


Abstract
Background/Aim: Malignant biliary obstruction (MBO) is a life-threatening condition. We aimed to investigate the outcome of salvage percutaneous transhepatic biliary drainage (PTBD) in patients with unresectable MBO due to failure of management by endoscopic retrograde cholangiopancreatography (ERCP) and/or prior surgical bypass. Patients and Methods: Fifty-two consecutive patients (mean age, 69 years; 44.2% women) underwent salvage PTBD between 2013 and 2020. Results: The median overall survival rate was 4.2 months, with a 95% confidence interval (CI) of 1.9-5.7. The median overall survival (OS) were 11.1 months and 1.9 months for patients who underwent chemotherapy (n=17) and best supportive care (n=35), respectively (p=0.0005). Independent factors predicting poor outcome were best supportive care, with a hazard ratio (HR) of 3.3 (95%CI=1.3-8.5), American Society of Anesthesiologists physical status classification (ASA) with a HR of 13.5 (95%CI=1.3-136.0) and Eastern Cooperative Oncology Group (ECOG) performance status of 4, with a HR of 3.3 (95%CI=1.0-6.2). Conclusion: Salvage PTBD with chemotherapy has the potential to achieve prolonged survival in patients with unresectable MBO, including those with failure of ERCP and/or surgical bypass.
Malignant bile duct obstruction (MBO) is a life-threatening disease, with an incidence of 15 per 100,000 people of the calculated prevalence in 2020 (1). The most common causes of MBO are pancreatic cancers and cholangiocarcinomas. Other etiologies include gallbladder carcinoma, hepatocellular carcinoma, lymphoma, and other malignant tumors with regional invasion or lymph node metastasis (2). Despite technological advances, most of these diseases are diagnosed in the late stages or recur after treatment and are unresectable (3). The goal of resectable MBO is to proceed with surgical resection. Options for palliative therapy of MBO have an important purpose, mainly to relief of symptoms and delay of disease progression.
In unresectable pancreatobiliary malignancies, chemotherapy is considered the standard treatment and cornerstone of patient management. However, exacerbation of liver function due to MBO may limit the administration of chemotherapy by interfering with the hepatic metabolism of drugs and their biliary elimination. Biliary drainage before palliative chemo-therapy is mandatory. Recently, endoscopic drainage has been recommended as the first-line approach for managing MBO (4-6). However, endoscopic procedures fail in approximately 6% to 7% of cases (7). In our institution, percutaneous transhepatic biliary drainage (PTBD) has been used as a salvage procedure to set a tract for internal and/or external drainage in cases of failure or insufficient effect of endoscopic drainage. However, there are very limited data concerning the outcomes of patients who receive salvage PTBD, especially in the management of palliative chemotherapy.
This study aimed to retrospectively investigate the clinical and oncological profiles and prognosis of patients who received palliative chemotherapy after salvage PTBD for unresectable MBO, where endoscopic management and surgical bypass failed at a single institution, and to evaluate predictive factors that lead to better patient selection for salvage PTBD.
Patients and Methods
This study included 52 patients who underwent salvage PTBD for unresectable MBO in cases of failed or unsuitable endoscopic management between 2013 and 2020 at the Department of Surgery, Kurume University Hospital. In our institution, the endoscopic management of unresectable MBO is the first line approach even in patients with surgically-altered anatomy or hilar biliary obstruction. The reasons for salvage PTBD were as follows: technically failed endoscopic drainage, 24 (46%) cases; insufficient endoscopic drainage, 14 (27%) cases; poor performance status, 7 (13%) cases; duodenal obstruction, 3 (6%) cases; and surgically-altered anatomy as surgical bypass, 4 (8%) cases. All procedures were performed under local anesthesia. The procedure was performed under ultrasonography and fluoroscopy guidance by experienced interventional radiologists. The study protocol was approved by the ethical committee of Kurume University Hospital (no.21040/2021).
Variables collected and analyzed from the electronic medical records included age, sex, pre-procedure American Society of Anesthesiologists physical status classification (ASA) class (8), ECOG performance status (ECOG PS), comorbidities (cardiovascular disease, diabetes, renal disease, and pulmonary disease), type of malignant disease, serum bilirubin concentration, white blood cell count and C-reactive protein level. Malignant disease was classified according to cancer type as primary or metastatic. Based on radiological findings, the obstruction level was classified as perihilar or distal bile duct obstruction. The highest bilirubin value, white blood cell count and C-reactive protein level were observed in the 3 days before the procedure. Survival rates were defined as the interval between the initial PTBD and patient death or last follow-up.
Statistical analysis. Time-to-event endpoints were analyzed using the Kaplan–Meier method, and between-treatment comparisons for OS were conducted using the log-rank test with a two-sided significance level of 5%. Cox proportional hazard analysis was used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs). Chi-square tests were used to compare quantitative and categorical variables based on p<0.05. A two-sided significance level of 5% was considered statistically significant. All statistical analyses were performed using JMP version 15 (SAS Institute, Cary, NC, USA).
Results
During the study period, 52 patients were treated with salvage PTBD. The median follow-up period was 4.2 months after PTBD. The majority of the patients were men, with a median age of 69 years (range=44-87 years). There were 14 different primary malignancies, but the majority of cases were either pancreatic (n=15, 28.8%) or biliary tract cancer (n=15, 28.8%).
As shown in Table I, bile duct obstruction was due to local progression of the primary tumor in 30 patients (57.7%). Among metastatic cancers, metastasis origin included gastric cancer in eight (36.4%) patients, colorectal cancer in four (18.2%) patients and ten (45.4%) other different types of primary cancer in 22 patients. The obstruction location was found in the perihilar bile duct in 13 patients (25.0%), in the distal bile duct in 35 patients (67.3%), and at the choledocojejunostomy in four patients (7.7%). An internal and external drainage were used in 36 (69%) patients, while sole external drainage was used in 16 (31%) patients. A total of 17 patients (32.7%) received chemotherapy after salvage PTBD, while 35 patients (67.3%) did not receive chemotherapy. The main exclusion criteria for chemotherapy evaluation were poor performance status, age, and advanced disease such as bowel obstruction due to peritoneal dissemination. The median OS after PTBD was 4.2 months (95%CI=1.9-5.7), and six patients (11.5%) were alive at 1-year post-drainage.
Univariate analysis of demographics and clinical characteristics.
Efficacy and complications. Successful biliary tract decompression, and relief from symptoms, such as appetite and fatigue, was achieved in all cases. The overall rate of all complications was 17.3%. Cholangitis and acute pancreatitis occurred in one patient. Other minor complications included limited bleeding, pain around the catheter, and a minor bile leak, which were observed in three, two, and one patient, respectively. All complications were effectively controlled using conservative medical treatment. The related mortality was 0%.
Survival. In this study, 22 patients had already received initial chemotherapy: six had pancreatic cancer, six biliary tract cancer, and 10 other malignancies. Among the 17 patients who received chemotherapy after salvage PTBD, four had pancreatic cancer, nine biliary tract cancer, and four other malignancies. The median survival of the 17 chemotherapy-treated patients was 11.1 months, and five patients were alive 1 year after PTBD (p=0.0005; Table I, Figure 1).

Survival rate after percutaneous drainage for biliary obstruction in patients with or without chemotherapy. PTBD: Percutaneous transhepatic biliary drainage.
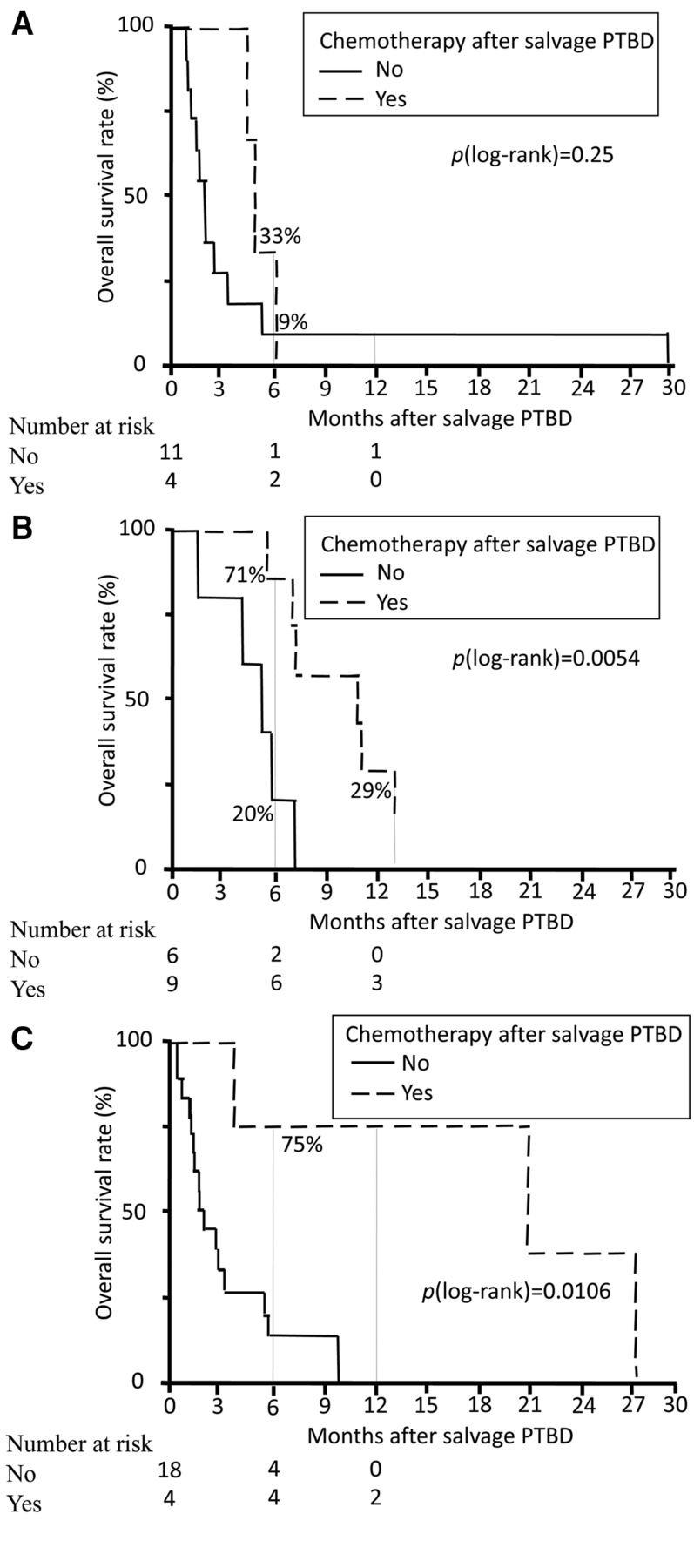
Our present results showed no statistically significant survival differences between pancreatic cancer patients who underwent chemotherapy after PTBD and those who received only best supportive care (p=0.25; Figure 2A). Both cancer groups gained significant survival benefits with chemotherapy, with a median survival of 11.2 months for the biliary tract cancer group (p=0.0054; Figure 2B) and 21.3 months for the other malignancies group (p=0.0106; Figure 2C).

Kaplan–Meier curve of the survival of patients with pancreatic, biliary tract, or metastatic cancer after percutaneous drainage for biliary obstruction. A) Survival rate after percutaneous drainage for biliary obstruction in patients with pancreatic cancer treated with or without chemotherapy. B) Survival rate after percutaneous drainage for biliary obstruction in patients with biliary tract cancer treated with or without chemotherapy. C) Survival rate after percutaneous drainage for biliary obstruction in patients with metastatic malignancies treated with or without chemotherapy. PTBD: Percutaneous transhepatic biliary drainage.
Combination chemotherapy was administered to 13% (2/15) of patients with pancreatic cancer (oxaliplatin, irinotecan, fluorouracil, leucovorin, or nab-paclitaxel and gemcitabine) and 27% (4/15) of patients with biliary tract cancer (gemcitabine with cisplatin or gemcitabine with S-1). Two patients with pancreatic cancer had already received second-line treatments. None of the patients with pancreatic cancer received a third-line treatment. Four patients with biliary tract cancer received second-line treatment. The median survival of the 35 patients treated with best supportive care was 1.9 months (Table I and Figure 1), 6.1 months in patients with ASA PS3, and 2.4 months in patients with ASA PS4 (p=0.0038, Figure 3A), 4.3 months in patients with ECOG PS3, and 1.8 months with ECOG PS4 (p=0.0052, Figure 3B). Only one (2.9%) of the patients with best supportive care was alive at 1 year after PTBD.

Kaplan–Meier curve of survival after percutaneous drainage for biliary obstruction according to American Society of Anesthesiologists physical status classification (ASA) classification and Eastern Cooperative Oncology Group (ECOG) performance status. A) Survival rate after percutaneous drainage for biliary obstruction according to ASA classification based on the Cox proportional hazards model. B) Survival rate after percutaneous drainage for biliary obstruction according to ECOG performance status based on the Cox proportional hazards model.
Furthermore, univariate analyses revealed that higher median survival times were associated with lower ASA class, lower ECOG performance status, and ability to receive chemotherapy after PTBD (Table I). Multivariate analysis revealed that poor prognostic status was associated with ASA class 4, EOCG PS 4 and unable to receive chemotherapy (Table II).
Multivariate Cox regression analysis of factors associated with survival after percutaneous biliary drainage for malignant obstructions.
Figure 2 and Figure 3 show survival times according to bile duct obstruction etiology (Figure 2A-C), ASA PS (Figure 3A) and ECOG PS (Figure 3B).
Discussion
The results of our study showed that patients who underwent salvage PTBD and subsequent chemotherapy had significantly better survival than those treated with best supportive care after drainage for MBO patients with biliary tract cancer or metastases when endoscopic management was unsuitable or unsuccessful. Our results showed no statistically significant survival differences between patients with local progression of the primary cancer and metastatic disease in the univariate analysis. In addition, poorer prognosis was independently predicted by an ASA PS 4 and ECOG PS 4. The overall median survival in our cohort was only 4.2 months after drainage, which is in agreement with previous reports (9-16).
In this study, the standard chemotherapy for biliary tract cancer was gemcitabine or S-1 alone. In our series, the median survival was 11.2 months for patients with biliary tract cancer who received chemotherapy after PTBD and 5.4 months for those who received the best supportive care. Niemela et al. (16) reported a better median survival of 15.1 months in patients who can undergo chemotherapy after palliative PTBD, and a poor median survival of 1.9 months in patients unable to receive chemotherapy. Recently, the combination of gemcitabine and S-1 or cisplatin has been shown to significantly improve the outcomes of patients with advanced/recurrent biliary tract cancer (17). The survival figures may have been even better for our patients by introducing a new combination chemotherapy (16).
Our study showed that the median overall survival was better in patients with biliary obstruction due to metastasis-treated chemotherapy than in patients given best supportive care. Previous studies have also reported that survival is better in MBO patients due to metastases with good performance status and who can undergo chemotherapy after biliary drainage compared to patients unable to receive chemotherapy (18-24).
Concerning pancreatic cancer, our present results showed no statistically significant survival differences between patients who underwent chemotherapy after PTBD and those who received only the best supportive care. The median survival of our patients with pancreatic cancer treated with chemotherapy was 4.9 months and 1.9 months for those given the best supportive care. The aggressive nature of pancreatic cancer is well known and is associated with a very poor prognosis; however, there has been improvement in chemotherapy regimens. Since the 1990s, gemcitabine has been considered the standard agent of choice, but for advanced pancreatic cancer, gemcitabine is generally insufficient due to chemoresistance that develops in cancer cells. Although multiple agents have been evaluated in combination with gemcitabine or alone, few have demonstrated a positive impact on the survival of patients with pancreatic cancer. More recently, a higher response rate and significantly improved overall survival were observed with FOLFIRINOX and gemcitabine + nab-paclitaxel regimen compared with gemcitabine alone (25-28). In this study, only a portion of the patients was administered with these new combination chemotherapies. The outcome of patients with pancreatic cancer receiving chemotherapy could be improved by new combination chemotherapies (25, 29).
In this study, ASA PS was an independent factor predicting survival. Prognosis was poor for patients with an ASA PS of 4, among whom the median overall survival was 2.4 months and only two patients (6.5%) survived 1-year post-drainage. Prognosis was slightly better in patients with ASA PS3, who showed a median overall survival of 6.1 months and of whom four patient (25%) were alive at 1-year post-drainage. Prior studies have reported similar results (16).
The present study demonstrated that higher ECOG PS predicted poorer outcome following biliary drainage. Patients with an ECOG PS of 4 had poor prognosis, with a median overall survival of 2.4 months, and only two of the 31 patients (6.5%) were alive 1-year post-drainage, which is in agreement with previous studies (14, 18, 20, 22).
Biliary drainage in MBO may palliate symptoms with improvement in quality of life, prevention of complications such as sepsis, and reduction in bilirubin levels to improve the chances of delivering palliative chemotherapy based on performance status. As improvements in chemotherapy have shown a positive trend of prolonged survival in MBO patients, salvage PTBD has an increasingly important role in patients in whom endoscopic drainage or surgical bypass is unsuccessful or insufficient. Therefore, patients with poor PS should be critically considered when evaluating the usefulness of invasive percutaneous biliary drainage procedures.
There are limitations to this study. It was a single-center study involving a small patient population. Furthermore, although patients were enrolled prospectively and consecutively, our analysis was retrospective, non-randomized, and uncontrolled.
Conclusion
MBO is associated with poor outcomes and decreased survival rates. Biliary decompression through salvage PTBD discussed in this study can be performed to relieve symptoms, improve patient quality of life, and reduce the bilirubin level to improve the chances of chemotherapy based on performance status. In particular, patients with poor ASA PS and poor ECOG PS showed poor survival even after salvage PTBD.
Footnotes
Authors’ Contributions
DM: Study design; collection of data; manuscript writing and data analysis. HT, HS, KH, ST: collection of data. KO: quality control of data. RM, ST: Editing and review. YW, YN, YY, ST; quality control of data. SK, SA, TS, YG, HS, TH, YA; quality control of data, literature search and data analysis. All other coauthors discussed the content of the manuscript. All Authors read and approved the final manuscript.
Conflicts of Interest
All Authors declare no conflicts of interest or competing financial interests for this article.
- Received May 20, 2022.
- Revision received June 3, 2022.
- Accepted June 14, 2022.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.