


Abstract
Background/Aim: Studies have indicated that liver mobilization during hepatectomy could cause the dissemination of tumor cells. However, the data are still limited in terms of the relationship between circulating tumor cells (CTCs) and surgical procedures. Patients and Methods: Fifteen patients who underwent hepatectomy for primary hepatocellular carcinoma (HCC) were included in the study. Blood samples were collected from the portal vein, central vein, and peripheral artery at three time points, namely, before mobilization (BM) of the liver, during transection (DT) of parenchyma, and after resection (AR) of the tumor. To detect CTCs, a real-time PCR assay was performed using primers for the epithelial cell adhesion molecule, cytokeratin 18, and glypican 3. Patients were divided into anterior approach (AA) and non-AA (NA) groups. In the AA group, patients underwent an initial hilar vascular dissection followed by a liver hanging maneuver during transection. Results: Seven patients were allocated to the AA group, and eight to the NA group. In the NA group, CTC levels in the portal vein were significantly increased at DT and AR compared to BM. In cases with large HCC (>70 mm), CTC levels in central venous blood were significantly increased at DT and AR in the NA group. Conclusion: The AA liver resection technique may minimize CTC dissemination, improving the prognosis of patients with HCC.
Hepatocellular carcinoma (HCC) is a major primary liver cancer (1, 2) that is often associated with poor prognosis due to the high incidence of recurrence and metastasis (3). Intrahepatic and distant metastases are thought to be caused by tumor cells seeded in the blood stream (4). Circulating tumor cells (CTCs) are defined as cells that detach from a primary cancer and enter the blood stream (5). The presence of CTCs is closely associated with poor prognosis in various types of cancers (6-8). In patients with HCC, a high preoperative CTC level is an independent prognostic factor for post-surgery recurrence. However, the relationship between the surgical procedure of hepatectomy and CTC level is still not well elucidated in the literature (9). Hematogenous dissemination of malignant tumor cells during surgical procedures has been reported for various types of cancers, and manipulation of the tumor could be the root cause (10-12). Similarly, it has been suggested that liver mobilization, as the current standard hepatectomy procedure for HCC, may cause dissemination of tumor cells from the primary lesion (13-16). However, some studies have reported that anterior approach (AA) resection technique without liver mobilization achieved better operative and survival outcomes compared to liver resection with liver mobilization (14, 17, 18). Therefore, the AA resection may have contributed to the decrease in hepatogenic dissemination of CTCs. In this study, we assessed the effects of surgical procedures on tumor cell dissemination during hepatectomy. The identified surgical procedures were: 1) liver mobilization (to reduce tumor cell dissemination), 2) upfront hilar vascular dissection (to prevent tumor cell dissemination), and 3) hanging maneuver (to prevent tumor manipulation). We evaluated the changes in CTC level during hepatectomy in the AA and the non-anterior approach (NA) groups. Three surgical procedures (liver mobilization, upfront hilar vascular dissection, and hanging maneuver), surgical factors, and tumor related factors were also analyzed individually.
Patients and Methods
Patients. From March 2017 to June 2018, 165 patients underwent hepatectomy at our hospital. Of these patients, 15 who underwent anatomical hepatectomy for primary HCC by laparotomy were included in this study. The following exclusion criteria were applied: 1) not diagnosed as HCC preoperatively, 2) partial liver resection, 3) laparoscopic liver resection, 4) treated with preoperative chemotherapy, and 5) recurrence of HCC (Figure 1). Written informed consent was obtained from all patients before enrollment. This study was performed in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) and approved by the ethics board of Kurume University Hospital (Approval number: 302).

Flow chart of the patient selection process. A total of 165 patients underwent hepatectomy at our hospital. Fifteen patients who underwent anatomical hepatectomy for primary hepatocellular carcinoma (HCC) by laparotomy were included in this study.
Specimen collection. Blood specimens from the portal vein, central vein, and peripheral artery were collected at three time-points, namely before liver mobilization (BM), during transection (DT) of parenchyma, and after resection (AR) of the tumor. All blood specimens were drawn into 2.5 ml PAXgene Blood RNA tubes (Becton, Dickinson and Company, Franklin Lakes, NJ, USA). Peripheral blood specimens were collected from an indwelling radial-artery catheter, which was used for intraoperative hemodynamic monitoring. Blood specimens from the central vein were collected from an internal jugular venous catheter, which was used for intraoperative fluid administration and central vein pressure monitoring, and the tip of the catheter was placed near the right atrium. Blood specimen from the portal vein were collected from the portal pressure monitoring catheter, which was inserted via the ileocolic vein and the tip of the catheter was placed proximal to the bifurcation of the right and left portal veins.
RNA extraction and real-time polymerase chain reaction (PCR). RNA extraction was performed using the PAXgene Blood RNA kit (QIAGEN, Hilden, Germany). After RNA was converted to complementary deoxyribonucleic acid (cDNA) using Super Script VI VILO Master mix (Thermo Fisher Scientific, Waltham, MA, USA), real-time PCR was performed using a TaqMan Gene Expression Assay in the StepOne Plus Real-Time PCR System (Thermo Fisher Scientific). Primers for epithelial cell adhesion molecule (EpCAM), cytokeratin 18 (CK18), and glypican 3 (GPC3) were used for the detection of CTCs. The probes used were EpCAM, Hs00158980_m1; CK18, Hs01941416_g1; GPC3, Hs01018936; and glyceraldehyde-3-phosphate dehydrogenase (GAPDH), Hs02758991_g1 (Thermo Fisher Scientific). The expression of the markers was normalized to GAPDH. The PCR assay consisted of an initial denaturation step at 95°C for 20 s, followed by 40 cycles of annealing and extension at 60°C for 20 s.
Surgical procedure for hepatectomy. After an incision was made, a portal pressure monitoring catheter was inserted to the portal vein via the ileocolic vein. Ultrasonic scalpel was used for liver parenchyma transection, and the Pringle maneuver was used to control hepatic blood flow.
Based on the surgical procedure, the patients were divided into the AA and NA groups. The following surgical procedures were performed in the AA group (1). Minimal liver mobilization: The liver was minimally mobilized during the transection of the liver parenchyma (2). Upfront hilar vascular dissection: Hilar vascular dissection was first performed to isolate and divide the hepatic artery and portal vein. The hepatic artery and portal vein were dissected individually or a Glissonean pedicle ligation was performed (3). Hanging maneuver: The suprahepatic inferior vena cava (IVC) was exposed and the space between the right and middle hepatic veins was dissected, and the retrohepatic space anterior to the IVC was established in a caudal to cranial direction. A tetron tape was passed through the tunnel anterior to the IVC and used for the liver hanging maneuver. If any of the above three steps were not performed, the patient was categorized as NA group.
Surgery was performed by two board-certified hepato-biliary-pancreatic surgeons, and one surgeon performed AA.
PCR analysis for CTC detection. Blood specimens collected from the peripheral artery, portal vein, and central vein for BM, were molecularly assessed for CTC levels using the PCR primers for EpCAM, GPC3, and CK18. Expression values for the three markers were then normalized to that of GAPDH, which was assigned as 1. Then, the percentages of the quantitative values of CTCs for DT and AR for each sample were calculated and compared to the value of BM.
Statistical analysis. We used t-tests to compare the averages of continuous variables and Chi-square tests to compare the proportions of categorical variables between the groups. Comparisons between the value of CTC for BM and DT or AR of each blood sampling site were performed using the Wilcoxon test. A p-value<0.05 was considered statistically significant. All statistical analyses were conducted using JMP 13 (SAS Institute Inc., Cary, NC, USA).
Results
Of the fifteen patients with HCC, six had right hepatectomy, two had left hepatectomy, three had posterior sectionectomy, one had anterior sectionectomy, two had central bisectionectomy and one had medial sectionectomy. There were seven and eight patients in the AA and NA groups, respectively.
Preoperative clinical characteristics, demographics, and surgery-associated factors are shown in Table I. Serum albumin levels were significantly elevated in the NA group (p<0.001); however, there were no significant differences in other preoperative liver function and tumor marker levels between the two groups. Additionally, there was no significant differences between the two groups for tumor or surgery-associated factors, namely Pringle time, tumor size, histology, and microscopic portal invasion.
Preoperative clinical findings, demographics, and surgery associated factors for anterior approach (AA) and non-anterior approach (NA) groups.
Changes in CTC level during hepatectomy
Portal vein blood. A comparison of the portal vein blood specimen between the AA and NA groups is shown in Figure 2A and B. In the NA group, the CTC levels were significantly increased for DT (p=0.001) and AR (p=0.001) compared to those for BM. The sub-analysis of three surgical procedures (upfront hilar vascular dissection, liver mobilization, and hanging maneuver) were also performed. In cases with liver mobilization, the CTC levels were significantly increased for DT (p=0.003) and AR (p<0.001). In the cases without hanging maneuver, the CTC levels were significantly increased for DT (p=0.037) and AR (p<0.001). In cases with or without hilar dissection, there was no significant change in CTC levels during hepatectomy. In cases with tumors >70 mm in diameter, the CTC levels were significantly increased for AR (p<0.001), and in cases with protein induced by vitamin K absence or antagonists-II (PIVKA-II) >1,000 mAU/ml CTC levels were significantly increased for DT (p=0.003) (Table II).

Changes in the levels of circulating tumor cells (CTCs) during hepatectomy in the AA and NA groups. (A) and (B): Changes in the levels of CTCs in the portal vein. In the anterior approach (AA) group, there was no significant change for DT and AR (A). In the non-anterior approach (NA) group, CTC levels were significantly increased for DT and AR compared to that for the BM (B). (B) and (C): Changes in the levels of CTCs in the central vein. There was no significant increase in CTCs for DT and AR in the AA and NA groups. (D) and (E): Changes in the levels of CTCs during hepatectomy in the central vein with tumor size over 70 mm. In the AA group, there was no significant increase in the CTC levels for DT and AR (D). The CTC levels were significantly increased for DT and AR in the NA group for patients with tumors >70 mm in diameter (E). BM: Before liver mobilization; DT: during parenchymal transection; AR: after liver resection.
The relationship between circulating tumor cell (CTC) levels in the portal vein and surgical procedure or tumor related factors.
Central vein blood. In the central vein blood sample, there was no significant increase in CTC levels for DT and AR in the AA and NA group (Figure 2C and D). However, the sub-analysis for tumor size >70 mm revealed that the CTC levels were significantly increased for DT (p=0.049) and AR (p=0.049) in the NA group (Figure 2E and F). Sub-analysis of the three surgical procedures revealed that the CTC levels significantly increased for AR in cases without hanging maneuver (p=0.003). In cases with a tumor histology of poor differentiation, the CTC levels were significantly increased for DT (p=0.028) (Table III).
The relationship between circulating tumor cell (CTC) levels in the central vein and surgical procedure or tumor related factors.
Peripheral blood. In the peripheral blood specimens, there was no significant increase in CTC levels in either group and both CTC levels were decreased at AR.
Discussion
For surgeons, it is extremely important to be able to predict how a surgical procedure may cause tumor cells to spread to the surrounding liver parenchyma from the primary HCC during surgery. In the present study, we examined blood specimens from three different vessels (the portal vein, peripheral artery, and central vein) and at three different time-points (BM, DT, and AR) to determine changes in CTC levels during hepatectomy. Furthermore, we aimed to improve the feasibility of molecular detection of circulating cancer cells by using three primers (EpCAM, GPC-3, and CK18) (19). In previous reports, CTC detection was performed using EpCAM (9, 20). Which constitute only approximately 35% of HCC; thus, sensitivity of detection might be low (21). Owing to the heterogeneity of HCC and lack of an established single marker, we used three primers for the detection of CTCs (22). GPC3 and CK18 were reported to be reliable biomarkers for CTC detection in HCC (19, 23).
Some researchers have detected CTCs at a single site and compared the method of AA and the conventional approach of resection with liver mobilization (15, 17). However, in these studies, blood specimens were collected for CTC detection only after surgery or at a single peripheral site. To the best of our knowledge, this is the first study to examine the correlation between hepatectomy procedures and CTCs collected at different surgical time-points and from vessels near the liver.
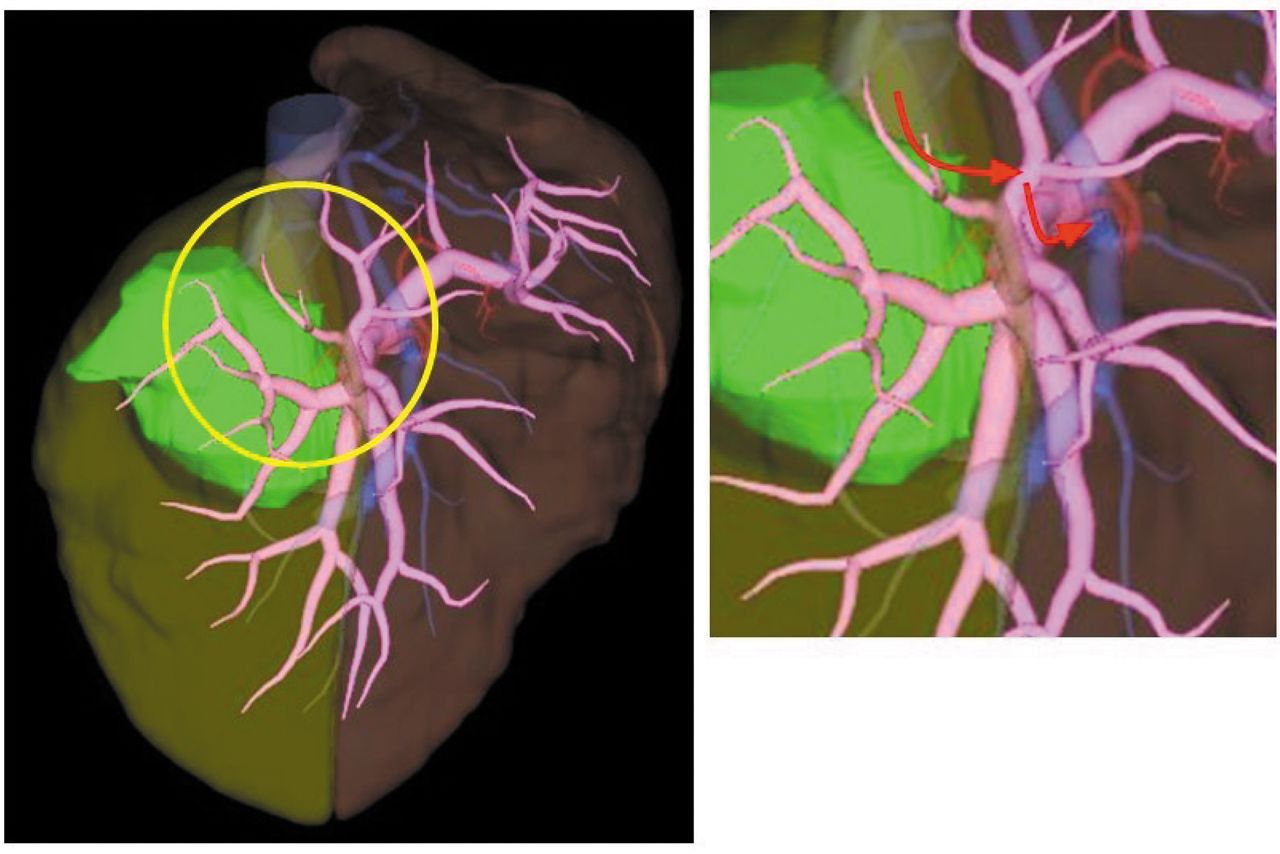
Intraoperative manipulation of HCC, especially large tumors, has been regarded as a risk factor of tumor cell dissemination via the portal vein circulation, which could account for the early widespread of intrahepatic recurrence frequently seen after resection of advanced HCC (2, 24-26). In our study, the risk of tumor cell dissemination to the portal vein was reduced by utilizing the AA surgical technique. Specially, liver mobilization and the hanging maneuver play significant determining roles for tumor dissemination. The blood vessels that penetrate the tumor capsule are the least resistant pathways to tumor prolapse (27), and tumor fragments may disseminate via portal vein branches during liver mobilization to form peripheral intrahepatic metastatic lesions. Upfront hilar vascular dissection is performed to suppress the cancer cell dissemination due to the insulation effect from the regurgitation of tumor-relevant portal flow and reduction of the intratumoral pressure. However, changes in CTC levels during hepatectomy are independent of hilar vascular dissection. A recent report revealed that micro portal vein invasion or intrahepatic metastasis was often detected in nearly all portal territory of HCC (25). Thus, we inferred that liver mobilization caused the tumor cells to spread via the peripheral portal branches surrounding the tumor, which act as an efferent vessel system independent of the tumor-relevant hilar vasculature procedure before transection. For example, in the case of a posterior sectionectomy, as the catheter tip was placed at the bifurcation of the right and left portal veins, even though the posterior branch was completely dissected at the hepatic hilum before mobilization, CTCs could have back-flowed from the anterior portal branch via the peripheral portal branches proximal to the cancer-bearing portal territory. A 3-dimensional CT image of a patient who underwent posterior sectionectomy is shown in Figure 3. In this case, the tumor was located in the posterior section and the peripheral branch of the anterior portal vein extended near the tumor, and the tumor cells may have regurgitated through the peripheral branch of the anterior portal vein.

A 3D-CT image of a patient who underwent posterior sectionectomy. The portal vein inflows from outside the resected area. Tumor cells may be disseminated from the tumor lesion during liver mobilization and enter the portal circulation via the anterior branch of the portal vein (inset, red arrows).
The assessment of blood specimens from the central vein, revealed that CTC levels significantly increased in the NA group for patients with tumors >70 mm in diameter. As reported earlier, large HCC demonstrate high incidences of microscopic venous invasions and is independently related to postresectional outcome (28). Additionally, a large HCC is the single highest risk factor for lung metastasis after hepatectomy (29). Considering these findings, it is evident that liver mobilization in cases of large HCCs may contribute to the dissemination of CTCs via the hepatic vein circulation. Furthermore, CTC levels significantly increased in patients for whom the hanging maneuver was not performed. The liver hanging maneuver procedure described by Belghiti et al. has become a common technique for liver resection (30). Furthermore, this procedure has been reported to reduce intraoperative blood loss and is associated with longer overall survival (31). A recent study reported that in patients with HCC≥100 mm, AA without liver mobilization resulted in better survival outcomes compared to a surgical approach with liver mobilization (14, 32). In large HCCs, combining AA with the liver hanging maneuver may have reduced the dissemination of tumor cells into the hepatic and central veins and, consequently, suppressed metastasis. Interestingly, two patients with recurrence of lung metastasis had significantly elevated CTCs in the central vein for DT. In both patients, PIVKA-II was over 10,000 mAU/ml and microscopic hepatic vein invasion was detected in one patient.
In the peripheral blood specimens, there was no significant increase in CTCs in the patients of both the AA and NA groups. Therefore, the surgical procedure had a negligible effect on the dissemination of CTCs into peripheral blood.
The limitations of this study are that it is a single center study, with a small sample size. Therefore, further studies involving larger sample sizes, multiple centers, and comprehensive postoperative prognoses are crucial to better understand the correlation between surgical procedure and clinical outcome of patients with HCC.
Conclusion
AA liver resection is a technique aimed at reducing intraoperative blood loss for large HCCs. This technique also offers an oncological advantage by reducing the risk of tumor dissemination into the hepatic and systematic blood circulation. Thus, AA hepatectomy may improve the prognosis of patients with HCCs.
Acknowledgements
We gratefully acknowledge the work of the members of our laboratory, and we would like to thank Editage (www.editage.jp) for English language editing.
Footnotes
Authors’ Contributions
Shin Sasaki and Yoriko Nomura contributed equally to the study and are co-first authors. Shin Sasaki, Yoriko Nomura, and Tomoya Sudo contributed to study design and drafted the manuscript. Shin Sasaki, Yoriko Nomura, Hisamune Sakai, and Toru Hisaka contributed to acquisition, analysis, and interpretation of data. Yoshito Akagi, Masayoshi Kage, Hirohisa Yano, Osamu Nakashima, and Jun Akiba contributed to the revision and editing of the manuscript. Koji Okuda contributed to the study design and revision of the manuscript. All Authors read and approved the final manuscript.
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received May 20, 2022.
- Revision received June 20, 2022.
- Accepted July 8, 2022.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.