


Abstract
Prostate cancer (PCa) is among the most frequent cancers worldwide. Nowadays, several therapeutic strategies are available for PCa treatment, namely chemotherapy, immunotherapy, radiotherapy, and hormonal therapy. Despite existing therapeutic approaches, in vitro and in vivo models are essential to better understand cancer development and search for more effective therapies, with a positive impact in cancer patient survival and quality of life. Among several models available, the rat model is the one most frequently used, since it shares anatomical, physiological, pathological, and behavioral features with humans. Animal models can be classified as: spontaneous, chemically-induced; hormonally-induced; implantation of cancer cell lines obtained from humans or from the same species, in the place of disease development or in a different place; and genetically-modified models. The chemically-induced models are among the most frequently used for PCa research. This manuscript provides a comprehensive overview of PCa models, presenting their application, advantages, and disadvantages, and their importance for the development of current therapies for prostate cancer.
Prostate cancer (PCa) is among the most common cancers in men. In 2020, PCa was the third most diagnosed neoplasia, with 1,414,259 new cases (7.3% of all cancer cases) and 375,304 deaths (1).
During the last decades, PCa therapy has seen a remarkable evolution in many sectors, namely chemotherapy, immunotherapy, radiotherapy, and hormonal therapy. New precision medicine strategies and treatments are also suffering massive developments nowadays, also for PCa management, namely new proteomic and genomic technologies, non-coding RNA therapeutics or gene editing technologies (2).
Over the decades, different animal and non-animal models have been used to describe PCa morphologically, evaluate its development, set up prognostics, and develop more successful and globally used treatments.
This work aimed to review the different models used in PCa research among the decades and highlight their significant contribution to the discovery of various therapies regularly used nowadays to treat men with PCa and significantly improve their lives.
Prostate Cancer: An Overview
PCa is a neoplasia that results from the uncontrolled growth of the prostatic gland cells. Almost all PCas are adenocarcinomas. However, histologically, two types can be considered: acinar adenocarcinoma and non-acinar carcinoma. PCa acinar adenocarcinomas include atrophic, colloid, pseudohyperplastic, signet ring, and oncocytic carcinomas, among others. Non-acinar carcinoma only includes 5-10% of PCas, as the ductal adenocarcinoma, urothelial carcinoma, sarcomatoid carcinoma, squamous, basal cell carcinoma, or the small-cell carcinoma (3).
PCa is usually asymptomatic at the early stages with an average age of diagnosis at 66 years old. The most reported symptoms include dysuria, pollakiuria, and nocturia, which also occur in patients with prostatic hypertrophy. At an advanced stage, urinary retention is common, as well as back pain, since the axis skeleton is the most usual site of metastasis (4). Detection of elevated levels of prostate-specific antigen (PSA >4 ng/ml) is the first suspicion for the presence of PCa. However, tissue biopsy is necessary to confirm the diagnosis, since PSA levels may be found elevated in men with normal prostate (4). The growing incidence of PCa can be attributed to the increased awareness of PCa and routine use of the PSA analysis (5). It was found that a single PSA measurement between 44 and 50 years-old could predict PCa up to 25 years later (6).
Risk factors of PCa have been widely studied and discussed over the last decades. The factors most frequently mentioned are age, ethnicity, genetic, inflammation and infection, lifestyle, and androgen-related (5). The incidence of PCa is variable between countries and ethnic groups: in Asia (India, China, and Japan), the annual incidence is 1.9 new cases per 100,000 people. In the US, it is 161 per 100,000. However, if only the African American ethnicity is considered, this number rises to 272 new cases per 100,000 people. Hereditary PCa represents 43% of all men that had PCa before 55 years-old (7). PCa is also related to prostatitis (odds ratio=1.6) and the presence of sexually transmitted diseases (relative risk=1.4), like gonorrhea, syphilis, and human papillomavirus (5, 8). Even though others did not confirm this hypothesis, and one study demonstrated that high serum testosterone levels in men increased the risk of PCa (5).
What Constitutes a Disease Model?
Models of disease display some of the pathological processes observed in both humans and animals. They are essential for understanding how the disease develops, evaluate new diagnostic tools and testing potential treatments (9).
Animal models have been used in biomedical research with a perspective of comparative medicine, since the foundation of anatomy and physiology, in ancient Greece, more than 2,000 years ago (10). Animal species share anatomical, physiological, pathological, and behavioral features with humans. Mice and rats are the most commonly used species, representing approximately 95% of all animals used in laboratory research (11). Animal models of disease can be classified according to the mode of action: the spontaneous models (those that spontaneously develop the disease to be studied), genetically-engineered models (basically a mutant, i.e., a natural organism with a genetic alteration), the induced model (when a condition is experimentally induced through exposition to biological, physical or chemical agents); the implantation of cell lines (xenograft when cells are derived from a different species, syngeneic when the cells are derived from an animal genetically similar, orthotopic in which the cells are implanted in the place of origin of the neoplasia, or heterotopic when the cells are implanted in a place different from origin, like subcutaneous, intraperitoneal or intramuscular); the negative model (when studied condition/agent is innocuous to the model); and the orphan model (when the situation has not yet been described in humans) (12–14). Moreover, models can also be categorized regarding their genetics (inbred or outbred), as well as their microecology (gnotobiotic, germ free, specific germ free, or conventional) (15, 16).
Other disease models are becoming popular in clinical research, providing an alternative to animal models in scientific projects. The 3 R’s principle (Reduction, Replacement and Refinement) launched in the early 1960s by Russel and Burch have encouraged the substitution of mammals by simpler organisms (as invertebrates) or even non-living organisms. These alternatives include cell cultures and ex vivo models, such as computer modelling (17, 18).
A variety of in vitro cell lines, tissues or even organ cultures (3D models, organ-on-a-chip models) are available to study different conditions. This involves growth of cells outside the body in a controlled environment. Cells and tissues (from skin, liver, brain etc.) that are obtained from a donor and can be kept for a few days to a few years. In general, such research techniques are easy to perform and inexpensive. They are widely used in preliminary drug or cosmetic screening to test for potential toxicity and efficacy as, for instance, in eye irritancy tests (18). When compared with 2D models, the 3D cell culture model allows a better cell-cell and cell-extracellular matrix interaction, mimicking the complexity of tumor architecture and physiology. These 3D models are promising tools for PCa diagnosis, and drug discovery (19). Organ-on-chip model arose as a great technological advance, reforming biomedical research and drug discovery, by mimicking the structure and functionality of organs in vitro. Regarding oncology research, organ-on-a-chip is able to replicate key aspects of the tumor microenvironment, like biochemical gradients and niche factors, cell–cell and cell–matrix interactions, and complex tissue structures composed of tumor and stromal cells (20).
Computer modelling is widely used in certain medical areas, such as epidemiology. In this case, they help predict and characterize an infectious agent’s behavior in a population, becoming crucial to decide possible mitigation strategies or vaccination policies (21). Moreover, such models can help understand biology responses based on recognized principles and patterns. For instance, they can help predict possible biological or toxic effects of a drug candidate as primary screening, before in vivo experimentation, helping reduce and refine animal experimentation (18).
Which Models Are Available for Studying Prostate Cancer?
According to the World Health Organization (WHO), cancer is a leading cause of death worldwide, accounting for nearly one in six deaths, with a total of approximately 10 million deaths in 2020 (22). Considering this, and the great diversity of cancers, in terms of their location, histological type, progression, and response to therapy, researchers and funding agencies are continuously investing in projects for cancer research, looking for strategies towards an early diagnosis and better treatment, with a positive impact in the quality of life and survival of cancer patients.
In vitro and in vivo models. Several in vitro assays using cell lines have been formulated to study this PCa. Although this model allows understanding of several biological features of the disease, it is not able to mimic the complex cell–to–cell interactions occurring in the tumor microenvironment. To overtake this limitation, scientists were forced to develop animal models of PCa. Moore and Melchionna were pioneers in this field, with the induction of prostate carcinoma in the anterior lobe of prostate of rats, in 1937, through injection of 1:2 benzpyrene into prostate (23). This model was not able to develop metastasis, which constituted a limitation, and lead researchers to the development of other in vivo models of PCa. In 1945, Dunning et al. (24) induced the development of PCa able to metastasize in Fisher and Irish AxC 9935 rats, trough implantation of methylcholanthrene crystal into the prostate. Since the development of the first models of PCa, and with the discovery of chemical carcinogens with tropism for prostate, other models were arising. Some examples of these carcinogens are the N-nitrosobis (2-oxopropyl) amine (BOP) discovered by Pour in 1981 (25), the N-methyl-N-nitrosourea (MNU) discovered by Pollard in 1986 (26), the 3,2′-dimethyl-4-aminobiphenyl (DMAB) discovered by Katayama in 1986 (27) and the 2-amino-1-methyl-6-phe-nylimidazol[4,5-b]pyridine (PhiP) discovered by Shirai in 1997 (28). Beyond these, other chemical or natural agents may be used for the chemical induction of PCa development, namely: dehydroepiandrosterone (DHEA), cadmium, celecoxib (29), cholesterol, fluasterone, flutamide, lycopene, pioglitazone, pomegranate, quercetin, selenium, vitamin E, and zinc (30). These induced models are easy to obtain and allow to assess the effects of natural biological and synthetic agents.
Although the rat model of PCa may mimic human male prostate tumors, and they are able to metastasize to bones, it is worth noting that there are several differences in prostate anatomy between these species that should not be neglected. The human male prostate is a non-lobulated gland, appearing as a compact solitary structure below the bladder in front of rectum, like dogs’ prostate. Differently, the rat prostate consists of four distinct lobes, named according to their relative position to urinary bladder as: ventral, lateral, dorsal, and anterior lobes (26, 31). The lobes are morphologically different, and some authors consider only dorsal and lateral lobes homologous to human prostate (32). Despite these anatomical disparities, humans and rats present many similarities in the molecular mechanisms underlying PCa development, validating the rat as a model for PCa study. A proper rat model of PCa should be able to develop androgen-dependent adenocarcinomas within a short latency period, mimic the physiology and characteristics of man tumors, and the tumors must metastasize, preferably to bones (33).
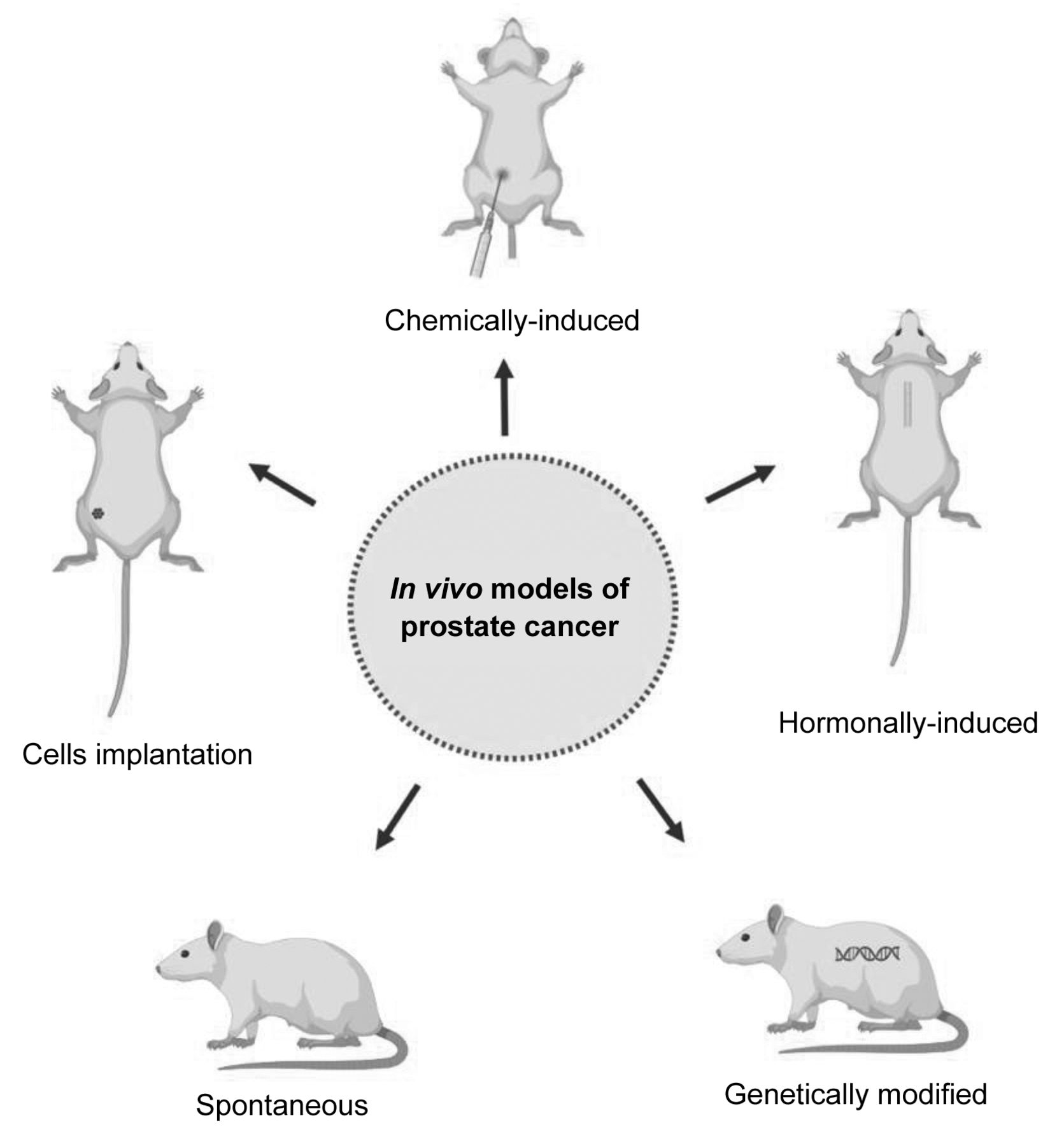
Nowadays, several animal models are available for PCa study, namely spontaneous models, chemically-induced, hormonally-induced, implanted, and genetically-modified (34, 35) (Figure 1).

In vivo models available for prostate cancer. Spontaneous models develop prostate cancer spontaneously; chemically-induced models are obtained through administration of chemical carcinogens, like N-methyl-N-nitrosourea, 3,2′-dimethyl-4-aminobiphenyl, 2-amino-1-methyl-6-phenylimidazol[4,5-b]pyridine and N-nitrosobis (2-oxopropyl) amine; hormonally-induced models are obtained through administration of hormones, like testosterone; implanted models can be obtained through implantation of cancer cell lines obtained from humans (xenograft model) or from the same species (syngeneic), in the prostate (orthotopic) or in a different place (heterotopic); and genetically-modified models results from genetic alterations.
The spontaneous models of PCa present a long period of latency (nearly 2-3 years) and a low incidence, being not advantageous for the study of this condition. The first spontaneous PCa tumor was reported by Dunning in 1963 in a 22 months-old Copenhagen rat (36–38). Ten years later, in 1973, Pollard described a spontaneous prostatic carcinoma in 26 months-old Wistar rats (37). In 1957 were described spontaneous tumors of ventral prostate in 34-37 months-old AxC rats (38). Moreover to these rat strains, aged ACI/Seg rats have a high susceptibility to develop spontaneous tumors in ventral prostate lobe (39).
The development of PCa may be induced though administration of chemical carcinogens, being the MNU, 3,2′-dimethyl-4-aminobiphenyl (DMBA), PhiP and BOP the most used. MNU is a direct alkylating agent, frequently used to induce the development of cancer in several organs, including prostate and the mammary gland. MNU may be used in combination with hormones to induce PCa development. Our research team has successfully used a rat model of PCa that was chemically and hormonally-induced in 12 weeks-old Wistar rats as follows: the anti-androgenic drug flutamide (50 mg/kg) was administered subcutaneously for 21 consecutive days; twenty-four hours later the testosterone propionate (100 mg/kg) was dissolved in corn oil and administered subcutaneously; two days later the MNU (30 mg/kg) was intraperitoneally injected; and two weeks later the implants filled with crystalline testosterone were implanted in the interscapular region of animals under anesthesia (30, 40–42). DMBA is an indirect carcinogenic agent that needs to be activated in the liver. Its metabolites interact with DNA inducing irreversible changes in DNA (43). DMBA is able to induce the development of carcinomas in ventral prostate lobe through a subcutaneous injection (27). PhiP is a heterocyclic amine whose active metabolites form DNA adducts, inducing development of cancer in prostate, mammary gland, and intestine (44–46). It can be administered in the diet or administered by gavage (47, 48). BOP is a nitrosamine with tropism to several organs, like pancreas, liver, and prostate (49). After its oral administration, BOP is converted into carbon dioxide that acts as a DNA methylating agent. The BOP has only the ability to induce the development of squamous cell carcinomas in ventral prostate lobes, that have no correspondence with human prostate, constituting a limitation of this model (33).
PCa can be also induced through administration of hormones, due to the sensitivity of prostate tissue to androgens. The implants filled with testosterone and estrogen may be subcutaneously implanted for a long period of time in rats. Simultaneously to the development of PCa, the animals may develop pituitary tumors leading to their early death (33).
The implanted models of PCa may be obtained through implantation of PCa cells obtained from humans (xenograft model) or from rat PCa (syngeneic model). The cell lines may be implanted in the rat prostate (orthotopic) or in a different place (heterotopic) (50–53). The xenograft models are immunodeficient, which did not allow the evaluation of the interplay between immune system and cancer. Genetically-engineered models are less time-consuming and labor-intensive when compared with chemically and hormonally-induced models. An incidence of 100% in guaranteed and tumors are androgen-sensitive (54).
At the current stage of knowledge, the advances in the study of PCa using 3D and organ-on-chip models have been small and need further research and increased funding.
Current Therapies for Prostate Cancer
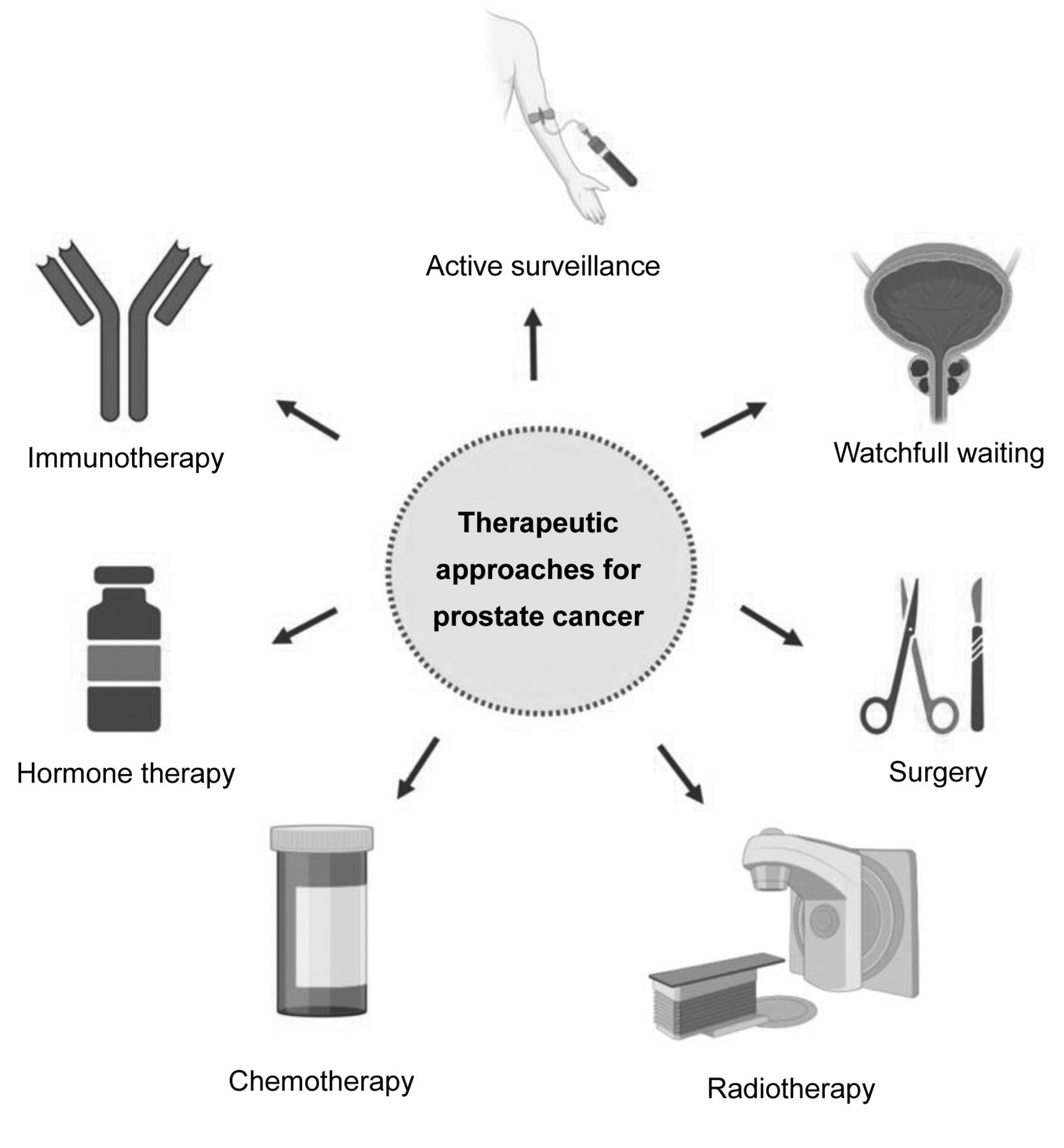
First, the stage of the disease and the patient’s profile must be clearly understood to choose the best treatment for each patient (55, 56). For this, it is important to have a good early diagnosis and assess the risk of the disease. After this, there exist a variety of approaches to be considered, which include active surveillance, watchful waiting, surgery, radiation, chemotherapy, hormone therapy and immunotherapy (55, 57) (Figure 2). All these approaches can be used alone or in combination.

Therapeutic approaches for prostate cancer.
Active surveillance consists of cancer monitoring through blood tests, PSA blood test and digital rectal exam. Moreover, prostate biopsies and imaging screening can be performed. This strategy is usually applied to patients with localized PCa and low risk of cancer growing or spreading outside of prostate. Watchful waiting is used in patients with low-risk and slow-growing disease, patients with other diseases and those with a limited life expectancy. Routine tests are not usually done on these patients (55, 57).
There are different surgical approaches, depending on the stage of the disease and patient status. Radical prostatectomy, by laparoscopic or robotic-assisted, removes entire prostate gland and seminal vesicles (58). Transurethral resection of the prostate is performed to remove the inner part of the prostate that surrounds the urethra relieving trouble urinating (59). Minimally invasive techniques, with minimal incisions or using tiny instruments into the urethra are increasingly used to treat PCa or relieve symptoms.
Radiation therapy in PCa include, for example, external beam radiation, brachytherapy or radiopharmaceuticals use. Radiopharmaceuticals is an emergent cancer therapy that deliver radiation therapy directly to cancer cells (60). Specifically in set of PCa, at the end of March 2022 the Food and Drug Administration (FDA) approved 177Lu-PSMA-617 to treat patients with metastatic PCa who have been treated with androgen receptor (AR) pathway inhibitors and taxane-based chemotherapy (61). This drug combines a targeting compound with a therapeutic radioisotope. After its administration binds to PCa cells that express prostate-specific membrane antigen (PSMA), a transmembrane protein and, once bound, emissions from the radioisotope damage tumor cells disrupting their capacity to replicate and triggering cell death (62–64).
Hormonotherapy is one of the most advanced areas where new drugs have been developed, such as apalutamide and darolutamide. Apalutamide, an androgen signaling inhibitor, has been studied and was approved by FDA in 2018 and by European Medicine Agency (EMA) in 2019 (65–67). It is used to treat non-metastatic castration-resistant prostate cancer (CRPCa) and metastatic hormone-sensitive PCa in combination with androgen deprivation therapy (65). Darolutamide is an androgen-receptor inhibitor used in the treatment of non-metastatic CRPCa in combination with surgery or medical castration approved in USA in 2019 and in the European Union in 2020 (68–71).
Another emerging therapy for PCa is called focal irreversible electroporation. This technology uses low voltage direct electric current that permanently damages the cell membrane and leads to cell death, preserving the surrounding prostate structures (72–74). Tissue selectivity, reduced toxicity on vital anatomical structures surrounding the prostate lesions, and preservation of urinary and sexual functions are the main advantages of this technique (75). Moreover, this technique is minimally invasive in contrast with other therapies, allow precision in targeting cancerous cells and the recovery time is short (74, 76). However, this technique is still at an early stage of development and there are still not many scientific studies comparing it with more traditional approaches, but the results seem promising (74, 77–79).
Immunotherapy is a promising PCa therapy that uses patients’ own immune system to recognize and kill cancer cells. Sipuleucel-T, a cell-based vaccine, is the only FDA approved immunotherapy for asymptomatic or minimally symptomatic metastatic CRPCa (80, 81). However, it is not yet available in Europe (82, 83). The treatment involves the use of patient’s immune cells stimulated to target the antigen prostatic acid phosphatase (80). Other vaccine therapies are being tested in clinical trials, such as Prostvac (84). Immune checkpoint inhibitors are another type of immunotherapy that block checkpoint proteins from binding with their partner proteins, allowing the immune system, namely T cells, to attack and kill the cancer cells. Pembrolizumab is a drug that targets PD-1/PD-L1 pathway and is the only FDA approved for advanced PCa that has high microsatellite instability, DNA mismatch repair deficiency or high tumor mutational burden (85–87). There are more ongoing studies and clinical trials with these immune checkpoint inhibitors drugs but whose results still do not allow their approval by the competent authorities and their commercialization (88–91).
Animal models have been vital for discovery, development, and approval of novel drugs for cancer treatment, by allowing to evaluate their safety, toxicity, pharmacodynamics, pharmacokinetic and efficacy. Determining efficacy and safety is critical during the initial phases of drugs discovery and development, and ultimately for approval and commercialization. Some of the drugs approved by the FDA or EMA, and listed above, were tested in rodent models (92–102).
Conclusion
Models for any given assay should be carefully chosen by researchers whilst considering the aim of the study, the associated costs, and the advantages and disadvantages of each model. Although several models are available for PCa studies, rodent models remain the ones most used. Despite their disadvantages, rat models have provided a great deal of information concerning PCa biopathology, allowing better understanding of the disease as well as leading to the development of more effective therapies. The PCa hormone and chemically-induced model is very complex, time and labor-consuming, but it successfully induces development of PCa tumors hormone-dependent and histologically similar to those developed by men, allowing data translation. In the future, animal models will certainly continue to be a fundamental tool in the study of PCa and development of new therapeutic approaches, since only laboratory animals allow for the study of several variables simultaneously.
Acknowledgements
This work was supported by National Funds by FCT - Portuguese Foundation for Science and Technology, under the projects UIDB/04033/2020 and LA/P/0126/2020), and PhD grants SFRH/BD/136747/2018 (E. Nascimento-Gonçalves) and 2021.04520.BD (C. Jota-Baptista).
Footnotes
Authors’ Contributions
All Authors were responsible for manuscript writing and revision and approved its submission.
Conflicts of Interest
The Authors have no conflicts of interest to declare.
- Received November 14, 2022.
- Revision received November 26, 2022.
- Accepted December 9, 2022.
- Copyright © 2023 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).





{kind=link}
{kind=link}