

Abstract
Advanced pancreatic adenocarcinoma is usually treated with single-agent gemcitabine chemotherapy or combinations that include gemcitabine application that have palliative benefit but do not lead to survival benefits. We present the results of preclinical and clinical studies using combination chemotherapies that include 41.8°C whole-body hyperthermia for pancreatic adenocarcinoma. Materials and Methods: DAN-G pancreatic carcinoma cells were treated with carboplatin and gemcitabine in vitro under hyperthermic conditions of 37°C, 39°C, 41.8°C and 43°C and cytotoxic drug effects were measured under various conditions using crystal violet assays. Data on outcome and toxicity of a clinical study using gemcitabine and carboplatin with 41.8°C whole-body hyperthermia in a compassionate manner in patients with advanced and heavily pretreated pancreatic adenocarcinoma are also shown. Results: In vitro data showed the DAN-G cells did not show increased responses to gemcitabine with or without carboplatinum under hyperthermic culture conditions at 39 and 41.8°C. Only temperatures of 43°C led to increased hyperthermic damage. Clinical data showed that a therapy of whole-body hyperthermia at 41.8°C with gemcitabine and carboplatin was well tolerated leading mainly to the expected hematological side-effects due to chemotherapy. The median overall survival after whole-body-hyperthemia was of 357 days, with a median progression-free survival of 140 days. Conclusion: Preclinical data indicate that hyperthermia does not increase the chemosensitivity of DAN-G pancreatic carcinoma cells to gemcitabine and carboplatin. Clinical data show that a treatment of pancreatic adenocarcinoma with C whole-body hyperthermia at 41.8° with gemcitabine and carboplatin is feasible for patients with advanced disease.
- Pancreatic carcinoma
- whole-body hyperthermia
- gemcitabine
- carboplatin
- cell lines
- clinical data
Pancreatic adenocarcinoma represents the fourth commonest cancer in Western Europe (Germany 10,700 new diseases each year) and the US (33,730 new diseases each year), and almost all patients are expected to die from the disease (1). Surgical resection offers a chance of cure for 15 to 20% of patients with resectable disease at diagnosis. Patients with advanced pancreatic adenocarcinoma have a dismal prognosis with a median survival of 8 to 12 month or less. Unresectable patients show either extensive peripancreatic lymphatic involvement and/or distant metastasis, or encasement, or occlusion of the superior mesenteric artery, inferior vena cava, aorta or celiac axis as assessed upon preoperative staging computed tomography scan or at the time of laparatomy (2). A variety of other imaging modalities, including magnetic resonance imaging (MRI) and endoscopic ultrasound, may be needed at times. Optimal treatment for locally advanced unresectable and metastatic pancreatic cancer is controversial including therapeutic options such as radiation alone, chemotherapy alone, and combined chemoradiotherapy with or without surgery. Metastatic disease is usually treated with single-agent gemcitabine chemotherapy or combinations that include gemcitabine application that lead to an improvement in quality of life and to a moderate increase in survival when compared to best supportive care. The first drug that showed some treatment benefits was 5-fluorouracil (5-FU) leading to median survivals of 10 to 24 weeks (3-5). Single-agent gemcitabine, which may be considered provisional standard chemotherapy for advanced metastatic adencarcinoma, showed a minimally prolonged median survival as compared to 5-FU (5.7 months vs. 4.4 months, 1-year survivals 18% vs. 2%) but a marked clinical benefit as measured through a parameter termed ‘clinical benefit responses’ (6) that measures pain intensity, use of analgesics, functional impairments and body weight changes (7). A Cochrane analysis that sumarizes the results of all published studies failed to demonstrate survival advantages for gemcitabine single-agent therapy (9). Combination chemotherapy including gemcitabine with other agents is feasible and may lead to moderate increases of median survival (10-13), but is also always associated with increased toxicities (14-16). Perfusional hyperthermia combined with chemotherapy and cytokines has successfully been employed for locoregional disease in sarcoma and melanoma patient (17). The rationale of 41.8°C radiant heat (Aquatherm) whole-body hyperthermia (WBH) (60 min.) in combination with chemotherapy as a treatment for advanced cancer, based on extensive preclinical studies, has been strong for decades (18). Preclinical research has so far focused on hyperthermia enhancement of selected antineoplastic agents such as mitoxantrone, cyclophosphamide, ifosfamide and cis-diaminedichloroplatinum (carboplatin) and melphalan (19-27). The biological basis for hyperthermia effects are related to the inhibition of chemotherapy resistance and increased cellular drug penetration (21, 28-32). Some studies demonstrated an improvement in terms of therapeutic index (i.e. the relative ratio of neoplastic toxicity to normal tissue toxicity) (21, 25, 28, 33), others the induction of cytokines (27, 33-35). Consequently, a number of phase 1 and phase 2 studies have proven the feasability and efficacy of a treatment with WBH combined with chemotherapy for a variety of tumor types (36).
Encouraged by these favorable results and the poor results for the treatment of pancreatic carcinoma, we initiated a pilot study that allowed compassionate treatment of heavily pretreated patients with WBH with gemcitabine and carboplatin. At the same time, in vitro analyses were performed to provide a basis for this treatment.
Materials and Methods
In vitro chemotherapy. Drug administration was performed by replacing normal media with carbolatedplatin and/or gemcitabine-containing media in increasing concentrations for 1 h, after which the therapeutic medium was replaced with normal medium and the cells further incubated. Carboplatin (Bristol-Meyers Squibb, NJ, USA) and gemcitabine (Lilly, Bad Homburg, Germany) were purchased and handled as indicated by the manufacturers.
Cells were treated with carboplatin and gemcitabine, and the drug concentration leading to 50% growth inhibition (IC50) was determined, which enables determination of positive and negative deviations. Tested dose ranges were carboplatin at 20-200 μg per ml and gemcitabine at 0.025-500 μg per ml. These levels correspond to therapeutic plasma concentrations. In order to heat the cells for one hour under controlled conditions at 39, 41.8 and 43°C, they were put in Safelock 2 ml Eppendorf tubes and placed in a water-bath that had been preheated for 15 minutes (37). The temperatures were continuously monitored with a thermometer during each experiment.
Cell line and culture. The human malignant pancreatic adenocarcinoma cell line DAN-G, having a cell doubling time of 33 hours (38) was used for in vitro studies (obtained from the Tumor Cell Collection of the Deutsches Krebsinstitut, Heidelberg, Germany). Cells were maintained as subconfluent monolayers in 75 cm2 culture flasks at 37°C in a humidified atmosphere with 5% CO2. Cells were maintained in RPMI-1640 culture medium supplemented with 10% fetal calf serum, 2 mM L-glutamine and 1% MEM non-essential amino acid solution (all reagents: Biochrom, Berlin, Germany). The cells were fed or subcultured once or twice a week depending on cell density. For experimental purposes, cells were seeded either on Thermanox plastic coverslips (Merck Eurolab, Hamburg, Germany) or glass coverslips in 6-well plates at a density of 2×105 cells per well and allowed to settle for 24 h before beginning therapy. Preliminary experiments (data not shown) showed that DAN-G cells display linear growth curves when seeded in the range of 500 to 10,000 cells as determined by cell numbers and optical density (crystal violet assay, see below) so that the optimal seeding conditions were found to be 5,000 cells per dish.
Assaying crystal violet binding capacity (Crystal violet assay). Determination of cell mass as a measurement of the proliferation after exposure to cytostatic drugs and capacity of survival of the cell line was performed with the standardized crystal violet assay for monolayer cultures (39, 40) that correlates with the biomass of cells (41). The amount of crystal violet released through acetic acid photometrically determined is directly proportional to the number of live cells. In brief, the supernatants of the culture were discarded and the DAN-G cell layers were immediately incubated with crystal violet (Chroma, Stuttgart, Germany) solution (0.2% w/v with ethanol 2% v/v in 0.5 M Tris-C1, pH 7.8; 1 ml per well) at room temperature for 10 min. The stained cell layers were rinsed thoroughly with 0.5 M Tris-C1 (pH 7.8, 5×2 ml), air dried and incubated with SDS solution (0.5% w/v with ethanol 50% v/v in 0.5 M Tris-C1, pH 7.8) for 60 min at 37°C under Parafilm occlusion. Meanwhile, crystal violet was completely released from the cells into the supernatant. The absorbance of this supernatant was scanned in a DU Series 70 Beckman spectrophotometer and read at a fixed wavelength of 586 nm (42). For quantitative evaluation, the Student's t-test was applied according to standard methods in order to determine differences between the controls and the treatment groups of each drug concentration (for determinations IC50 concentrations) or of treatment groups at different temperatures.
Light microscopy. Cells were rinsed once with warm phosphate-buffered saline (PBS), fixed with 4% buffered formaldehyde for at least 1 h, stained with Mayer's hematoxylin/eosin (HE), dehydrated through a graded alcohol series followed by xylene incubation and finally mounted with Entellan (Merck Eurolab, Hamburg, Germany). Slides were examined with a Zeiss Axiophot and findings documented on Agfapan 25 films.
Immunochemical procedure for cell cycle analysis. For the detection of BrdUrd incorporated into DNA, a denaturation step of DNA was performed. Cells were denaturated with 4N HCl for 10-20 min at 20°C. Flow cytometric analysis of the cell cycle was then performed. After denaturation of DNA, the cells were stained by an indirect immunofluorescence method using a commercially available monoclonal anti-BrdUrd antibody (43).
Patient characteristics of thirteen patients with advanced progressive pancreatic adenocarcinoma not amenable to other treatment. Patients were treated with gemcitabine and carboplatin with 41.8°C WBH as described in the Materials and Methods section. Median age was 57 years. All patients had metastatic disease spread to the liver.
Clinical study of Thermochemotherapy
Patient selection. Thirteen patients with histologically confirmed advanced progressive pancreatic adenocarcinoma not amenable to other treatment were treated at the University of Lübeck between May/2000 and March/2003. Patients were informed of the investigational nature of this study and signed an informed consent form approved by the Ethics Committee. The study was approved by the Institutional Review Board at the University of Lübeck. Patients were pretreated: most had received gemcitabine and were progressive on treatment with this agent. The patients referred underwent pathology review at the University of Lübeck. Patients were over 18 years of age and had to have a projected life expectancy of at least 12 weeks and an ECOG performance status of ≤2. Medical history, physical examination and extensive preregistration screening was performed. Chest X-ray, electrogardiogram (ECG), exercise Multiple Gated Acquisition scan (MUGA) scan or dopamine stress ultrasonography, pulmonary function tests, abdominal and brain computed tomography (CT) scan, full hematology and chemistry panels, and urinanalysis were performed. Patients were not allowed to receive prior chemotherapy within 4 weeks before study enrollment or radiation within 2 weeks prior to study enrollment. No other chemotherapeutic or hormonal agents were allowed while the patients were in the study. A demographic profile of patients is presented in Table I. Patients were required to have adequate bone marrow function (defined as WBC >3,000 cells/μL, an absolute granulocyte count ≥1,000 cell/μL and a platelet count of ≥100,000 cells/μl), adequate liver function (total bilirubin ≤1.5mg%, alkaline phosphatase and AST 3x upper normal limit; total protein not less than 15% of lower normal limit), adequate renal function (creatinine <1.2 mg%, and BUN ≤30 mg%, or creatinine clearance ≥60ml/min) and normal metabolic parameters (calcium and serum electrolyte values). Patients with a history of an allergy to lidocaine, malignant hyperthermia associated with general anesthesia, documented coronary artery disease, angina, congestive heart failure, or serious dysrhythmias were excluded. The protocol excluded patients with severely compromised respiratory status, i.e. any component of full pulmonary function tests being less than 60% of predicted. Neurological reasons for exclusion were central nervous involvement by tumor, previous spinal cord or brain irradiation, documented peripheral neuropathy (paraneoplastic or otherwise), or a history of emotional instability.
Chemotherapy. Gemcitabine was infused over 30 min at a dose of 800 mg/m2 at room temperature on days 0, 8 and 15. Carboplatin (Bristol-Meyers Squibb) was infused over 20 minutes at a dose of area under the curve 5 (AUC 5), 10 min after achieving 41.8°C as assessed using an esophageal probe.
WBH treatment procedure and supportive care. The WBH treatment procedure was performed as described elsewhere (44). A hyperthermia treatment session was defined as raising a patient's systemic temperature (maximum temperature recorded by either rectal or esophageal probe, usually both) to 41.8°C±0.2°C and maintaining this level for 60 min. The patient was removed from the WBH device and systemic temperatures were maintained by keeping a vapor barrier on the patient to minimize evaporative losses. To terminate a hyperthermia treatment, the vapor barrier was removed to allow physiological temperature regulation. The Aquatherm system for delivering WBH (patent, Cancer Research Institute, New York, NY, USA) has been described in detail elsewhere (45). Briefly, the apparatus produces radiant heat through circulating hot water in a cylinder constructed on the basis of a copper tubing; the design incorporates a countercurrent distribution system to maintain thermal constancy. Other features include a humidification system to eliminate evaporative heat losses. Esophageal, rectal, skin and ambient air temperatures are monitored continuously and recorded at a minimum of 10-min intervals (44, 45). During all hyperthermia treatments, patients received nasal oxygen at a rate of 2-6 l/min. Patients received 0.75-1.0 l i.v. 5% dextrose in 0.25 N saline per hour alternated with 5% dextrose in 0.5 N saline plus approximately 7.5 mEq of KCl/l. Body weight, urinary output (75 ml/h) and electrolytes were monitored to ensure fluid and electrolyte homeostasis during and after the procedure. A typical WBH treatment lasted 4 hours, including 1.3 h to reach target temperature, 1 h at 41.8°C, and a 1-hour cooling phase (44). Post-treatment, patients received normal saline 500-1000 ml as needed to maintain systolic blood pressures >90 mmHg. Patients were sedated during WBH with a combination of i.v. thiopental (4 mg/ml) as described (44), as well as incremental boluses of i.v. midazolam (2-5 mg) and i.v. fentanyl (25-50 μg). Droperidol (1.25-5 mg) was administered during the first 30 min of WBH therapy for both its sedative and antiemetic effects. The aim of sedation was to have a patient who could respond to verbal stimulation and continue spontaneous respirations at a rate >10 breaths/min. During the procedure, heart rate, respiratory rate, oxygen saturation and cardiac rhythm were continuously monitored in all patients. Blood pressure (systolic/diastolic) was monitored at least every 10 min. Patients were observed after treatment for 20-24 h prior to discharge. Some patients received 10.35 mg of metoclopramide i.v. after WBH as a prophylaxis against the gastric stasis effect of thiopental. Patients received granistron with dexamethasone for emetic prophylaxis.
Duration of treatment. Patients received a second cycle of therapy 4 weeks after the first cycle if sufficiently recovered from toxicity.
Evaluation for toxicity. Laboratory values, including blood counts and serum chemistries, were assessed at least weekly. Toxicity was assessed weekly and graded. All patients were evaluated for toxicity. According to WHO criteria.
Evaluation for response. Patients were required to undergo at least two cycles of therapy to be evaluated for response.
Results
Quantitative measurements of inhibitory concentration of carboplatin and gemcitabine leading to 50% DAN-G cell death (IC50). Carboplatin induced an obvious dose-dependent cell killing of cultured DAN-G cells in a range of 20-200 μg/ml using the crystal violet assay. The inhibitory concentration leading to 50% cell death (IC50) was 69.24 μg/ml of carboplatin. At a concentration of 200 μg/ml, which was the maximum used in these experiments, 90% of seeded cells were killed by carboplatin. The IC50 of gemcitabine was 0.0988 μg/ml. Notably, the inhibitory curve for gemcitabine showed an unexpected pattern, in which even high increases of drug concentrations led to cell kill fractions of approximatly 30%. Higher concentrations were not tested as the upper ones used here already exceed plasma equivalents that may be used in clinical practice.
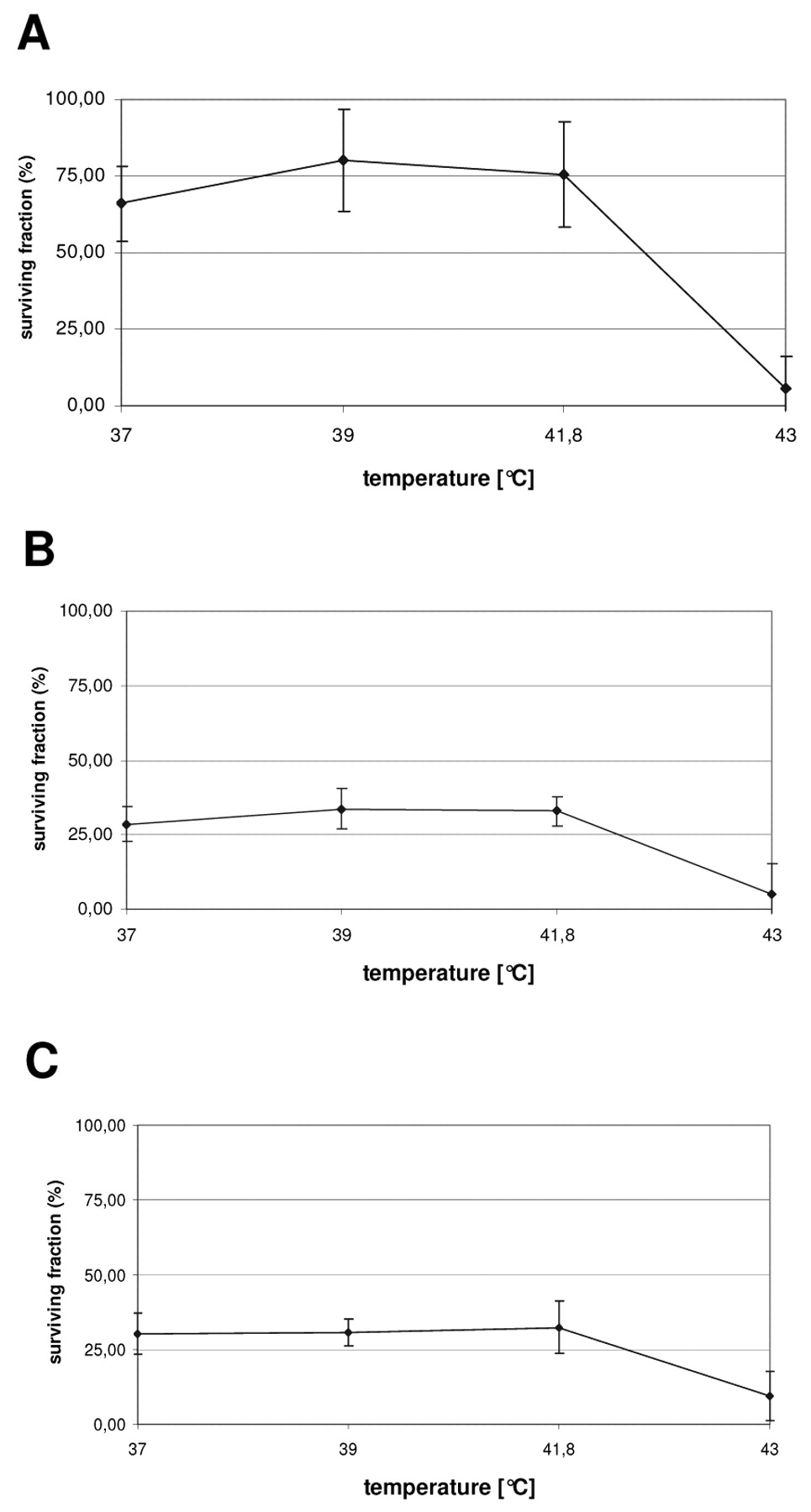
The effects of hyperthermia on the survival of DAN-G cells under treatment with carboplatin and gemcitabine at IC50 dosage. In order to study the effects of hyperthermia alone on cell survival, untreated DAN-G cells were cultured and incubated in a preheated controlled water-bath at 37°C, 39°C, 41.8°C and 43°C (38) and analyzed for survival by crystal violet assay. The results show that there was no decrease in cell number, which would have been considered a positive therapeutic effect, at any temperature between 37°C and 41.8°C (data not shown). A further increase of the temperature to 43°C led to apoptosis of all the DAN-G cells in culture (data not shown). The effects of hyperthermia on DAN-G cell survival were also studied on cells that were grown in a preheated controlled water bath at 37°C, 39°C, 41.8°C and 43°C (38) with carboplatin and/or gemcitabine at IC50 concentrations and were then analyzed for survival by crystal violet assay. For carboplatin at IC50, a culture of DAN-G cells at 37°C led to expected decreases in cell numbers as compared to seeded cells alone. The DAN-G cell kill was somewhat decreased at 39°C and 41.8°C as compared to cells grown at 37°C (Figure 1A). Cell numbers were 65.9% at 37°C, 80.22% at 39°C and 75.51% at 41.8°C. After culture at a temperature 43°C, only 5.53% survived, thus almost all DAN-G cells in culture underwent apoptosis as occurred in cultures without cytotoxic drug (Figure 1A). Gemcitabine at IC50 as determined in dose-finding experiments described above, led to a somewhat higher cell kill than expected. Survival was 27% of the input cell number; this result was seen in all repeats. As the culture conditions were consistent, this did not affect intrinsically the results of the hyperthermia experiments. Again, application of hyperthermic conditions in at 39°C and 41.8°C to cultures with gemcitabine at IC50 did not increase cell kill. Intact, cell numbers were 33.61% and 32.84% respectively, thus slightly higher than in cells grown with gemcitabine at 37°C. Culture at 43°C led to cell survival of 5.19% (Figure 1B).
When cells were grown at 37°C with both carboplatin at IC50 and gemcitabine at IC50, 30.12% of the cells survived, 30.55% survived at 39°C and 32.26% survived at 41.8°C. At 43°C, the cell numbers decrease markedly to 9.37% (Figure 1C). When comparing the results, a combination of carboplatin at IC50 with gemcitabine at IC50 did not lead to improved cell kill as compared with gemcitabine IC50 alone. Hyperthermic conditions did not lead to increased cell death at any time as compared to 37°C. High temperatures of 43°C, which are incompatible with clinical WBH, led to very high cell death fractions in all the experimental settings. In order to analyze the effects of application of these cytostatics in succession, experiments examining three different approaches were also performed. In the first, carboplatin and gemcitabine were added at the same time point. In the second, carboplatin was added first and gemcitabine was added 30 min later. In the third approach, gemcitabine was added first and carboplatin was added 30 min thereafter. The first approach led to reduced cell numbers of 35.5% of input; the second, carboplatin first with gemcitabine 30 min later, led to cell numbers of 37.31% of input; the third led to cell numbers of 34.14% input. There was no difference in cell kill of DAN-G cells observed through application of these cytostatics in succession.
Cell cycle analysis of DAN-G cells under treatment with carboplatin and gemcitabine at IC50 dosages and hyperthermia. As DAN-G cells did not show any thermosensitivity, repeat experiments included cell cycle analysis as thermo- and chemoresistance might be explained by high G0/G1 fractions as opposed to S-phase fractions (46). Cell cycle analysis was performed using fluorescent cell marking according to Dean et al. (47). Cell cycle fractions were 40-50% in G0/G1, 8-12% G2 and 40-50% S-phase at 37°C and did not differ with temperatures of 39°C and 41.8°C. There were no significant differences in cell cycle fractions after treatment with carboplatin at IC50, gemcitabine at IC50 or a combination of both drugs as differences monitored were 10% at the most.

Survival of DAN-G cells after treatment with carboplatin and/or gemcitabine. Line graphs showing the survival of DAN-G cells after treatment with carboplatin and/or gemcitabine at IC50 at 37°C, 39°C, 41.8°C and 43°C compared to untreated controls as analyzed by crystal violet assay. (A) DAN-G cells cultured with (A) carboplatin, (B) gemcitabine and (C) with both carboplatin and gemcitabine. Graphs show the mean values of 5 repeat experiments using 6-well plates for each timepoint and temperature with bars indicating the standard error of means. Hyperthermic conditions of 39°C and 41.8°C did not lead to increased cell death at any time as compared to 37°C. A temperature of 41.8°C corresponds to the temperature that is generally used for clinical WBH. Statistically relevant increases in cell kill were detected in all groups at very high temperatures of 43°C. This temperature would be incompatible for clinical WBH.
{kind=link}
{kind=link}
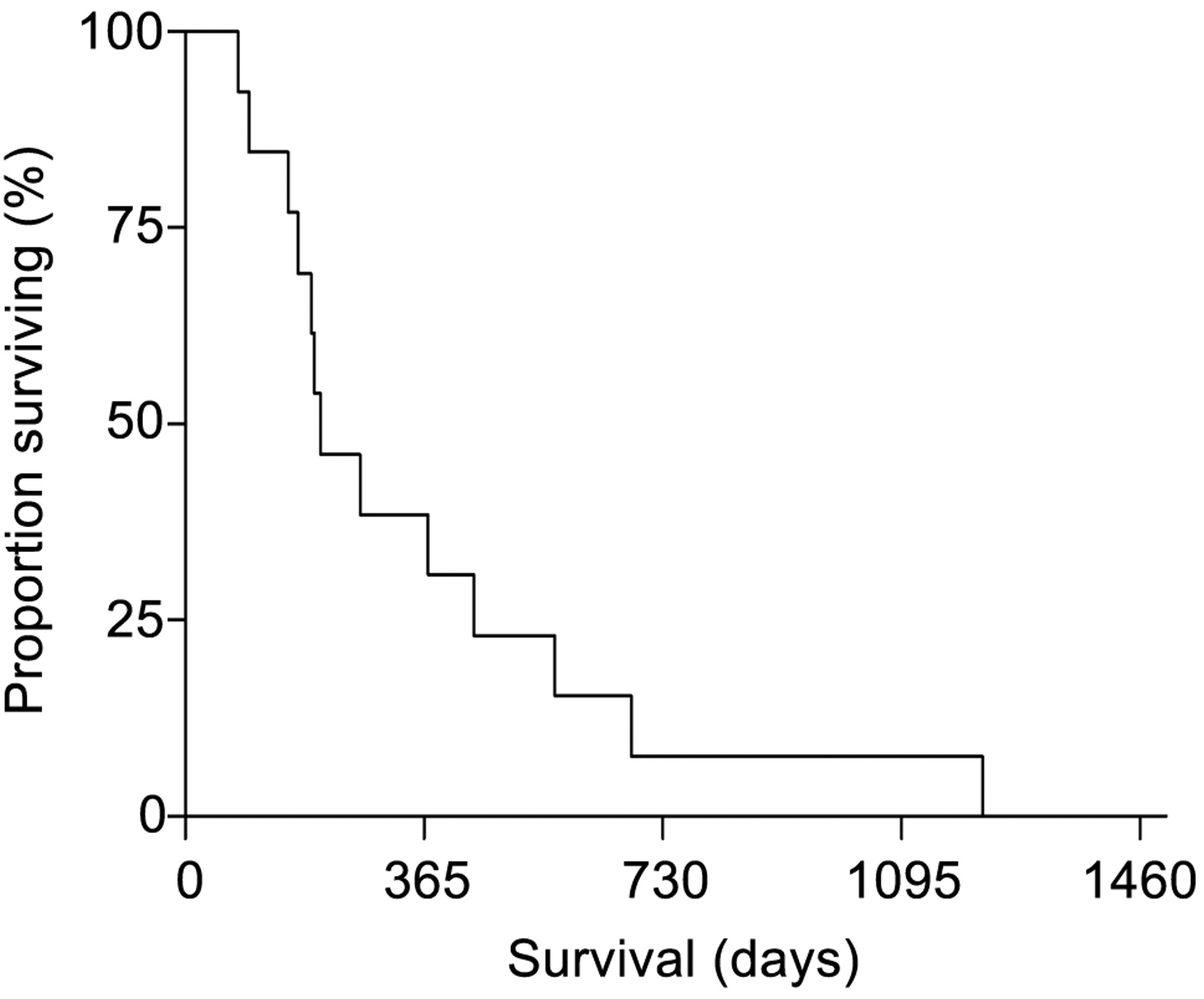
Kaplan-Meier analysis of survival for all patients who entered the study. Of thirteen patients with metastatic pancreatic adenocarcinoma receiving gemcitabine and carboplatin with 41.8°C WBH, 3 patients achieved a partial remission and 5 stabilization of disease. The median progression-free period of all patients was 4.7 months. The median survival was 11.4 months and the one year survival was 38%.
Toxicity and survival data of 13 patients with advanced pancreatic adenocarcinoma treated with carboplatin and gemcitabine combined with 41.8°C WBH. Thirteen patients with stage IVB pancreatic adenocarcinoma (all with liver metastasis) were treated in this study. As described in the Materials and Methods section, they received gemcitabine without WBH on days 0, 8, 15 and carboplatin with 41.8°C WBH (60 min) on day 1. The patients' median age was 57 years. In addition to liver metastasis, 4 had tumor infiltration of the stomach and the duodenum. Patients were assessed for therapy response. Three patients achieved a partial remission and 5 (38%) stabilization of disease. The median progression-free period of all patients was 4.7 months. The median survival was 11.4 months. The patients who achieved partial remission had a median survival of 15.8 months. One year survival was 38% (Figure 2).The main toxicity was myelosuppression leading to grade 3 leukopenia in 25% and WHO grade 4 thrombocytopenia in 25% (Table II).
Discussion
A number of preclinical and clinical studies showed the efficacy of WBH with chemotherapy for a number of malignant tumors (18, 48-53). Here we report on two different aspects/principles that may give insights to evaluate the influence of a treatment of WBH with chemotherapy for adenocarcinoma of the pancreas. The in vitro data that we present using the crystal violet assay as a measurement of cytotoxicity in the DAN-G cell model show that there is no additional effect of hyperthermia to the effects of cytotoxic chemotherapy with carboplatin and/or gemcitabine. Application of 39°C and 41.8°C along with carboplatin led to lower drug effects of 10 to 15% less cell death in DAN-G cells. This study shows a similar decrease of drug effects with hyperthermia and gemcitabine. Other tumor models, as for pulmonary and a bladder carcinoma, showed a positive synergistic effect of hyperthermia and gemcitabine treatment (52, 54). Thus pancreatic adenocarcinomas may be inherently more resistant to drug and hyperthermic effects. As a combination of carboplatin with gemcitabine showed synergistic effects on cell lines in other preclinical studies (55-57) and as the combination of these drugs led to positive clinical effects in the treatment of patients with pancreatic adenocarcinoma (16, 58, 59), we hypothesized that this combination of gemcitabine and carboplatin with hyperthermia could be synergistic. Nevertheless, the results were negative, showing no additive effects of this combination when used on DAN-G cells. DAN-G cells have been shown to be representative of the behavior of pancreatic carcinomas within the limits of preclinical studies, which substantiates the usefulness of these findings (36, 60, 61). A possible explanation for the efficacy of hyperthermia with cytotoxics in other entities is the induction of a cell cycle shift towards the S-phase (46). The importance of the prognosis of actively cycling cells with high S-phase fractions has been shown to be of importance in clinical medicine with and without hyperthermia (62, 63). We thus studied the influence of hyperthermia with and without the cytotoxics gemcitabine and carboplatin on the cell cycle of DAN-G cells in culture. This data show that the cell cycle phase fraction remained unchanged throughout clinically applicable temperatures between 37°C and 41.8°C. We also found relatively high proportions of DAN-G cells in S-phase undergoing mitosis (30-40% at the end of culture) while 40 to 50% of the cells were in G0 phase. This is indicative of high mitotic activity on the one hand, but does not point towards active cell cycling as a parameter of sensitivity to therapy. There are no clinical data available on WBH with chemotherapy on the treatment of advanced adenocarcinoma of the pancreas, thus we also analyzed the clinical outcome of 13 patients treated on a compassionate use basis with carboplatin and gemcitabine combined with 41.8°C WBH. The rationale for WBH in combination with chemotherapy as a treatment for advanced cancer, based on extensive preclinical studies, has been strong for decades (18). However, the toxicity associated with extracorporeal WBH has precluded the conduct of larger, multi-institutional studies of WBH until recently (47, 64). The use of a radiant heat WBH device has eliminated such excessive toxicity (45). The toxicity and efficacy of (ICE) chemotherapy concurrent with WBH was studied in patients with advanced soft tissue sarcomas and pleural mesothelioma showing positive effects. The cytotoxic drugs that were used in this context were gemcitabine and carboplatin, which are drugs with proven efficacy for this disease, the latter also having synergistic effects with WBH in other diseases. The patients included in this study were heavily pretreated thus representing a bad prognostic group even among pancreatic carcinoma patients (for details of patients characteristics see Table I). Patients apt to undergo a treatment with WBH are rare as this requires a good performance status without signs of cardiac, pulmonary or renal disease. Treatment showed surprising activity in these patients: 23% of the patients achieved a partial remission and 38% achieved stable disease. Another 38% of the patients did not show response but progressed. Median survival of all patients was 11.8 months. This is longer than the median survival rates achieved with other drugs and surpasses even the data of the treatment of advanced pancreatic adenocarcinoma achieved with gemcitabine alone in drug naive patients, which was 5.7 months (6). The rate of side-effects with this therapy was acceptable. Patients required hospitalization terms of 4 days. Nausea and vomiting were well controlled through efficient antiemetic medication. All patients required rehydration due to mild signs of dehydration. Relevant grade III or IV hematotoxicity was seen no sooner than after the third cycle. Nevertheless, there were only four patients that agreed to more than two cycles as patients were either progressive or considered the treatment as too dermanding.
Reported toxicities of thirteen patients that had received therapy with gemcitabine and carboplatin with 41.8°C WBH. The main toxicities were myelosuppression leading to grade 3 leukopenia in 25%, and WHO grade 4 thrombocytopenia in 25%.
To summarize, the small patient numbers and selection make objective judgment about this treatment modality difficult. This study shows on the other hand at least feasibility of this treatment for some of the patients with advanced disease. Cost efficacy is not very good as hospitalization and expensive supportive care are required. We conclude that WBH with gemcitabine and carboplatin is feasible for some patients with advanced adenocarcinoma of the pancreas that may lead to some clinical benefit, although preclinical data do not support its use for this entity.
Footnotes
-
* Both authors contributed equally to this work.
- Received February 9, 2009.
- Revision received June 2, 2009.
- Accepted June 17, 2009.
- Copyright© 2009 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved