

Abstract
Background: Epidermal growth factor receptor (EGFR) mutational analysis has become essential in determining a therapeutic strategy for lung cancer. This study validated the reliability of recently generated rabbit monoclonal antibodies that recognise specific mutations of the EGFR protein. Patients and Methods: Pulmonary adenocarcinoma tissue from 20 previously genotyped specimens was prepared for immunohistochemical staining by two antibodies that recognise products of in-frame deletions in exon 19 (E746_A750del) and a point mutation that replaces leucine with arginine at codon 858 in exon 21 (L858R) of the EGFR gene. Results: The findings of EGFR-mutation-specific immunohistochemistry were concordant with the results of DNA analysis in 18 of 20 tested samples leading to 90% sensitivity and 100% specificity of the method. Conclusion: This immunohistochemical assay for products of representative EGFR gene mutations may be performed reliably using tissue specimens from resected pulmonary adenocarcinomas.
- Adenocarcinoma
- epidermal growth factor receptor
- immunohistochemistry
- lung cancer
- mutation
Molecular target therapy is important in the treatment of inoperable non-small cell lung cancer (NSCLC) with specific genetic aberrations. One representative target is the epidermal growth factor receptor (EGFR) (1, 2). Activating mutations within the tyrosine kinase domain of EGFR in NSCLC are directly associated with sensitivity to gefitinib and erlotinib, small molecules that act as EGFR tyrosine kinase inhibitors (EGFR-TKIs) (3, 4). EGFR mutational analysis, therefore, is essential for determining a therapeutic strategy in patients with NSCLC.
At present, DNA-based analysis such as direct DNA sequencing of PCR-amplified genomic DNA extracted from tumour tissue is the standard method for detecting EGFR mutations. However, sensitivity of direct DNA sequencing is limited by contamination with DNA from normal stromal cells. If the proportion of tumour cells among the cells in the sample is low, mutations are difficult to find by direct DNA sequencing. Recently, various molecular biological techniques have been developed to screen for genetic mutations in samples containing relatively few tumour cells. Microdissection of cancer cells from tissue specimens on glass slides followed by amplification of specific DNA fragments from the mutational hot spot of the EGFR gene is one such analysis (5, 6). Other highly sensitive and refined molecular methods for detecting EGFR mutants have been developed (7-9), but the need for special instruments and techniques renders them unsuitable for clinical laboratory use.
Although a variety of activating mutations within the EGFR gene have been reported, two types of mutations in exons 18 to 21 are common: in-frame deletions in exon 19 (E746_A750del) and a point mutation replacing leucine with arginine at codon 858 of exon 21 (L858R). Together, these two types of mutation account for 90% of all activating mutations of the EGFR gene (10). Recently, two commercially available rabbit monoclonal antibodies binding specifically to the above mutant EGFRs, E746_A750del and L858R, have been produced for immunohistochemical analysis (11).
Since immunohistochemical analysis is well-established, routinely performed for pathological diagnosis in clinical laboratories, mutation-specific EGFR detection using specific antibodies is much easier and more cost-effective than analysis of extracted DNA. In addition, immunohistochemical analysis is able to identify individual tumour cells carrying an EGFR mutation in tissue sections while still preserving tumour morphology. The present study evaluated the accuracy of genetic diagnosis for EGFR mutations using these two monoclonal antibodies in resected pulmonary adenocarcinoma specimens.
Results of immunohistochemistry
Patients and Methods
Clinical samples. This study was approved by the Institutional Review Board of St. Marianna University School of Medicine. A portion of the resected tumour obtained from patients who underwent surgery for lung cancer in the St. Marianna University Hospital was analysed. Written informed consent for genetic analysis of lung cancer specimens was obtained from all patients enrolled in this study. Among 20 samples of NSCLC preselected for evaluating the efficacy of EGFR mutation analysis by immunohistochemistry, 10 had an EGFR mutation and 10 did not.
DNA analysis to detect EGFR mutation. A peptide nucleic acid-locked nucleic acid polymerase chain reaction (PNA-LNA PCR) clamp method (7) was carried out to detect EGFR gene mutations within the tyrosine kinase domain, from exon 18 through exon 21, using DNA extracted from the resected lung cancer tissue specimens. If aberrations were identified by this method, further DNA sequencing was performed to determine the precise type of mutation. This DNA analysis was considered to be the ‘gold standard’ to which the capabilities of immunohistochemical detection were compared.
Immunohistochemistry to detect EGFR mutation. Three rabbit monoclonal antibodies, 6B6, 43B2, and D38B1, were obtained from Cell Signaling Technology (Boston, MA, USA). The 6B6 antibody detects EGFR molecules with an E746_A750 deletion, while the 43B2 antibody detects EGFR with an L858R point mutation. The D38B1 antibody, which recognises all forms of EGFR, was used as a positive control. Resected tumour specimens were stained simultaneously using these three antibodies according to the manufacturer's instructions. In brief, serial 4 μm-thick tissue sections were cut from formalin-fixed, paraffin-embedded blocks. Sections were deparaffinised in xylene and rehydrated through a graded series of ethanol concentrations. Antigen retrieval was carried out by microwave boiling for 10 min in 1 mM/l EDTA. Intrinsic peroxidase activity was blocked using 3% hydrogen peroxide for 10 min. After washing the sections with Tris-buffered saline (TBS), diluted primary antibodies (1: 200) were applied to cover the specimen. Sections were incubated at 4°C overnight. After three washes in TBS for 5 min each, slides were incubated for 30 min at room temperature with labelled polymer-HRP anti-rabbit secondary antibody (Envision+ kit; Dako, Glostrup, Denmark). Following three washes in TBS, the slides were visualised using substrate-chromagen (Dako). The sections were counterstained by haematoxylin for 2 min.
Evaluation of immunohistochemistry for EGFR mutation. Without knowledge of the results of the DNA analysis for EGFR gene mutations, the stained specimens were evaluated by the following procedure. Intensity of staining was graded as: (+), moderate to strong staining; (±), faint staining, and (−), no staining. Tumours graded as (±) were considered to show uncertain results.
Results
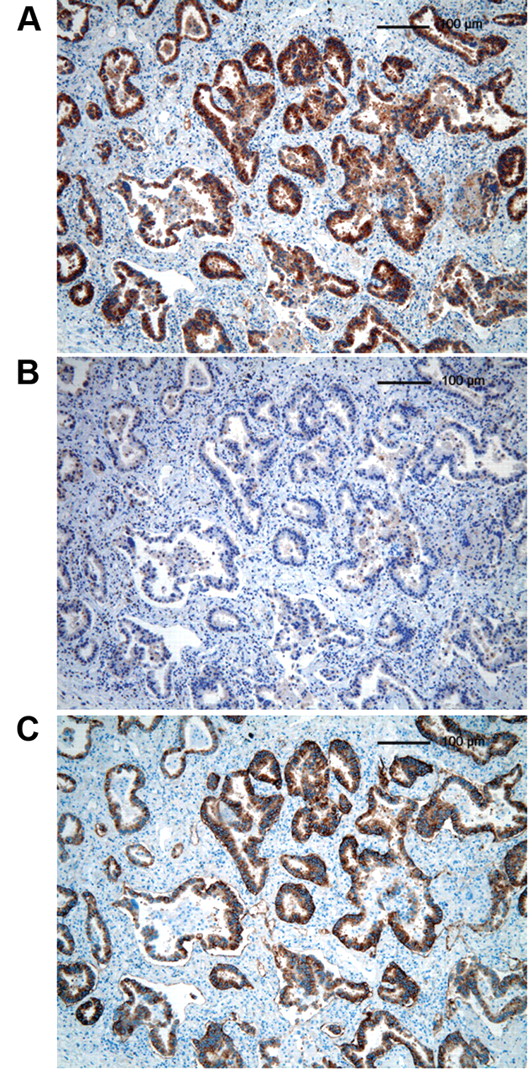
The results of the study are summarised in Table I. Types of EGFR gene mutations detected by DNA analysis were: L858R in five tumours, E746_A750del in three tumours and G719A and G719S in one tumour each. All 20 specimens were stained by the control antibody D38B1which recognises the EGFR protein non specifically, indicating that all paraffin blocks were in good condition. None of the non-mutant tumours were stained by any of the mutation-specific EGFR antibodies (43B2 or 6B6). All three E746_A750del tumours and four L858R tumours determined by DNA analysis were correctly diagnosed by immunohistochemistry (Figures 1 and 2). One L858R tumour (Table I, sample 2) was not diagnosed because of inconclusive staining by both 43B2 and 6B6 antibodies. One G719A tumour (Table I, sample 7) was misdiagnosed as E746_A750del because of a positive result using 6B6. Among the 20 samples examined, EGFR mutations were diagnosed correctly by EGFR mutation-specific immunohistochemistry in 18, leading to 90% sensitivity and 100% specificity for the method.
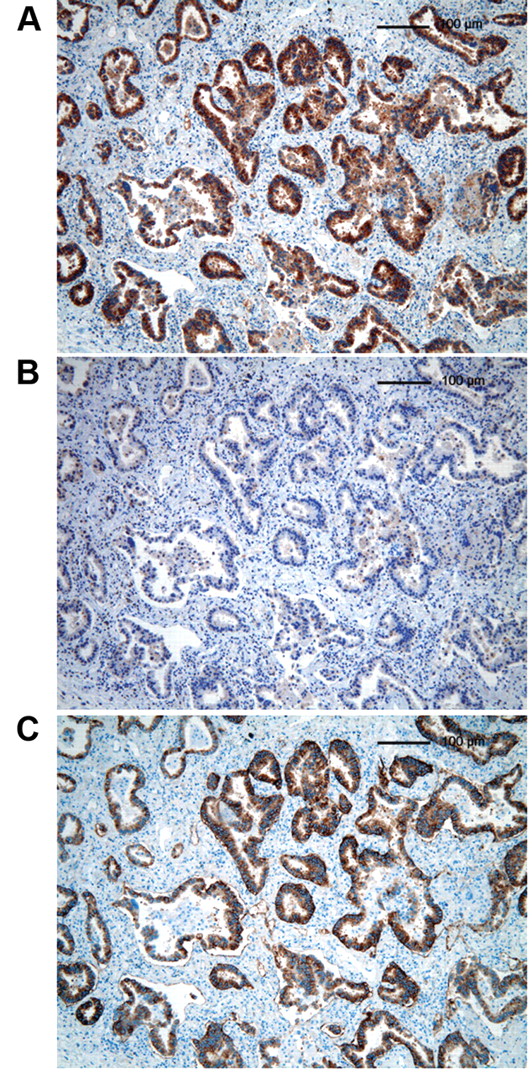
Immunohistochemistry of case 1, previously genotyped as having the E746_A750 deletion in the EGFR gene, ×100. A: The specimen was stained by the 6B6 antibody recognising E746_A750. B: The specimen showed no staining with the 43B2 antibody recognising the L858R point mutation. C: The specimen was stained by the D38B1 antibody recognising EGFR non specifically, indicating integrity of the tissue sample.

{kind=link}
{kind=link}
Immunohistochemistry of case 6, previously genotyped as having the L858R point mutation in the EGFR gene, ×100. A: The specimen was stained by the 6B6 antibody that recognised E746_A750, showing no staining. B: The specimen showed staining with the 43B2 antibody, which recognises the L858R point mutation. C: The specimen was stained by the D38B1 antibody recognising EGFR non specifically, confirming integrity of the tissue sample.
Discussion
In this study, rabbit monoclonal antibodies specific for EGFR mutations led to 90% of tumours carrying EGFR gene mutations to be correctly diagnosed. The initial report of these mutation-specific antibodies noted a sensitivity of 92% and a specificity of 99% (11). In the present study, the sensitivity was 90% and the specificity was 100%. Thus, the study obtained satisfactory results comparable to those of the initial report characterizing the diagnostic accuracy of this immunohistochemical method.
Though concordant results were obtained in most tumours, two of the examined cases showed conflicting results between DNA analysis and immunohistochemistry. One of these cases involved equivocal immunostaining. Since the positive control section in this case was well stained, this problem is not attributable to degradation of the paraffin block. As immunohistochemistry is essentially a qualitative assay, some equivocal results may be unavoidable. The other inconclusive result involved false-positive staining by antibody 6B6 of a tumour carrying the G719A mutation according to DNA analysis. The possibility that the tumour had different mutations in different areas of the lesion cannot be ruled out since different EGFR mutations are sometimes present heterogeneously in the same tumour (12, 13).
Immunohistochemical assays have several advantages over DNA analysis. Relationships between morphological features of tumour cells and genetic mutations may be studied by immunohistochemistry but not by DNA analysis of whole-tumour samples. Heterogeneity within tumours with respect to EGFR mutations may explain escape phenomena such as tumour re-growth after treatment with EGFR-TKI (14). Since immunohistochemistry may be performed using tiny tissue fragments obtained by bronchoscopic lung biopsy, this method may yield important information about EGFR mutations at the time of initial pathological diagnosis.
Until now, the method was able to diagnose two major types of representative EGFR mutations; however, other, minor mutations cannot be diagnosed by the currently available assays. The development of monoclonal antibodies that recognise TKI-resistant-mutations (15), in addition to other EGFR-activating mutations, is a very important goal.
In conclusion, the immunohistochemical detection of mutation-specific EGFR proteins was possible in resected pulmonary adenocarcinoma specimens. This assay system may be applicable to small tissue fragments obtained by a minimally invasive biopsy, providing useful information about pathophysiologically important mutations of the EGFR gene. Further studies are required to determine the strengths and limitations of this approach.
- Received October 14, 2010.
- Revision received November 5, 2010.
- Accepted November 8, 2010.
- Copyright© 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved