

Abstract
Background/Aim: Vimentin expression in epithelial cells is reported to be associated with the malignant phenotype of cancer cells in vitro. However, the clinical significance of vimentin expression in carcinomas is not well understood. The aim of this study was to clarify the significance of vimentin-positive gastric cancer (GC). Patients and Methods: A total of 265 GCs were examined by immunofluorescent staining with antibodies against vimentin and carcinoembryonic antigen. GCs were determined to be vimentin-positive when cells were positive for both vimentin and carcinoembryonic antigen staining. Results: A total of 86 (32%) of 265 GCs were vimentin positive. There was a statistically significant correlation between vimentin-positive GCs and advanced clinical stage (p<0.001), macroscopic scirrhous-type (p<0.001), histological diffuse-type (p<0.001), lymph node metastasis (p=0.008) and lymphatic invasion (p=0.013). The prognosis of patients with vimentin-positive GCs was significantly (p<0.001) worse than that with vimentin-negative GCs. Conclusion: Vimentin expression might contribute to the high invasive phenotype of GC, and may be a useful biomarker to determine the biological aggressiveness of GC.
- Vimentin
- gastric carcinoma cells
- scirrhous type
- lymph node metastasis
- prognosis
Vimentin is a 57 kDa intermediate filament protein, which forms a part of the cytoskeleton (1). Vimentin is a characteristic component of mesenchymal cells and it is not usually expressed in epithelial cells (2). The epithelial–mesenchymal transition (EMT) is a process in which cells undergo a developmental switch from an epithelial to a mesenchymal phenotype (3). During the EMT, epithelial cells seem to acquire fibroblast-like properties, with changes in cell morphology, architecture, adhesion, and migration capacity (4). The expression of vimentin in epithelial cells is essential to the successive EMT through the interaction with actin and other intermediate filaments (5). Although the vimentin expression of cancer cells has been linked to a more malignant potential in vitro, the clinical significance of vimentin expression in carcinomas is still controversial (6, 7). The aberrant overexpression of vimentin has been linked to a more aggressive status in various tumors including melanoma (8), breast cancer (9, 10), cervical carcinoma (11), renal cell carcinoma (12), and prostate carcinoma (13). On the other hand, some reports have shown that vimentin expression does not inversely predict patient survival (14). Since gastric carcinoma is one of the most frequent causes of cancer death due to its high metastatic ability (15), vimentin expression of cancer cells might be correlated with more malignant phenotype in gastric carcinoma. However, there are few studies of the clinical significance of vimentin expression in gastric carcinoma. This study examined the significance of vimentin-positive cancer cells in gastric carcinoma.
Patients and Methods
Clinical materials. A total of 265 patients who had undergone resection of a primary gastric tumor at the host institute were enrolled in this study. Tumor specimens were fixed in 10% formaldehyde solution and embedded in paraffin. The pathologic diagnoses and classifications were made according to the Japanese Classification of Gastric Carcinoma. ‘Early cancer’ indicates cancer invasion limited to the submucosa, and ‘advanced cancer’ indicates cancer invasion into the muscularis propria or serosa. The median follow-up time for all 265 patients was 58 months (range 1 to 177 months). The median follow-up time for the patients that died of the disease was 25 months (n=88), compared with 75 months for surviving patients (n=177). A total of 31 patients were lost from the study after more than 60 months of follow-up.
Antibodies and reagents. FITC mouse monoclonal vimentin (clone VIM 3B4, Cat.No.61413) was obtained from PROGEN Biotechnik (Heidelberg, Germany). PE mouse anti-Human CD66 (carcinoembryonic antigen, CEA; clone B1.1/CD66, Cat.No.551480) was obtained from BD bioscience (Heidelberg, Germany). DAPI solution was obtained from WAKO (Kumamoto Japan).
Immunofluorescence microscopy. Triple-immunofluorescence labeling was performed to examine the presence of vimentin-positive gastric cancer cells. The slides were deparaffinized in xylene and hydrated in decreasing concentrations of ethyl alcohol. The tissues were heated for 20 min at 105°C and at 0.4 kg/cm2 by autoclave in Target Retrieval Solution (Dako Co., Carpinteria, CA, USA). The slides were washed with 0.01 M PBS, and then blocked with 3% BSA (diluted in PBS) for 30 min at room temperature. Sections were further incubated with anti-Human CD66 (CEA) antibody (1:100) and vimentin (1:50) and DAPI (1:10000) for 60 min at room temperature. The sections were washed with 0.01 M PBS (three times) and mounted. Stained sections were viewed under a fluorescence microscope Leica Digital Microscopy DMI 6000 (Leica Microsystems, Heidelberg, Germany). Images were captured with a Leica TCS SP5. All three fluorescent parameters were investigated in the same section by switching to the appropriate wavelength filter for each of the markers. Stained sections were viewed with a DAPI filter (365 nm excitation), CEA fluorescence with a PE filter (546 nm excitation), and antibody distribution with a FITC filter (450-490 nm excitation).
Immunofluorescence determination of vimentin. The tumor specimens showed various patterns of immunofluorescent staining against vimentin antibody. Cells were defined as being gastric cancer cells when they were positive for CD66 (CEA) staining. Vimentin expression level was analyzed semi-quantitatively according to the percentage of cancer cells showing vimentin positivity: 0, 0%; 1+, 1-9%; 2+, 10-20%; 3+, >20%. Vimentin expression was considered positive when scores were ≥2+, and negative when scores were ≤1+ (Figure 1). Four scratched fields were chosen randomly and the number of vimentin-positive cancer cell was counted from the images (×200). The slides were interpreted by two investigators without knowledge of the corresponding clinicopathological data. The relationships between various clinicopathological factors and vimentin-positive cancer cells were analyzed.
Statistical analysis. The χ2 test, Fisher's exact test or Mann-Whitney U-test were used to determine the significance of the differences between the covariates. Survival durations were calculated using the Kaplan-Meier method and were analyzed by the log-rank test to compare the cumulative survival durations in the patient groups. The Cox proportional hazards model was used to compute univariate and multivariate hazards ratios for the study parameters. For all tests, a p-value <0.05 was defined as statistically significant. The SPSS software program (SPSS ver.11 Tokyo, Japan) was used for the analyses.
Results
Correlation between clinicopathological factors and vimentin-positive cancer expression. Vimentin-positive expression was found in 86 (32%) out of 265 gastric carcinomas, in 20 (17%) out of 119 early gastric carcinomas and in 66 (45%) out of 146 advanced gastric carcinomas. CD66 (CEA) staining was positive for most of the gastric carcinomas. The relationship between vimentin-positive cancer and clinicopathological features are shown in Table I. The occurrence of vimentin-positive gastric cancer was significantly frequent in advanced stage of T2-T4 (p<0.001), macroscopically scirrhous-type, diffuse-type (p<0.001), lymph node metastasis (p=0.008), lymphatic invasion (p<0.013). In contrast, there was no statistically significant association between vimentin-positive expression and peritoneal dissemination, cytology positive, and venous invasion.
Survival. Figure 2 shows Kaplan-Meier overall survival curves in relation to vimentin-positive gastric cancer expression levels in gastric carcinomas. The survival curve was calculated from the date of surgery. The 5-year survival of the patients with vimentin-positive gastric cancer expression tumors was 56.9% in comparison to 78.5% for those patients with negative tumors (Figure 2A). The prognosis of patients with vimentin-positive gastric cancer was significantly worse (p=0.003) than that of patients with vimentin-negative gastric cancer. In 214 patients with curative resection (R0), the prognosis of with those with vimentin-positive gastric cancer expression tumors was significantly worse (p<0.001) than that of those with vimentin-negative gastric cancer expression tumors (Figure 2B). In univariate analysis (Table II), vimentin-positive cancer (p<0.001), advanced cancer (p<0.001), peritoneal dissemination (p<0.001), venous invasion (p=0.042), and lymph node metastasis (p<0.001) were correlated significantly with patient survival. In multivariate analysis (Table III), invasion depth, macroscopic type, and peritoneal dissemination were found to be independent prognostic factors, but not vimentin expression.
Discussion
Since a number of stromal cells, such as fibroblasts, express vimentin, it is difficult to distinguish vimentin-positive cancer cells from stromal cells by comparing two different slides of hematoxylin and eosin staining and vimentin staining. Therefore vimentin-positive cancer cells were examined using triple-immunofluorescence labeling by CEA, vimentin, and DAPI staining in a single slide. Through the use of immunofluorescent staining it was possible to distinguish vimentin-positive cancer cells from stromal cells.
In this study, the aberrant overexpression of vimentin was found in 85 (32%) out of 265 patients. The vimentin expression was significantly high in patients with advanced gastric cancer, especially those with macroscopically scirrhous-type gastric carcinoma. Moreover, vimentin-positive cancer was significantly associated with histologically diffuse-type, lymphatic invasion, lymph node metastasis. Macroscopically scirrhous type gastric cancer (type 4 carcinoma, diffusely infiltrating carcinoma, or linitis plastica-type) is characterized by cancer cell infiltration, reflecting frequent distant metastasis of cancer cells, and carries a worse prognosis among other types of gastric carcinomas (16, 17). The expression of vimentin in epithelial cells was essential to the EMT which is associated with the acquisition of invasive properties of cancer cells (18, 19). These findings suggest that vimentin expression might contribute to the highly invasive phenotype of scirrhous gastric carcinoma. Overexpression of transforming growth factor-β (TGF-β) was frequent in scirrhous gastric carcinoma (20), and TGF-β signals play an important role for the metastatic spread of cancer cells (21-23) such as migration, invasion, and EMT (4, 22, 24). These findings suggest that TGF-β might up-regulate vimentin expression, and affect the highly metastatic ability of scirrhous gastric cancer cells.
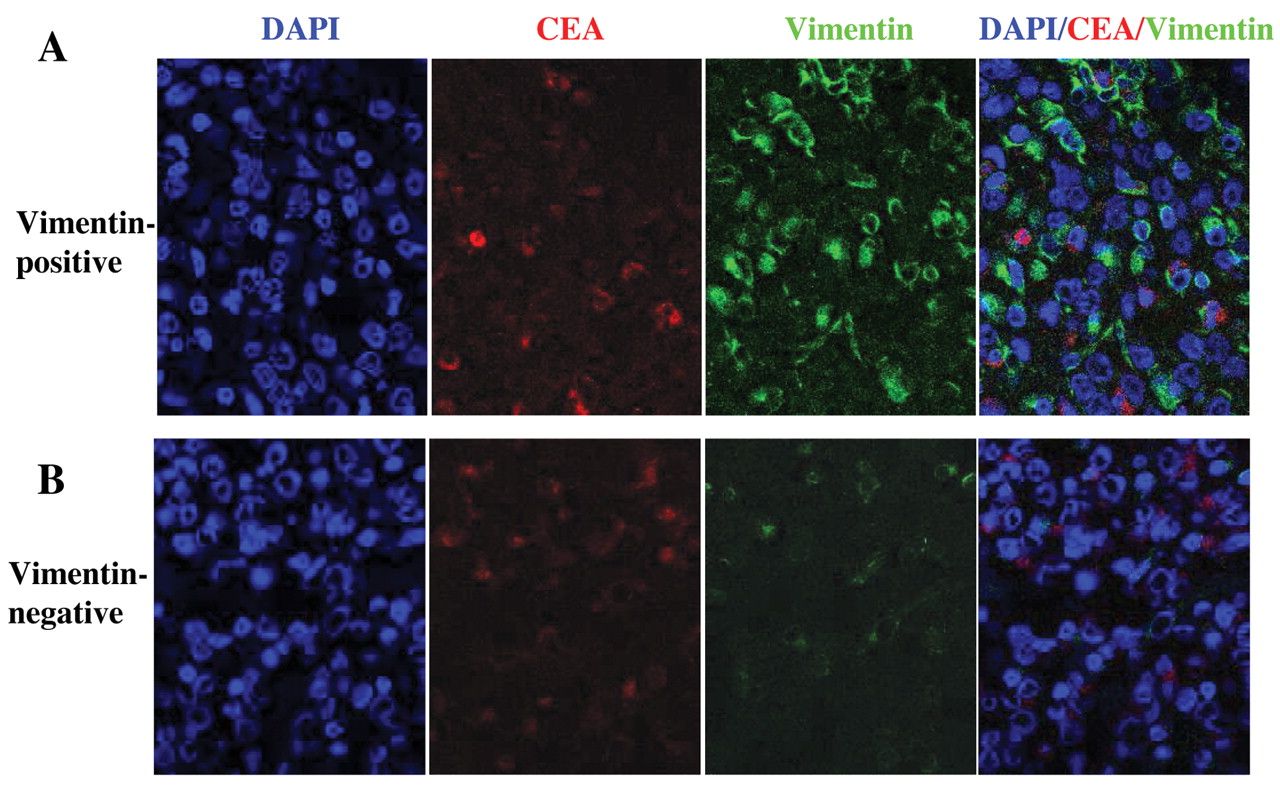
Immunofluorescent staining of vimentin expression in gastric cancer. A: The expression of vimentin was positive for 43% of CEA-positive gastric cancer cells. B: In contrast, vimentin expression was low (8%) in gastric cancer cells.

{kind=link}
{kind=link}
A: The overall survival of 265 patients based on vimentin expression. B: The overall survival of 214 patients with curative resection (R0).
Correlation between clinicopathological factors and vimentin-positive cancer.
The prognosis of patients with vimentin-positive gastric cancer was significantly worse than those with vimentin-negative gastric cancer, and in patients who had undergone curative R0 resection, the prognosis of those with vimentin-positive gastric cancer was significantly worse. Elevated vimentin expression level might be closely correlated with up-regulated migration and high invasiveness and poor prognosis of gastric carcinoma. On the other hand, multivariate survival analysis for all patients showed that vimentin expression did not influence the clinical outcome, suggesting that vimentin-positive gastric cancer expression was not an independent prognostic factor. Although vimentin failed to emerge as an independent prognostic factor, it was successful in identifying a subgroup of patients with disease of high malignancy. These findings suggested that vimentin expression might be a useful biomarker to determine the biological aggressiveness of gastric cancer.
Univariate analysis with respect to overall survival in gastric cancer.
Multivariate analysis with respect to overall survival in gastric cancer.
In conclusion, vimentin-positive gastric cancer was associated with the highly invasive phenotype of advanced gastric cancer, especially with scirrhous type of gastric carcinoma. Vimentin may play an important role in the metastasis of gastric carcinoma.
Acknowledgements
This study was supported in part by a Grant-in Aid for Scientific Research (C) 13671329 and (B) 13470260 from the Ministry of Education, Science, Sports, Culture and Technology of Japan, and by a Grant-in Aid for the Osaka City University Medical Research Foundation.
- Received October 19, 2010.
- Revision received November 15, 2010.
- Accepted November 16, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved