in mind when interpreting the data. In fact, some of the parameters included in both indices apparently lack predictive significance in patients with MALT lymphoma. This is especially striking for LDH, which is rarely elevated in patients with MALT lymphoma, illustrated by the fact that only 3 out of our 143 patients had an elevated LDH. In addition, patients suffering from MALT lymphoma usually have a good PS, as also evidenced in this series with only 11 (8%) patients presenting with a PS of 2 or worse according to ECOG. In follicular lymphoma, the low number of patients initially presenting with PS status was the reason for not considering the PS as a striking marker of prognosis of these patients, as opposed to the IPI in aggressive lymphoma. Therefore, the number of patients included in this single center analysis is simply too small to identify a potential prognostic role of a poor PS upon presentation in MALT lymphoma.
Due to the, by definition, preferentially observed occurrence in extranodal sites, involvement of more than 5 lymph node regions is highly uncommon in patients with MALT lymphoma. None of our patients presented in this way, while the involvement of two or more extranodal sites is very common and apparently increases with application of a stringent staging routine (3). One of the major drawbacks in applying indices and staging systems designed for nodal lymphomas is the fact that different staging systems are sometimes used in MALT lymphoma, especially for those of gastric origin. This includes the Lugano system as well as the Paris staging system, as opposed to the classical Ann Arbor system for nodal lymphomas. In addition, it has been debated whether bilateral involvement of paired organs, the salivary or lacrimal glands, does indeed reflect disseminated disease and should thus be classified as stage I or II. According to the Ann Arbour staging system we have rated a bilateral involvement as a stage IV, as disseminated disease. This follows the rationale that such lesions are not amenable to local therapy such as radiotherapy without debilitating side-effects. This results in patients older than 60 years with a bilateral involvement of a paired organ as the parotid gland being classified into the high-intermediate risk (IPI) group, which could explain the fact that the curve for the high-intermediate risk group is virtually superimposable over that of the low risk group. This application of the classical IPI to patients with MALT lymphoma does not result in a clinically relevant subdivision into four prognostic subgroups, but rather three. A similar finding occurred with application of FLIPI, where assessment of patients with low and intermediate risk together showed a better prognosis for the overall group over that of the high risk group, but did not show a significant difference between the low and intermediate risk groups. In view of this, our data suggest that both indices are potentially able to distinguish patients with good prognosis and low risk of relapse from those in the very high risk group, but do not allow for further subdivision and fine tuning as evidenced for follicular lymphoma and aggressive lymphoma, respectively. The fact that some parameters included in both indices simply are not clinically relevant in MALT lymphoma might partly explain this finding. However, despite being a relatively large series, our number of patients is simply not large enough to allow for discrimination of very rare parameters such as LDH or PS in MALT lymphoma, which would require a huge multicenter effort.
In terms of other clinical parameters, this analysis showed that autoimmune disease, multifocal disease, stage IV, as well as extranodal involvement ≥2 were significantly correlated with relapse on univariate analysis, which is in agreement with previous studies. Surprisingly, no influence of genetic aberrations, especially t(11,18)(q21,q21), on the clinical course could be found. Multiple regression analysis, however, identified only extragastric disease as a predictive factor for time to relapse (p=0.001), which was nevertheless significantly correlated with multifocality in our patient cohort (p=0.043). From our data and various parameters assessed, we were not able to compute a MALT lymphoma-specific prognostic index with the ability to discriminate between different groups (data not shown).
Taken together, our findings suggest that the simple clinical parameters such as extragastric disease and multifocality are able to define patients with a high risk of relapse. While IPI and FLIPI are somewhat useful to predict the clinical course of MALT lymphomas, they failed to distinguish patients into the classical clinical four or three subgroups, respectively, again underscoring that MALT lymphoma is a distinct clinical lymphoma entity. In view of this, one can conclude that IPI and FLIPI allow only for crude overall risk assessment, but further studies to design a more clinically relevant index for MALT lymphoma are warranted.
Footnotes
- Received September 13, 2009.
- Revision received January 25, 2010.
- Accepted January 25, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved