


Abstract
Background/Aim: Definitive treatment for locally advanced head and neck squamous cell carcinoma (LAHNSCC) is often compromised in older adults due to concerns about potential treatment toxicity intolerance. We reviewed our institutional experience with definitive management of older adults with LAHNSCC. Patients and Methods: From our Institutional Review Board-approved registry, we identified patients aged >60 years with stage III-IV, M0 LAHNSCC (seventh/earlier editions of the American Joint Committee on Cancer classification) treated with definitive radiotherapy from 1993-2019. Indications for concurrent chemotherapy included T3-4 or N2-3 disease. Multivariable analysis using Fine and Gray regression was performed to identify risk factors associated with recurrence. The cumulative incidence method was used to calculate recurrence rates. Results: Overall, 350 patients were identified: 223 aged 60-69, 82 aged 70-74, and 45 aged ≥75 years. Median follow-up was 36.3 months. Two-year recurrence rates were 13.7%, 20.2% and 34.8%, respectively; human papillomavirus-positive disease was present in 190 (85%), 44 (54%), and 25 (56%), respectively; and systemic therapy was given to 194 (87%), 64 (88%), and 23 (56%) patients, respectively. Factors significantly associated with increased risk of recurrence included age ≥75 years, Karnofsky performance status 70-80, clinical N2c-N3, and Charlson score 2-3. Conclusion: Patients aged ≥75 years received less aggressive therapy and experienced increased recurrence compared to younger patients. Outcomes for those aged 70-74 years were similar to younger patients treated with aggressive therapy, despite their inferior performance status/comorbidity, and such patients should not routinely be excluded from standard-of-care therapy. Further study is needed to optimize therapy for a redefined older adult (age ≥75 years) population.
The estimated incidence of head and neck cancer in the United States was 66,000 in 2021, with older adults comprising an increasing percentage of these patients (1, 2). Projections of age demographics in the United States forecast 70 million people will be aged 65 years or older by the year 2030 (3). Additionally, the median age at diagnosis of human papillomavirus (HPV)-related oropharyngeal squamous cell carcinoma (SCC) is increasing due to the increased proportion of older adult patients having these virally-mediated cancer types (4). There is a paucity of cancer outcome data specific to older adult patients because they are under-represented in cancer-treatment trials (5). Definitive radiotherapy (RT) with concurrent platinum-based chemotherapy has become a standard treatment for patients with locoregionally advanced head and neck SCC (LAHNSCC) (6). While less morbid than tri-modality therapy, definitive concurrent chemoradiotherapy can cause challenging toxicity, even for young and fit patients. The addition of concurrent chemoradiotherapy to definitive RT for LAHNSCC is well established given the survival benefit observed in numerous studies (7-10). However, this benefit was not seen in patients over 70 years of age in the Meta-Analysis of Chemotherapy in Head and Neck Cancer (MACH-NC) (11). In light of the results of the MACH-NC, as well as concerns about the anticipated tolerance of treatment toxicities, definitive treatment of LAHNSCC in older adult patients often comprises RT without concurrent cytotoxic chemotherapy (12).
The recommendation to forgo concurrent chemotherapy with definitive RT for older adult patients is an area of controversy, especially in those over 70 years old with excellent performance status and few comorbidities. It is unclear whether benefits of concurrent chemoradiotherapy would outweigh competing risks in selected older adult patients. The degree to which treatment toxicity, tumor biological differences due to advanced age, or other unknown competing risks contribute to the diminishing benefit of concurrent systemic therapy among older adult patients reported in MACH-NC is also unknown. The purpose of this study was to assess outcomes and patterns of practice in older adult patients with LAHNSCC receiving definitive therapy and to provide comparison with a younger cohort of similarly-staged patients. The Authors’ hypothesis was that selected patients over 70 years old can be safely treated with intensified therapy, achieving outcomes comparable to those of younger patients.
Patients and Methods
We queried our Institutional Review Board-approved institutional registry of patients with head and neck cancer treated with definitive RT with or without systemic therapy from 1993-2019. We included patients with non-metastatic, stage III to IVB [seventh edition of the American Joint Committee on Cancer (AJCC) classification (and earlier) (13)] SCC of the larynx, hypopharynx, or oropharynx. Data were collected on all patients aged 70 years and older, and on a similarly-staged cohort of patients aged 60-69 years for comparison of outcomes and patterns of practice. Patients were treated with definitive RT with a minimum prescribed dose of 60 Gy delivered via 3D-conformal radiotherapy (3D-CRT) or intensity-modulated radiotherapy (IMRT) techniques. Systemic therapy included induction or concurrent platinum-based cytotoxic chemotherapy or concurrent epidermal growth factor receptor inhibition (cetuximab). Indications for systemic therapy included either T3-T4 primary tumors or N2-N3 nodal disease based on the seventh edition of the AJCC staging system. Endpoints included cumulative incidence of disease recurrence defined as any local, regional or distant failure. Baseline characteristics of patients aged 60-69, 70-74, and ≥75 years were compared. The chi-square test was used to make comparisons among baseline categorical variables, and analysis of variance was used to make comparisons among continuous variables. Disease recurrence rates were calculated using cumulative incidence analysis with death from any cause as a competing risk, and Gray’s test was used to compare differences in recurrence rates among age groups. Fisher’s exact test was used to compare toxicity among the three age groups. The following factors were included in the univariate analysis: Age, clinical stage, pre-treatment Charlson comorbidity index, Karnofsky Performance Status (KPS), systemic therapy administration, smoking status, HPV status, and RT dose. Factors significant on univariate analysis were included in a multivariable analysis. All statistical tests were two-sided with a value of p<0.05 considered to be statistically significant. Statistical analysis was performed using SAS version 9.4 software, SAS Institute, Cary, NC, USA.
Results
A total of 350 patients were analyzed among the three age groups: 60-69 (n=223), 70-74 (n=82), and ≥75 (n=45) years. Table I presents the baseline characteristics of all patients included in the analysis. The median follow-up was 47.6 (range=2-202) months for patients aged 60-69 years, 40.1 months (range=3-189) for those aged 70-74 years, and 27.4 months (range=2-92) for those aged ≥75 years. The median age overall for patients was 67 (range=60-86) years. The median age by age group was 63.9, 72.1, and 77.7 years, respectively.
Patient characteristics.
There were several significant differences in characteristics between the groups. The older cohorts had a smaller proportion of HPV-positive tumors: 54% of those aged 70-74 years and 56% of patients aged ≥75 years, compared to 83% of patients aged 60-69 years. Among patients for whom performance status data were available, the KPS score was 90-100 in 27% of older adult patients (n=34) compared to 67% in the younger cohort (n=150). Additionally, pre-treatment Charlson Comorbidity Index scores were significantly higher in the older adult cohorts. Please refer to Table I for additional patient characteristics.
Treatment characteristics are presented in Table II. Systemic therapy was indicated for 312 (89%) patients in the entire cohort; 198 (89%) of those age 60-69 years, 73 (89%) of those 70-74 years, and 41 (91%) of those ≥75 years. Systemic therapy was given significantly less frequently at 56% to patients aged ≥75 years compared to 96% for those aged 60-69 years and 88% for those aged 70-74 years when indicated (p<0.0001). Additionally, the use of cetuximab instead of cytotoxic chemotherapy was higher among patients aged ≥75 years compared to younger groups: at 57% compared to 13% for those aged 70-74 years and 12% for those aged 60-69 years. Of patients 60-69 years old receiving systemic therapy, 81% were treated with concurrent cisplatin-based regimens while 26% of patients age ≥75 years were treated with concurrent cisplatin.
Treatment characteristics and outcomes.
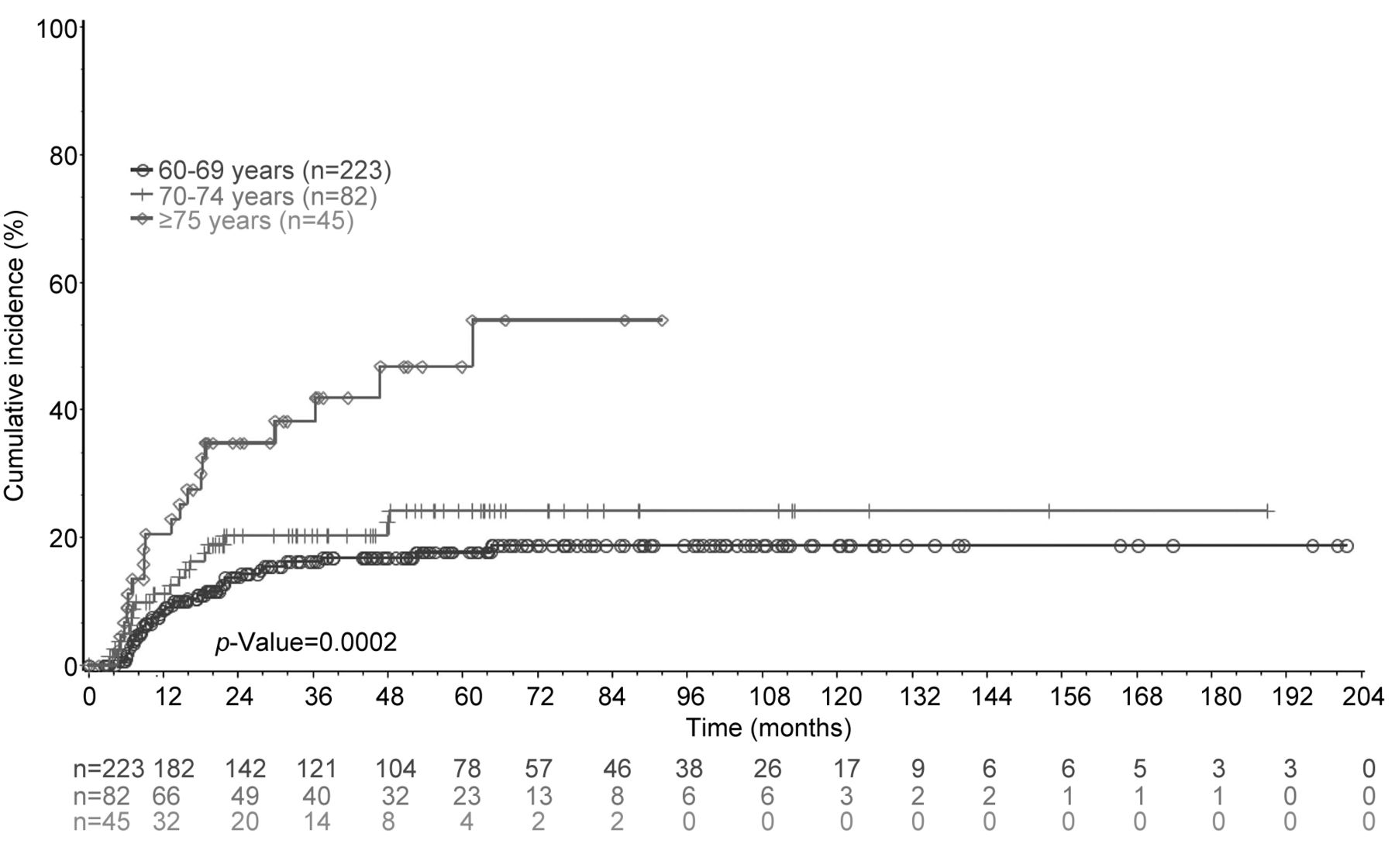
The 2-year cumulative incidence of any disease recurrence was 13.7%, 20.2% and 34.8% for patients aged 60-69, 70-74 and ≥75 years (p=0.0002). As shown in Figure 1, the disease recurrence rates of patients aged 70-74 and 60-69 years were comparable, while those ≥75 years old had a notably higher recurrence rate.

Cumulative incidence estimates for disease recurrence by age.
On univariate analysis (Table III), RT alone was not significantly associated with higher rates of recurrence compared to chemoradiotherapy among all patients, nor among patients with an indication for systemic therapy who did not receive it. On multivariable analysis adjusted for use of systemic therapy (Table III), the factors associated with increased risk of recurrence included age ≥75 years vs. 60-69 years, KPS 70-80 vs. 90, clinical N2c-N3 vs. clinical N0-N2b, and Charlson Comorbidity Index 2-3 vs. 0-1. Use of systemic therapy was not significantly associated with lower risk of recurrence on univariate or multivariable analyses.
Univariate and multivariable analyses for disease recurrence.
A subset analysis of recurrence by use of systemic therapy for older patients with an indication for systemic therapy revealed no benefit from the use of systemic therapy in either of the older cohorts. Patients aged ≥75 years who received systemic therapy in fact experienced a higher recurrence rate than patients who did not receive systemic therapy. These results, however, should be interpreted with caution due to the relatively small number of patients in this subset analysis.
As shown in Table IV, acute toxicity was comparable among age groups when using rates of feeding tube or tracheostomy placement within 90 days of completing RT as surrogates. Of note, our analysis revealed rates of feeding tube placement were generally higher than expected among all age groups. Of the patients aged 70-74 years who required feeding tube placement, 52% of these received 3D-CRT and 24% were treated with concurrent cisplatin/5-fluorouracil, both of which would be expected to result in higher rates of mucositis compared to IMRT and cisplatin alone, respectively. Rates of pre-existing dysphagia among patients requiring a feeding tube after RT were comparable among age groups. Rates of tracheostomy placement within 90 days of completing treatment were also low.
Toxicity outcomes.
Discussion
Choice of therapy in older adults with LAHNSCC presents a significant clinical challenge that requires accounting for multiple disease- and patient-related factors. Adding to the confusion is the relative under-representation of patients over the age of 70 years in clinical trials and the grouping of all patients over 70 years old into a single group in meta-analyses (11, 14). As a result, the current definition of “older adult” in head and neck cancer care is age ≥70 years. Accordingly, many older adults in their early 70s are given less aggressive therapy and are excluded from many prospective clinical trials. Given the heterogeneity within this population, we believe this definition of older adult may overlook a significant number of patients who would benefit from maximally aggressive therapy.
Our analysis has several key findings. Firstly, patients 70-74 years old did not experience significantly worse recurrence outcomes compared to those aged 60-69 years despite having significantly higher comorbidity indices and poorer performance status. Even with higher comorbidities and poorer performance status compared to younger patients, those aged 70-74 years received systemic therapy when indicated 88% of the time, suggesting the favorable recurrence rate was not attributable to careful selection of healthier patients compared to the oldest cohort. While patients of 70-74 years old received maximally intensive therapy similarly to patients aged 60-69 years, the degree to which concurrent systemic therapy drove this result remains unclear. A larger analysis of patients aged 70-74 years is needed to evaluate the potential impact of concurrent systemic therapy for this age group. Nevertheless, these data suggest that patients 70-74 years old represent a group for whom favorable outcomes are possible with maximally intensive therapy.
Secondly, patients aged ≥75 years experienced higher recurrence rates compared to younger patients, both in cumulative incidence analysis (Figure 1 and Table IV) and on multivariable analysis (Table III). Recurrence is an important outcome as shown by a recent population-level study from Chesney et al. which demonstrated a higher rate of cancer-related deaths than non-cancer-related deaths among older adults fit for intensive therapy with surgery (15). The higher recurrence among the oldest cohort in our study is potentially attributable in part to the lower proportion of those with HPV-positive oropharyngeal cancer and a slightly higher proportion of current/former smokers compared to the youngest cohort. HPV-negativity and >10 pack-year smoking history were both poor prognostic risk factors for survival on a recursive partitioning analysis of RTOG 0129 (16). Additionally, the higher incidence of recurrence among the oldest patients may be in part attributable to compromised treatment with regard to systemic therapy. As seen in Table II, 56% of the oldest patients received systemic therapy, and cetuximab was more frequently chose for this cohort. However, it is not clear from our analysis that compromised systemic therapy in the oldest cohort was related to increased recurrence. In cumulative incidence analysis, we observed a lack of disease recurrence benefit in those aged ≥75 years who received systemic therapy compared to those who did not, a finding in line with the results of the MACH-NC for older adults subgroup analysis described above (11). Multivariable analysis demonstrated higher recurrence rates in patients age ≥75 years compared to those aged 60-69 years, regardless of whether systemic therapy was given (hazard ratio=2.60, 95% CI=1.27-5.30, p=0.009) or not given (hazard ratio=2.39, 95% CI=1.18-4.86, p=0.02). In short, this cohort aged ≥75 years may represent patients with more aggressive tumor biology than that aged 60-69 years.
Thirdly, older patients were able to tolerate their treatment without an overabundance of acute toxicity compared to younger patients. Despite 88% of patients aged 70-74 years receiving systemic therapy, acute toxicity outcomes were comparable to those of the youngest cohort. Patients aged 70-74 years experienced a non-significantly higher rate of feeding tube placement (51%) compared to the youngest (41%) and oldest (31%) cohorts, however. Additionally, acute treatment toxicity as the reason for feeding tube placement was 45% among patients aged 70-74 years compared to the younger cohort at 15%. One caveat to this particular finding is that medical records were sparse, with the reason for feeding tube placement in 68% of the younger cohort being categorized as “other/unknown”. Additionally, the 70- to 74-year-old cohort were more frequently treated with 3D-CRT instead of IMRT, and more frequently received concurrent cisplatin/5-fluorouracil, a regimen known to frequently cause significant stomatitis and nausea.
Our analysis has limitations aside from the usual qualifications that accompany a retrospective study. Firstly, the number of older adult patients was small and limited the power and types of subset analyses performed. Secondly, the study cohort included patients encompassing multiple eras of diagnostic and therapeutic advancement from 1993-2019.
The addition of concurrent systemic therapy to definitive RT is the standard of care for treatment of LAHNSCC due to the overall survival and distant control benefits seen in the MACH-NC of over 17,000 patients in 93 trials (11, 17). Sub-group analysis in this meta-analysis demonstrated a decreasing benefit from the addition of systemic therapy with increasing age, with no survival benefit seen in patients over the age of 70 years. However, this meta-analysis highlights the relative paucity of prospective data for the use of systemic therapy among older adult patients as only 7% of those receiving systemic therapy in these trials were over 70 years old. Where cause of death data were available, the MACH-NC authors reported that the proportion of deaths not related to head and neck cancer was higher among those over 70 years old (39%) compared to those under 50 years old (15%), although the number of patients was too small to draw meaningful conclusions. A recent analysis of the MACH-NC by Zakeri et al. examined the relationship between risk of cancer progression relative to competing mortality and benefit to more intensive treatment for patients with LAHNSCC (18). The authors observed a significant survival benefit with the use of chemotherapy among patients with higher risk of cancer progression relative to competing mortality risk. While the use of multi-agent chemotherapy is associated with greater myelosuppression and supportive care needs in older adult patients (19, 20), previous retrospective data from our institution revealed similar oncological outcomes in a small cohort of patients aged ≥70 years receiving concurrent cisplatin-based chemotherapy compared to younger patients (21). Additionally, this analysis included patients treated largely in the 3D-CRT era, and clinician comfort by adding concurrent systemic therapy may increase with improved normal tissue-sparing dosimetry accompanying modern image-guided IMRT techniques. This may explain the results of a contemporary analysis of the National Cancer Database examining the use of systemic therapy with definitive RT for LAHNSCC among older adults which revealed an increased frequency of systemic therapy use from 64% in 2004 to 86% in 2012 (22). While in the analysis these older adults receiving systemic therapy were likely highly selected, the authors revealed the use of systemic therapy was associated with significantly improved overall survival on multivariable analysis. Multiple other National Cancer Database analyses of older adults with LAHNSCC demonstrated a benefit of concurrent chemoradiotherapy for selected patients aged >70 years (23, 24).
While concurrent cetuximab was observed to result in inferior survival compared to cisplatin in prospective randomized trials (25, 26), concurrent cetuximab along with RT was frequently given to the older adults in our analysis due to the survival benefit seen over RT alone (27). Alternative systemic therapy options for platinum-ineligible patients with LAHNSCC is an area of active prospective study among patients aged ≥70 years with moderate to severe comorbidity undergoing RT with either cetuximab or durvalumab for stage III-IVB HNSCC. However, our analysis suggests that the age cutoff of 70 years may inappropriately exclude patients for whom maximally intensive therapy is worth pursuing. While the level of evidence from this single-institution, retrospective analysis is insufficient to support the assertion that patients older than 70 years benefit from the addition of chemotherapy, our study corroborates a growing body of evidence showing that selected older patients can be safely treated with intensified therapy to achieve comparable outcomes to younger patients.
Conclusion
Compared to younger patients, patients ≥75 years old undergoing treatment for LAHNSCC experienced higher rates of recurrence, even when controlling for comorbidities and performance status. Patients between the ages of 70 and 74 years received maximally aggressive therapy and experienced similar recurrence outcomes to younger patients despite having higher comorbidity scores and inferior performance status. Patients 70 to 74 years old should not be routinely excluded from receiving standard of care therapy. Further study is required to optimize outcomes for the older adult (≥75 years) population.
Acknowledgements
This work was supported by the Melvin Markey Discovery Fund at the Cleveland Clinic.
Footnotes
Authors’ Contributions
Conception and design: T.D. Smile, S.A. Koyfman and D.J. Adelstein. Administrative support: T.D. Smile, B. Matia, S.A. Koyfman and D.J. Adelstein. Provision of study materials or patients: J.L. Geiger, N.P. Joshi, N.M. Woody, S.A. Koyfman, D.J. Chute, C.C. Griffith and D.J. Adelstein. Collection and assembly of data: T.D. Smile, C. Domb and C.W. Fleming. Data analysis and interpretation: T.D. Smile, C.A. Reddy, S.A. Koyfman and D.J. Adelstein. Article writing: T.D. Smile, C.W. Fleming, C.A. Reddy, S.A. Koyfman and D.J. Adelstein. Final approval of article: All Authors.
Conflicts of Interest
J.L. Geiger: Regeneron advisory board member, Institutional research support from Regeneron, Genentech, and Alkermes. S.A. Koyfman: Consulting for Merck and Regeneron, Research support from Bristol Meyers Squibb and Merck, Honoraria from UpToDate. None of the other Authors have any conflict to declare.
- Received May 17, 2022.
- Revision received June 8, 2022.
- Accepted June 15, 2022.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.