


Abstract
Background/Aim: Head and neck squamous cell carcinoma (HNSCC) is characterized by high relapse rates and low survival in comparison to other malignancies. Patients and Methods: Fifty-two patients suffering from recurrent HNSCC were compared, analyzing the impact of different regimes, including surgery, radiotherapy (RT), chemotherapy and immunotherapy on progression-free survival (PFS), overall survival (OS), locoregional control (LRC), and adverse events. Results: The standard RT technique was intensity-modulated radiotherapy (IMRT) in all patients. In the multivariate analysis, higher cumulative RT dose significantly influenced LRC whereas surgery and age significantly impacted PFS and OS. Conclusion: IMRT dose-escalation, as well as surgery, appear beneficial in the treatment of recurrent HNSCC. Moreover, nivolumab and platin-based therapy might be superior agents for systemic therapy in comparison to cetuximab.
- Recurrent head and neck cancer
- squamous cell carcinoma
- intensity-modulated radiotherapy
- local control
- prognosis
- immunotherapy
- salvage surgery
Head and neck cancer is a common neoplasm with a rising incidence and worldwide more than 600,000 new cases annually (1). It often arises from epithelial cells, especially squamous cells, representing 90% of all head and neck carcinomas (2). Carcinomas in the head and neck are frequently diagnosed in a locally advanced stage and represent a significant threat to patients’ lives (3-5). Head and neck squamous cell carcinoma (HNSCC) requires special treatment due to its location next to vital structures and organs and associated limitations of extensive surgery. An individual combination of therapy options is most commonly used, considering location, distinction, histological patterns, and patient characteristics (6). The aim is to treat the tumor and at the same time prevent a recurrence, grand reduction in quality of life, and long-term toxicities. Established approaches for the primary treatment of HNSCC include open and minimally invasive surgical interventions (7). Radiotherapy (RT) is beneficial in patients with locally advanced and large tumors or close resection margins (8, 9).
Moreover, adjuvant radiochemotherapy is used to treat primary tumor and micro metastases. In addition, platin-based chemotherapy and cetuximab, an EGFR-inhibitor, have proved to be efficient (10, 11). Despite aggressive primary treatment with curative intent, relapse rates are high in the form of distant metastases or locoregional recurrences (12). However, treatment for recurrent squamous cell carcinomas has been less investigated than for primary tumors (13, 14).
Agents used to treat recurrent HNSCC include cisplatin, methotrexate, paclitaxel, docetaxel, cetuximab, pembrolizumab, and 5-FU (15). In addition, nivolumab, an anti-PD-1 monoclonal antibody, presents an established agent after the failure of platinum-based therapy (16, 17). Various randomized phase III trials comparing anti-PD(L)-antibodies as a treatment alone or combined with chemotherapy are ongoing.
The purpose of this analysis is to investigate the effects of different surgery, RT, and chemotherapy regimens on overall survival (OS), progression-free survival (PFS), and locoregional control (LRC) rates for patients with recurrent HNSCC. Moreover, RT toxicities have been examined, considering in- or outfield radiation and the cumulative applied RT dose.
Patients and Methods
Patient selection. We conducted a retrospective cohort study based on 196 patients treated for HNSCC in our institution between 2012 and 2018. In our study, we included patients who met the following inclusion criteria: patients at the age of 18 years or older, with a local recurrence from a histological confirmed HNSCC, pre-treatment of the primary carcinoma in the head and neck, completion of treatment course, and a minimum follow-up time of 3 months (Figure 1). Patients only with distant recurrence were excluded (N=26). In addition, all patients were classified according to the TNM-classification version 8 (18). Common Terminology Criteria for Adverse Events (AEs) was used to assess toxicities. In this analysis, fifty-two patients filled the inclusion criteria.

Patient selection.
Therapy. After the initial diagnosis of HNSCC, twenty-seven (52%) subjects experienced surgical resection of the primary neoplasm, 46 (89%) patients underwent RT of the primary tumor, and 38 patients (73%) also had concurrent chemotherapy. The primary radiochemotherapy regimens included cisplatin (N=27), carboplatin (N=12) and cetuximab (N=3).
In the relapse situation, eleven patients (21%) underwent surgery of the locally recurrent tumor, 45 patients (87%) underwent re-irradiation of the locally recurrent HNSCC using intensity-modulated radiotherapy (IMRT) with a medium RT dose of 45 Gy and a medium fraction dose of 1.8 Gy. Forty-four (85%) patients received salvage concurrent chemotherapy. Chemotherapy regimens included platin-based therapy (cisplatin N=10 and carboplatin N=10) or cetuximab (N=20), immunotherapy included nivolumab (N=4) and 5-FU (N=3), 3 patients received a combination of agents. The median interval between the two RT courses was 14 months (range=5-267 months).
Compliance with Ethical Standards. All procedures were performed in accordance with the ethical standards of the University Hospital of Muenster, of the national research committee, of the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Statistical analysis. All our statistical analyses were conducted with SPSS version 27.0 software (IBM, Armonk, NY, USA). We considered differences statistically significant at a p-value of <0.05. Chi-squared or Fisher exact tests were used to examine the relationships between two categorical variables. OS was measured from the relapse date until death, and PFS was calculated from the relapse date until relapse or death, whichever occurred first. LRC was calculated from the relapse date until locoregional progress or recurrence. If progression or death did not occur before the cut-off-date, data were censored at the time of last seen. Time-dependent event curves were calculated using the Kaplan Meier method. Comparisons were made using the log-rank test.
Results
Patient and disease characteristics. Critical clinical characteristics of the study cohort are summarized in Table I, including tumor classification, grading of the carcinoma, tumor localization, operation, RT and systemic treatment parameters for the primary and recurrence therapy, relapses after salvage treatment, metastases, and vital state.
Patient and treatment characteristics.
At the time of the final analysis, 41 patients had died, and 11 were alive. The median age of this cohort at the time of diagnosis of the primary tumor was 58 years (range=0-83 years), the majority of patients was male (N=40, 77%). Regarding initial tumor stage, five patients (9%) were classified as T1, 13 patients (25%) as T2, 15 patients as T3 (29%), and 17 patients (33%) as T4 disease, according to the TNM classification systems (8th edition). The nodal status of 37 (71%) patients was positive. Thirty patients (58%) had a low-grade tumor, while 13 patients (25%) were diagnosed with a high-grade carcinoma. Out of this cohort, 27 patients (52%) received primary surgery. The most common primary tumor site was oropharyngeal in 26 patients (50%). Forty-six patients (89%) initially underwent radiotherapy, while 37 patients (71%) received primary radiochemotherapy. The medium radiation dose was 70.2 Gy (range=16-73 Gy), and the medium fraction dose was 1.8 (range=1.5-2). Thirty-nine patients (75%) developed early relapse (≤24 months after primary therapy). For the relapsed carcinoma, eleven patients (21%) received salvage surgery, 45 patients (86.5%) underwent salvage radiation, and 44 patients (85%) had salvage radiochemotherapy. The medium salvage radiation dose was 45 Gy (range=27-72 Gy), and the medium fraction dose was 1.8 (range=1.8-2). The medium cumulative dose was 107 Gy (range=53-150 Gy). Medium follow-up after salvage RT was 19 months (range=2-65 months). The recurrent carcinoma was located within the primary radiation area in 23 patients (44%), marginal to the primary tumor site in 7 patients (13%), outfield in 3 patients (6%). The remaining patients (37%) did not receive prior radiation, or their relapse pattern was unknown. Distant metastases were recorded in 28 patients (54%), most commonly in the lung (N=20), liver (N=5), brain (N=2), bones (N=3), and mediastinal (N=5). A recurrence after salvage treatment was recorded in 20 patients (38.5%). Most commonly, these second relapses were treated with cetuximab (N=7) or nivolumab (N=5).
Outcomes
Overall and progression-free survival rates. Following relapse, the median OS was 16 months (95%CI=11-20), and median PFS was ten months (95%CI=8-12). Thus, one-year OS and 1-year PFS were 59±7% and 38±7%, respectively. We could not observe any difference in OS regarding histological grade (p=0.7). Regarding primary T-classification, patients with early-stage (T1-T2) had a trend towards more prolonged survival. Early-stage patients had a median OS of 21 months vs. 13 months for late stages (p=0.1). Similarly, regarding tumor stages, there was a trend towards longer OS in patients with early-stage disease vs. advanced stages (21 months vs. 14 months, p=0.1). Nodal status (p=0.3) or distant metastases (p=0.4) were not associated with a significant difference in OS. Patients who underwent surgery as part of the primary treatment strategy had a significantly longer OS than patients without surgery (21 months vs. 11 months, p=0.04, Figure 2). Similarly, patients who received surgery as part of salvage treatment tended to have longer OS (36 months vs. 13 months, p=0.09). There was no significant impact of salvage radiotherapy (p=0.3) or chemotherapy (p=0.9) on OS. There was a significantly higher OS in sub-group analysis for patients treated with platin-based therapy than cetuximab (p<0.01). We could not observe a difference between platin-based therapy or nivolumab (p=0.2). We detected a significantly higher OS in younger patients (<58 years) compared to older patients (p<0.01, Figure 3). Female patients had a longer OS (p=0.04). Patients suffering from a relapse after salvage treatments compared to the other patients had a median OS of 22 months vs. 10 months (p=0.1). The time interval between first diagnosis and relapse did not have a significant impact on OS (p=0.6; Figure 4).
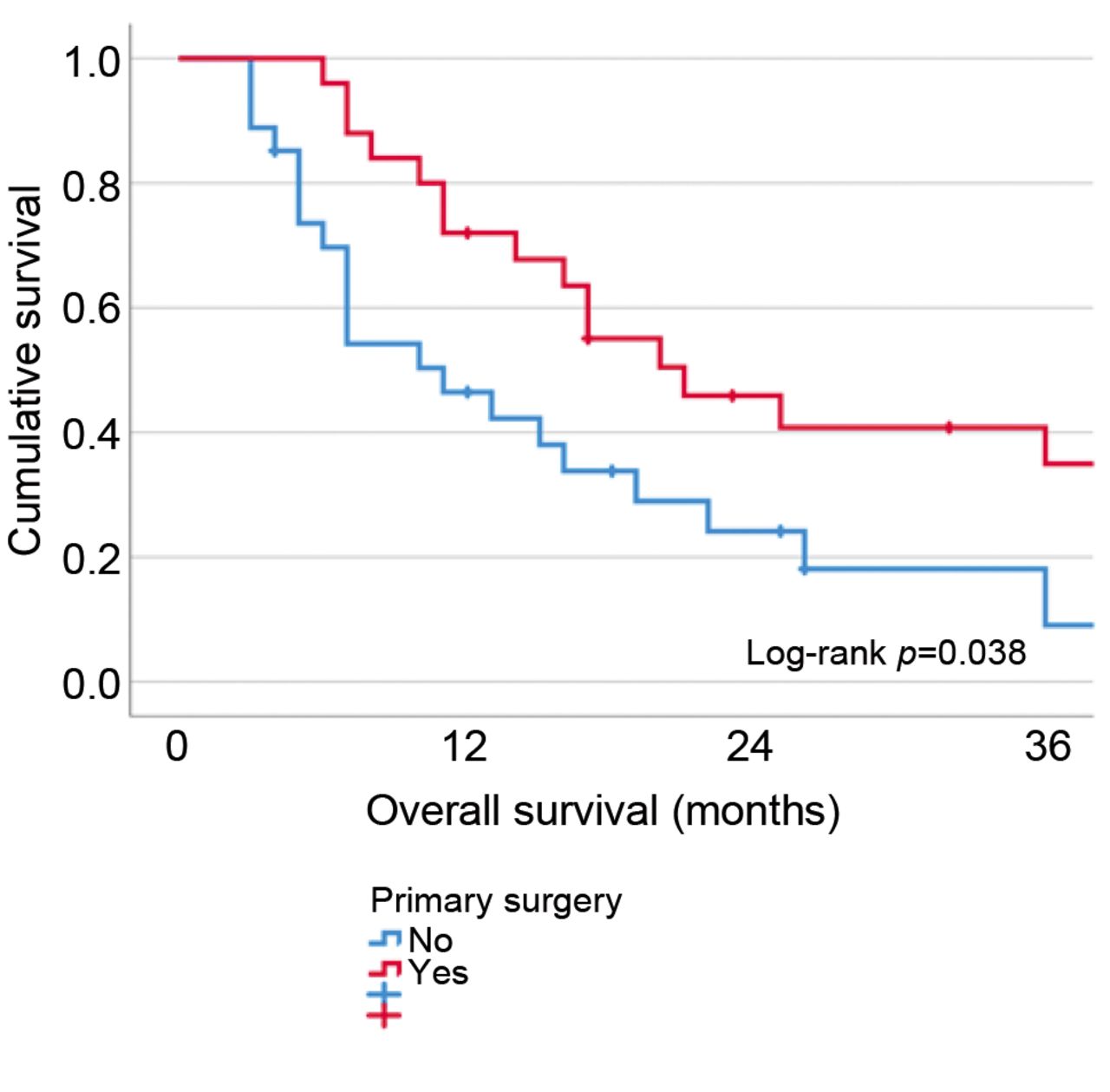
Kaplan–Meier estimates of overall survival according to primary surgery.

Kaplan–Meier estimates of overall survival according to age group (N=52).

Kaplan–Meier estimates of overall survival according to relapse interval (N=52).
There was no significant difference in PFS regarding histological grade (p=0.3), primary T classification (p=0.4) or nodal status (p=0.2). A trend for longer PFS could be detected for patients without distant metastases (p=0.06). Patients who experienced surgery as part of the primary treatment strategy had a significantly longer PFS than patients without surgery (14 months vs. 7 months, p=0.03). Similarly, patients who received surgery as part of salvage treatment had a significantly longer PFS (17 months vs. 9 months, p=0.03). PFS showed no significant difference between early or late relapses (p=0.5). There was no significant impact of RT (p=0.1) or chemotherapy (p=0.9) on PFS regarding salvage therapies. Comparing the chemotherapy agents, a significantly longer PFS for patients treated with cisplatin compared to cetuximab could be found (p=0.004). There was no noticeable difference between cisplatin and nivolumab (p=0.7). We detected a significantly higher PFS in younger patients compared to older patients (p=0.03). Female patients had a non-significant difference in PFS (p=0.2) compared to male patients.
Loco-regional control. Local relapses of the recurrent HNSCC were detected in 20 patients (38%). Distant metastases occurred in 28 patients (54%). Thirteen patients (24%) had both. For the whole cohort, the median LRC was 19 months (95%CI=12-26). The 1-year LRC was 65±8%.
In our cohort, no significant difference in LRC regarding histological grade (p=0.2), primary T classification (p=0.8), or nodal status (p=0.9) was detected. Regarding distant metastases (p=0.09), there was a trend towards longer LRC without metastases. We could not detect a significant impact of primary or salvage surgery on LRC (p=0.3). Patients who received surgery as part of salvage treatment had a longer LRC (41 months vs. 27 months, p=0.3). The application of primary RT showed a trend towards a shorter LRC (p=0.1). Regarding salvage therapies, there was no significant impact of RT (p=0.1) or chemotherapy (p=0.7) on LRC. Salvage radiation dose (p=0.02) and RT cumulative dose (p=0.004) showed a significant impact on LRC. Patients with early relapses compared to late relapses had a non-significant shorter LRC (p=0.6). Platin-based chemotherapy treatment showed a trend towards longer LRC compared to cetuximab (p=0.14). Nivolumab therapy had no significant difference compared to platin-based treatment (p=0.6). There was neither a difference in LRC between younger and older patients (p=0.8) nor did sex account for a significant difference in LRC (p=0.5).
Cox proportional hazards model. In a Cox proportional hazard model, age, sex, stage of disease, grade, surgical intervention, time interval till relapse, RT dose of salvage treatment, cumulative dose, and use of chemotherapy were included (Table II).
Univariate and multivariate analyses for locoregional control (LRC), progression-free survival (PFS), and overall survival (OS) (N=52).
In the univariate analyses, several parameters emerged as potential predictors of survivals. In the follow-up multivariate analysis, a higher salvage RT dose was associated with better LRC. RT cumulative dose was associated with PFS, while age and surgeries were found to be significant determinates of OS.
Toxicities. During salvage RT courses, most patients (85%) experienced adverse events (AEs). Twenty-two patients (44%) developed grade 1 AEs and 13 patients (25%) experienced grade 2 AEs. Grade 3 and 4 toxicities were observed in 9 patients (17%) and one (2%), respectively. No radiation-related deaths occurred, but two radiation-related breaks took place. The most common acute AEs were erythema and mucositis.
Regarding radiation dose, patients receiving a cumulative high-dose (>107 Gy) did not have more severe toxicities than patients with lower doses. Severe toxicities (grade 3 and 4) were not observed in patients receiving outfield radiation (N=3) as salvage therapy. Patients with infield radiation (N=22) developed grade 3 in 13% and grade 4 in 4% of cases.
Regarding salvage chemotherapy, seven patients (13%) changed the chemotherapy-agent or received a dose reduction due to side effects such as leukopenia (N=2), nephrotoxicity (N=2), or strong emesis (N=1).
Discussion
This analysis aimed to compare the impact of different combinations of RT, surgery, and chemotherapy strategies on LRC, PFS, OS, and radiation-related toxicity in recurrent HNSCC. From this work, several findings have emerged. Firstly, surgery treatment, especially primary surgery, significantly influenced OS and PFS of patients treated with recurrent HNSCC (p=0.05, p=0.04). Corresponding to this, patients who could not be treated with surgery in the first place but received primary radiation had a lower PFS and OS (p=0.04, p=0.03). Tumors with a locally advanced stage and inoperable tumors are considered for primary radiation and have a worse outcome (19, 20). Therefore, primary surgery is regarded as the standard treatment for HNSCC (21). It was shown that patients’ prognoses were better if surgery was conducted shortly after diagnosis (22). In accordance with several studies (23-26), our results also show that salvage surgery remains the preferred treatment for recurrent HNSCC with the best efficacy.
Secondly, age was shown to have a significant impact on OS. In multivariate analysis, this benefit remained a significant predictor for OS. Younger patients have better outcomes probably due to better general health status, better tolerance of aggressive treatment, and fewer comorbidities. With an increase in age, the effects of chemotherapy decrease (12). Chang and colleagues also regard age as a critical prognostic factor (23).
Concerning the systemic agents, cetuximab presented a disadvantage as a salvage agent compared to platin-based therapy over PFS and OS. In contrast to our findings, cetuximab is still often used as an agent for salvage treatment of HNSCC and has shown efficiency in other studies (11, 27). It is currently used in addition to cisplatin and 5-FU as first-line treatment for recurrent or metastatic HNSCC (28). Similar to our finding, Shapiro et al., Gillison et al., and Mehanna et al. have shown inferior outcomes for patients treated with cetuximab (29-32).
Re-irradiation as salvage treatment was used very carefully in the past due to increased risks of severe toxicities and showed unsatisfactory results in long-term control for conventional RT (33, 34). With image-guided RT and modern RT techniques, radio-related toxicities and deaths could be reduced (35, 36). However, only limited data serve as a guideline for re-irradiation of recurrent HNSCC (37).
In our analysis, IMRT with higher cumulative radiation dose impacted PFS in the multivariate analysis. While salvage radiation dose was associated with LRC. In accordance with our patients’ selection criteria, Strojan et al. also regard current comorbidities and the preexistence of organic dysfunction as important factors (38).
In accordance with previous studies (39, 40), sex seemed to impact OS of patients with recurrent HNSCC. Interestingly, characteristics of the primary tumor such as stage and grading, usually regarded as critical predictive factors for the primary tumor (41, 42), did not seem to impact LRC, OS, and PFS for the relapsed carcinoma.
Similar to previous studies (43), locoregional recurrence and salvage radiation mainly occurred infield in our patients. This could result in more adverse events due to higher amounts of cumulative radiation dose. IMRT, used for all patients’ salvage radiation, decreases toxicities and allows higher RT doses than conventional RT (44, 45). Our results indicated that higher radiation dose resulted in better local control and not necessarily in higher toxicity rates, although there was a slight trend towards higher grade AEs with infield radiation. However, as salvage RT significantly increased LRC with minimal grade 3 (13%) and grade 4 (4%), salvage radiation could be recommended. Still, individual factors such as health conditions seem to play an essential role in toxicities and should be evaluated before applying re-irradiation (46).
However, our study has several limitations due to its’ retrospective approach, relatively small number of patients, and diversity of characteristics and treatments, attributable to the relatively low frequency of recurrent HNSCC. Unfortunately, we could only include a few cases of patients treated with nivolumab, and some patient data were missing. Especially regarding treatment with nivolumab, ongoing prospective multi-institutional studies address this agent as a treatment option. Several studies have already found promising effects of nivolumab (47, 48). Therefore, immunotherapy might be considered in heavily pretreated patients.
Conclusion
Salvage treatment of HNSCC remains an interdisciplinary challenge. Although survival has already improved and significant advances in modern imaging and immunotherapy have been made, the need for more curative and less toxic treatment regimens remains an important issue.
Comparing the different treatment strategies, surgery remains the most effective primary and salvage therapy. In combination with high doses of salvage IMRT for better LRC and systemic therapy, survival could be increased. Platin-based therapy was superior to cetuximab in our analysis, and nivolumab could be a promising treatment option.
Footnotes
Author’s Contributions
Conceptualization, P.A.H., K.E., A.B. and H.T.E.; data curation, P.A.H.; formal analysis, P.A.H.; methodology, P.A.H, K.E., H.B., D.H., C.K., J.K., G.E., and E.W; writing – original draft, P.A.H. All Authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
There are no conflicts of interest related to this study.
- Received December 26, 2022.
- Revision received January 23, 2023.
- Accepted February 1, 2023.
- Copyright © 2023 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.