


Abstract
Background/Aim: Flap endonuclease 1 (FEN1) is a critical protein in DNA repair, genomic stability, and carcinogenesis. Functional polymorphisms in FEN1 promoter −69G>A (rs174538) and 3′UTR 4150G>T (rs4246215), have been associated with the susceptibility to several cancers, including lung, breast, esophageal, gastric, liver, colorectal, and gallbladder cancer, as well as glioma, endometriosis, and leukemia. However, the contribution of FEN1 variant genotypes to oral cancer has never been examined. Thus, we aimed to evaluate the contribution of FEN1 rs174538 and rs4246215 genotypes to oral cancer risk in Taiwan. Materials and Methods: The contribution of FEN1 genotypes to oral cancer risk was examined in 958 oral cancer patients and 958 age- and sex-matched healthy controls by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). Results: The percentages of GG, AG, and AA genotypes at FEN1 rs174538 were 34.8%, 46.0%, and 19.2% among oral cancer patients and 37.8%, 45.2%, and 17.0% among healthy controls (p for trend=0.2788). The genotypic percentages of FEN1 rs4246215 were 35.9%, 45.9%, and 18.2% among oral cancer patients and 37.6%, 45.1%, and 17.3% among healthy controls (p for trend=0.7315). Overall, FEN1 rs174538 and rs4246215 were not differently distributed between the oral cancer patient and healthy control groups. The allele frequency analysis confirmed that FEN1 rs174538 and rs4246215 were non-differentially distributed among case and control groups (OR=1.11 and 1.05, 95%CI=0.98-1.27 and 0.93-1.20, p=0.1074 and 0.4491, respectively). Conclusion: FEN1 may contribute to oral cancer risk determination via protein expression and/or post-transcription modification, but may not be a practical genetic marker.
Oral cancer is the fourth most prevalent and the fourth death-causing cancer among males in Taiwan, where the incidence density of oral cancer is higher worldwide (1-3). In literature, several factors are revealed to contribute to the etiology of oral cancer in Taiwan, such as betel quid chewing, tobacco smoking, alcohol drinking, bad tooth brushing habits, and virus infection (4, 5). Interestingly, in recent years, specific inherited genotypes have been reported to contribute to personal oral cancer susceptibility (6-13). A better understanding of genomic, environmental and behavioral factors can contribute to precise and personalized oral cancer prediction and therapy.
The DNA repair machinery represents a network of proteins, which is responsible for detecting and removing DNA adducts, thereby maintaining the genomic integrity and preventing the transmission of inherited mutations to offspring cells. Among the DNA repair proteins, Flap endonuclease 1 (FEN1) is an endonuclease specifically responsible for repairing DNA damages induced by alkylating drugs and UV irradiation (14). FEN1 has been localized in the cell nucleus in a cell cycle-dependent manner, implicating FEN1 in both DNA replication and repair processes (15). In addition, FEN1 has been shown to accumulate in cell nucleolus, where it acted as the tandem repeated ribosomal DNA gatekeeper (16). Furthermore, FEN1 has been also found in mitochondria, indicating its critical role in maintaining mitochondrial DNA integrity (17). However, the functions and regulations of FEN1 are complicated that its activity can be regulated by multiple mechanisms including acetylation, phosphorylation and methylation. These post-translational modifications on FEN1 have been shown to regulate not only its nuclease activities, but also its selective binding to numerous protein partners (18-20). In addition to its role in DNA replication and repair, FEN1 could also act as inducer of DNA fragmentation during apoptosis (21, 22). Knockout of FEN1 can elevate microsatellite instability and promote cancer progression in mice (23). In human cancer cell models, FEN1 mutations reduced its nuclease activity, and resulted in chronic inflammation and cancers, especially lung cancer (24). Thus, genetic variations of FEN1 could be associated with an elevation risk for carcinogenesis.
Most studies of FEN1 genotypic variations have been focused on the two common sites, promoter −69G>A (rs174538) and 3′UTR 4150G>T (rs4246215), which have been found to alter both the levels of FEN1 and its enzyme activity (25). The FEN1 genotypes rs174538 and/or rs4246215 have been reported to associate with the risk of several cancers including esophageal (26, 27), lung (25), breast (28-30), gastrointestinal (27, 31), and gallbladder cancer (32), as well as glioma (33), endometriosis (34) and childhood leukemia (35). However, the associations of FEN1 genotypes with oral cancer have never been examined. Thus, the purpose of the present study was to identify the genotypic patterns of FEN1 promoter rs174538 and 3′UTR rs4246215 in a representative oral cancer population consisting of 958 cases and 958 controls, and to evaluate the association of these two FEN1 genotypes and oral cancer risk. The FEN1 polymorphic sites rs174538 and rs4246215 are shown in Figure 1.
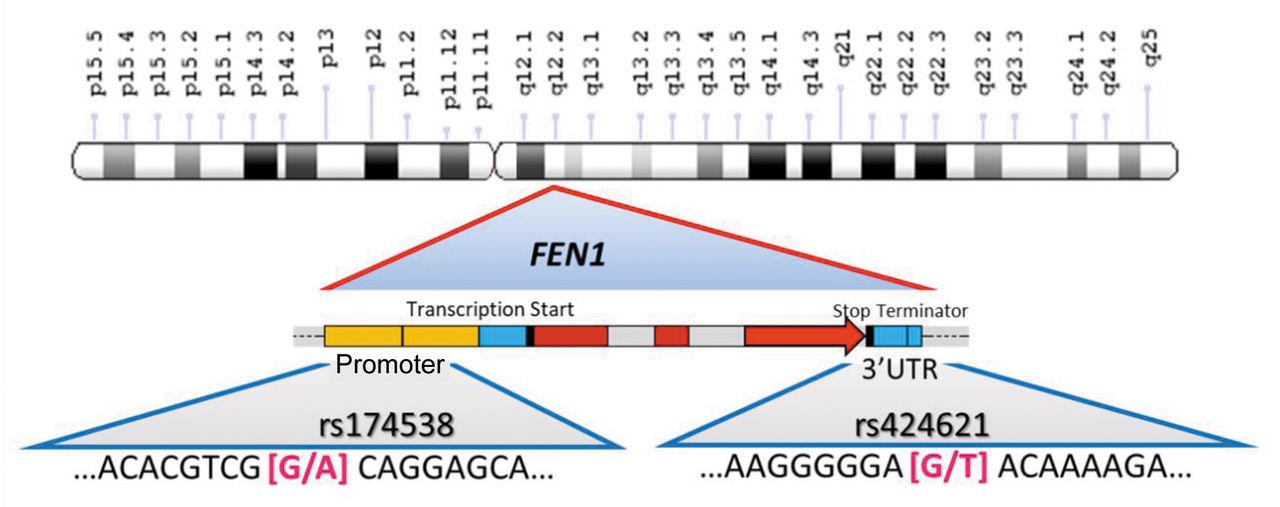
FEN1 polymorphic sites at the promoter rs174538, and 3′UTR rs4246215, in human chromosome 11.
Materials and Methods
Oral cancer cases recruiting methodology. Oral cancer cases were recruited in China Medical University Hospital by a group of surgeons. Patients with history of any malignancy, metastasized cancer from other (even those unknown) origins, any genetic inherited diseases (especially those with family history), or cancer-like diseases, such as pterygium and endometriosis, were all excluded. Finally, 958 cases agreed to sign an inform consent. All participants were Taiwanese. At the same time, 958 of healthy volunteers matched for age and sex from the Health Examination Cohort of China Medical University Hospital were selected as healthy controls. The study was approved by IRB of China Medical University Hospital (DMR101-IRB1-306). All protocols were conducted following the principles documented in the Helsinki Declaration. The detail sampling of the cases and controls has been published in our previous studies (12, 13). The demographics of participants are summarized in Table I.
Characteristics of 958 oral cancer patients and 958 healthy subjects.
FEN1 rs174538 and rs4246215 genotyping methodology. DNA was extracted applying QIAamp Blood Mini Kit (Blossom, Taipei, Taiwan, ROC) and further processed according to our previous studies (36-38). The sequences of primers for FEN1 rs174538 were: forward 5′-CCTAAGGAGTTCATGGCAAG-3′ and reverse 5′-AATCGCAGGACTACAAGTCC-3′. For FEN1 rs4246215, the sequences of primers were: forward 5′-GGTGGAGAGA GGATTCTAAG-3′ and reverse 5′-CATCTGCTAAGATGCGCCTT-3′. Following the polymerase chain reaction (PCR) processes, the PCR adducts for FEN1 rs174538 and rs4246215 were subject to the digestion with Sal I and BcoD I (New England BioLabs, Ipswich, MA, USA). As for FEN1 rs174538, the digestible A-allele adducts were cut into fragments of 223 and 84 base pairs, while the indigestible G-allele adducts were left as intact 307 base pairs. As for FEN1 rs4246215, the digestible G-allele adducts were cut into fragments of 234 and 148 base pairs, while the indigestible T-allele adducts were left as intact 382 base pairs.
Statistical analysis. To examine the representativeness, the percentages of FEN1 genotypes for the control group under Hardy-Weinberg Equilibrium were examined using the goodness-of-fit test. To compare the distribution of age between the two groups, the unpaired Student’s t-test was conducted. To compare the FEN1 rs174538 and rs4246215 genotypic distributions, Pearson’s Chi-square test was applied. The associations between FEN1 rs174538 and rs4246215 genotypes with oral cancer risk were estimated by odds ratios (ORs) and 95% confidence intervals (CIs). Trend analysis was performed using the chi-square test without Yates’ correction. Any analysis outcome with p<0.05 was considered statistically significant.
Results
Demographic data comparison between oral cancer patients and healthy controls. First, since we matched the case and control groups by age and sex there are no differences between the oral cancer case and control groups (p=0.3755 and 1.0000, respectively) (Table I, top panel). Second, there are more smokers (p=0.0107), alcohol drinkers (p=0.0377) and betel quid chewers (p=0.0001) in the oral cancer than in the control group, indicating that cigarette smoking, alcohol drinking and betel quid chewing behaviors are oral cancer risk factors in Taiwan (Table I, middle panel). Third, among Taiwanese oral cancer cases, the most common primary tumor sites were the tongue (41.4%) and buccal mucosa (37.2%) (Table I, bottom panel). As for oral cancer subtypes, 93.1% of the oral cancer patients belonged to the subtype of squamous cell carcinoma (Table I, bottom panel).
FEN1 rs174538 and rs4246215 genotypic comparison between oral cancer patients and healthy controls. First, the genotypic frequencies for FEN1 rs174538 in the control group fitted well under the Hardy–Weinberg equilibrium (p=0.0871). Second, there was no significant difference in the distribution of FEN1 rs174538 genotypes between the oral cancer and control groups (p for trend=0.2788). In detail, the frequencies of the wild-type GG, heterozygous variant AG and homozygous variant AA of FEN1 rs174538 were 37.8%, 45.2% and 17.0% in the healthy control group, and 34.8%, 46.0% and 19.2% in the oral cancer patient group. These results indicated that neither AG (OR=1.11, 95%CI=0.91-1.35, p=0.3419) nor AA (OR=1.23, 95%CI=0.95-1.59, p=0.1363) genotypes at FEN1 rs174538 can serve as a good marker for oral cancer early detection (Table II, top panel). In the recessive model, the AA genotype at FEN1 rs174538 was not associated with altered cancer risk, compared to GG+AG genotypes (OR=1.16, 95%CI=0.92-1.46, p=0.2354) (Table II, middle panel). In the dominant model, AG+AA genotypes at FEN1 rs174538 were not associated with altered oral cancer risk, compared to GG genotype (OR=1.14, 95%CI=0.95-1.37, p=0.1834) (Table II, bottom panel).
Distribution of FEN1 rs174538 genotypes among the oral cancer patients and healthy subjects.
Similarly, the FEN1 rs4246215 genotypic frequency was examined for its association with oral cancer in each model. However, no difference was found in either codominant, recessive or dominant models (Table III).
Distribution of FEN1 rs4246215 genotypes among the oral cancer patients and healthy subjects.
FEN1 rs174538 and rs4246215 genotypic comparison between oral cancer patients and healthy controls. To confirm these associations for FEN1 rs174538 and rs4246215 genotypes, the allelic frequency analysis was also performed. The results showed that neither the wild-type G allele nor variant A allele of FEN1 rs174538 was associated with an altered risk of oral cancer (OR=1.11, 95%CI=0.98-1.27, p=0.1074, Table IV, top panel). At the same time, neither the wild-type G allele nor variant T of FEN1 rs4246215 was associated with an altered risk for oral cancer (OR=1.05, 95%CI=0.93-1.20, p=0.4491, Table IV, bottom panel).
Distribution of FEN1 rs174538 and rs4246215 allelic frequencies among the oral cancer patients and healthy subjects.
Discussion
In the present study, we first examined the contribution of FEN1 genotypes to oral cancer susceptibility. FEN1 has been reported to exert multiple functions in DNA replication, DNA repair, cell cycle and programmed cell death, which made us to hypothesized that subtle genomic variations like SNPs may determine differential personal risk in oral cancer. The polymorphic FEN1 rs174538 and rs4246215 genotypes have been reported to differentially affect enzymatic activity and determine the rate of tumorigenesis (23, 24). However, our data showed that FEN1 rs174538 or rs4246215 genotype was not associated with altered susceptibility to oral cancer among Taiwanese (Table III). These findings are in conflict with studies showing that the A allele of FEN1 rs174538 can serve as a protective factor for the risk of lung (25), gastrointestinal (31), esophageal (27), and breast cancer (28), as well as glioma (33) and childhood leukemia (35). The inconstancy may suggest that the association of FEN1 genotypes with cancer susceptibility is cancer-specific, and population-dependent. The results of our study should be validated in other populations. To the best of our knowledge, the current study was the first to provide evidence that FEN1 rs174538 and rs4246215 are not associated with oral cancer risk (Table II and Table III).
It is of our interest to reveal the combinatorial effects of FEN1 rs174538 and rs4246215 genotypes with sex, age, and personal behaviors. First, the oral cancer prevalence among Taiwanese is of the highest in the world and the male versus female ratio is about 9 to 1 (39). We determined the distribution of FEN1 rs174538 and rs4246215 among oral cancer patients and controls according to the sex status and found that there was no significant difference in the distribution among oral cancer patients and controls (data not shown). Second, we also determined the distribution of FEN1 rs174538 and rs4246215 among oral cancer patients and controls with age less than 45 or larger than 45 and found that there was no significant difference in the distribution among oral cancer patients and controls (data not shown). Third, since betel quid chewing, smoking and alcohol drinking behaviors are the top three environmental contributors to oral cancer risk (40, 41), we also evaluated the combinatorial effects of the FEN1 rs174538 and rs4246215 genotypes and these personal behaviors on oral cancer susceptibility. There were no obvious combined effects of FEN1 genotypes with any of these risk-conferring behaviors (data not shown).
In summary, the current study provides solid evidence, in a representative population, that the FEN1 genotypes are not sensitive biomarkers for early detection of oral cancer in Taiwan. The contribution of FEN1 genotypes should be validated in different populations with different genetic background and lifestyle to understand the role of FEN1 in oral carcinogenesis.
Acknowledgements
The Authors are grateful to China Medical University Hospital Tissuebank and doctors/nurses for their help in sample collection and inform consent assistance. This study was supported mainly by China Medical University, Taichung, Taiwan and Asia University, Taichung, Taiwan (CMU111-ASIA-01) and Chang Bing Show Chwan Memorial Hospital, Changhua, Taiwan (BRD-109025).
Footnotes
↵* These Authors contributed equally to this study.
Authors’ Contributions
Research design was performed by PSH, CWT and JLH. Patient and questionnaire collections were conducted by LCS and CLH. Experimental work was performed by WCC, TCH, PSH and YCW. Statistical analysis was conducted by WCC, HYT and JLH. DTB and WSC wrote the manuscript, whereas DTB, CWS, and WSC reviewed it and were responsible for the revision.
Conflicts of Interest
The Authors declare no conflicts of interest with any company or individual.
- Received July 18, 2022.
- Revision received July 27, 2022.
- Accepted July 28, 2022.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).





{kind=link}