


Abstract
Background/Aim: Intradural extramedullary spinal metastases (IESMs) may severely affect quality-of-life of oncological patients. Several treatments are available but their impact on prognosis is unclear. We systematically reviewed the literature on IESMs of non-neurogenic origin. Materials and Methods: PubMed, Ovid EMBASE, Scopus, and Web-of-Science were screened to include articles reporting patients with IESMs from non-neurogenic primary tumors. Clinico-radiological presentation, treatments, and outcomes were analyzed. Results: We included 51 articles encompassing 130 patients of a median age of 62 years (range=32-91 years). The most common primary neoplasms were pulmonary (26.2%), renal (20%), and breast (13.8%) carcinomas. Median time interval from primary tumor to IESMs was 18 months (range=0-240 months). The most common symptoms were sensory (58.3%) and motor (54.2%) deficits. Acute cauda equina syndrome was reported in 29 patients (37.7%). Lesions were diagnosed at magnetic resonance imaging (93.3%), myelography (25%), or computed tomography (16.7%). All patients underwent decompressive laminectomy with tumor resection, partial (54.6%) more frequently than complete (43.1%). Adjuvant radiation (67.5%) and/or systemic (13.3%) therapies were administered. After treatment, most patients had symptom improvement (70.8%) and optimal radiological response (64.2%). Four patients experienced IESMs recurrences (3.1%) with median local tumor control of 14.5 months (range=0.1-36 months). Deaths occurred in 50% of patients, with median overall survival of 6.7 months (range=0.1-108 months). Conclusion: Patients with IESMs have significant tumor burden with poor prognoses. Resection and locoregional radiation may offer favorable clinico-radiological responses but are limited in achieving optimal local control and survival.
- Extramedullary spine metastases
- intradural metastases
- neuro-oncology
- spine oncology
- spine metastases
- systematic review
Intradural extramedullary spinal metastases (IESMs) are uncommon entities, with an estimated prevalence of ≤5% among all spinal metastases (1-3). Despite the rarity, their incidence is recently increasing due to the improved management and increased survival of oncological patients, coupled with major advances in diagnostic imaging tools (4, 5). Presenting symptoms are non-specific and stem from tumor location, commonly characterized by axial and radicular pain, sensorimotor deficits, sphincter, and sexual dysfunction (6-8). Radiological diagnosis may be difficult as imaging characteristics may show some similarities with benign primary intradural spinal cord tumors (9, 10). Lesion biopsy and histopathological diagnosis are mandatory, particularly in patients with no cancer history, to guide metastatic diagnostic work-up and treatment planning. Of note, contrary to leptomeningeal metastases (LM), which present diffuse brain and/or spinal disease, IESMs are confined lesions amenable to focal regional treatment (11).
The management of IESMs is complex and comprises multiple therapeutic options, all of which somewhat effective but not risk-free (1, 5, 12). Surgical resection plays both a diagnostic and therapeutic role, preserving or improving functional status in selected patients and also showing some benefits in terms of survival (5). Several intraoperative adjuncts, including neuromonitoring, imaging guidance, and neuronavigation, have been introduced in spine oncology surgery, aimed at enhancing surgical performance and reducing risks (13-15). The confined space and the neighboring critical neurovascular structures pose serious challenges for surgical tumor resection. Locoregional radiotherapy and systemic chemotherapy represent additional options that should be discussed in multidisciplinary teams to weight feasible benefits, related to primary tumor responsiveness, to potential treatment-related adverse events (16, 17). Overall, IESMs are associated with poor prognosis, and the lack of optimal management strategies constitutes a major burden for affected patients.
Due to the rarity of IESMs, most conclusions are drawn from a limited number of case reports and case series, heterogeneous in clinical presentations and treatments (18, 19). In this systematic review, we comprehensively summarized clinical characteristics, management, and outcomes in patients with IESMs from non-neurogenic tumors.
Materials and Methods
Literature search. A systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (20). PubMed, Ovid EMBASE, Scopus, and Web of Science were searched from database inception to May 27, 2022, using the search query: [(intradural extramedullary) AND (spinal OR spine OR cauda equina) AND (metastases OR metastasis)]. Articles were exported to Mendeley, and duplicates were deleted.
Study selection. Inclusion and exclusion criteria were set a priori. Studies were included if they: 1) involved ≥1 patients aged ≥18 years with histologically confirmed IESMs from non-neurogenic primary tumors, 2) reported data on clinico-radiological features, treatment strategies, and post-treatment outcomes, 3) were written in English. Studies were excluded if they were: 1) literature reviews, animal studies, or autopsy reports, 2) studies involving patients only with diffuse leptomeningeal spinal metastases, 3) studies involving patients with spinal metastases from neurogenic primary tumors, 4) studies with unclear distinction between patients with IESMs and patients with intramedullary or extradural spinal metastases, 5) studies with insufficient clinical data, lacking ≥2 of clinico-radiological features, management strategies, or post-treatment outcomes.
Titles and abstracts of all collected articles were independently screened by two reviewers (P.P. and A.L.C.), who then assessed full texts of studies meeting the inclusion criteria. Any disagreements were settled by a third reviewer (A.S.H.). Eligible articles were included upon the pre-specified criteria and references were searched to retrieve additional relevant studies.
Data extraction. Data were extracted by one reviewer (A.L.C.) and then confirmed independently by two additional reviewers (P.P. and O.B.A.). Missing data were not reported by the authors. Extracted data included: authors, year, sample size, age, sex, primary tumor, concurrent systemic metastases, symptoms, tumor location, surgical technique, extent of resection, adjuvant therapy protocols, symptom improvement, radiological responses, local tumor control (LC), and overall survival (OS). Extent of resection was defined as “complete resection” for 90%-100% tumor resection and “partial resection” for <90% resection. Symptom improvement and radiological responses were appraised at last available follow-up. Post-treatment radiological responses were defined as: “complete response” (CR), for absence of IESM, “partial response” (PR), reduced IESM volume, “stable disease” (PD), for no change in IESM volume, “progression” (PD), for increase in IESM volume.
Data synthesis and quality assessment. Primary outcomes of interest were clinical presentation, management, and post-treatment outcomes in non-neurogenic IESMs. For each article, level of evidence was determined upon the 2011 Oxford Centre For Evidence-Based Medicine guidelines (21), and risk of bias was appraised by two independent reviewers (P.P. and O.B.A.) upon the JBI checklists (22). A study-level meta-analysis was not performed because all included articles had levels IV and V of evidence and hazard ratios could not be deducted. Patient-level data were collected for individual patient data meta-analysis.
Statistical analysis. SPSS V.25 (IBM Corp, Armonk, NY, USA) was utilized for all statistical analyses. Continuous variables are summarized as medians with ranges, and categorical variables as frequencies with percentages. The time intervals between tumor resection and IESMs recurrence (LC curve) or death (OS curve) were appraised with the Kaplan-Meier method.
Results
Study selection and overview. The initial search returned 1,575 citations (PubMed: 199, Ovid EMBASE: 990, Scopus: 208, Web of Science: 178) (Supplementary File 1). Nine case series and 42 case reports were included, evaluated as level IV and V of evidence (Supplementary File 2) (1, 4-8, 11, 23-67). For all included studies, quality assessment returned low risk of bias (Supplementary File 3), predisposing this review to a low risk of bias overall.
Demographics and characteristics of primary tumors. In total,130 patients diagnosed with non-neurogenic IESMs were collected (Table I). Patients were mostly male (55.4%), with a median age of 62 years (range=32-91 years). The most common primary neoplasms comprised lung cancer (26.2%), renal cell carcinoma (20%), breast cancer (13.8%), and prostate cancer (8.5%). Two patients reported by Gazzeri et al. (5) had unknown primary tumors. All primary neoplasms were treated with surgery (100%), and often with adjuvant radiotherapy (67.7%) and/or chemotherapy (20.8%). Systemic metastases were reported in 58.5% patients, frequently involving the brain (67.1%), the lungs (13.2%), and/or the vertebrae (13.2%). Castillo et al. (66) reported one case of IESM with concurrent LM.
Summary of patients’ demographics and primary tumors’ characteristics.
Clinical and diagnostic features of IESMs. Median time interval from the diagnosis of primary tumor to IESM occurrence was 18.0 months (range=0-240.0 months), with synchronous IESMs detected in 16 cases (12.3%). The most common presenting symptoms were sensory deficits (58.3%), motor deficits (54.2%), including paraparesis with difficult walking (15%), lower back pain (LBP, 40.8%), and radicular pain (59.3%) (Table II). Acute cauda equina syndrome (CES) was reported in 29/77 cases (37.7%). Strong et al. (45) and Saway et al. (60) documented two asymptomatic patients with renal cell and pancreatic carcinoma, respectively, diagnosed with IESM at oncological imaging follow-up. The diagnosis of IESMs was mainly obtained at T1-contrast magnetic resonance imaging (MRI) scans (93.3%), showing contrastenhancing lesions within the spinal dural sac and not involving the spinal cord, which encased or displaced the spinal nerve roots. Myelography was performed in 30 (25%) patients, showing partial or complete blockage of the contrast dye. Most lesions occurred in the lumbar (40%) and thoracic (32.3%) spine, with only 14 (10.8%) involving the cervical spine. Stein et al. (54) reported one patient with multiple IESMs involving the cervical and lumbar-sacral spine.
Summary of clinical and radiological features of intradural extramedullary spinal metastases.
Management strategies. All patients underwent decompressive laminectomy with tumor removal (100%), most frequently partial (54.6%) than complete (43.1%) (Table III). Biopsy alone was performed in 3 cases (2.3%). Locoregional radiation therapy was delivered in 81 patients (67.5%) at a median dose of 30 Gy (range=10-40 Gy). Most patients received external beam radiotherapy (EBRT) targeting the involved spine region. Pagano et al. (64) utilized palliative stereotactic radiosurgery (SRS) in one patient with lung IESM. Systemic chemotherapy was administered in 16 patients (13.3%). Castillo et al. (66) used intrathecal chemotherapy in one patient with a lung IESM and concurrent LM. No treatment-related complications were reported.
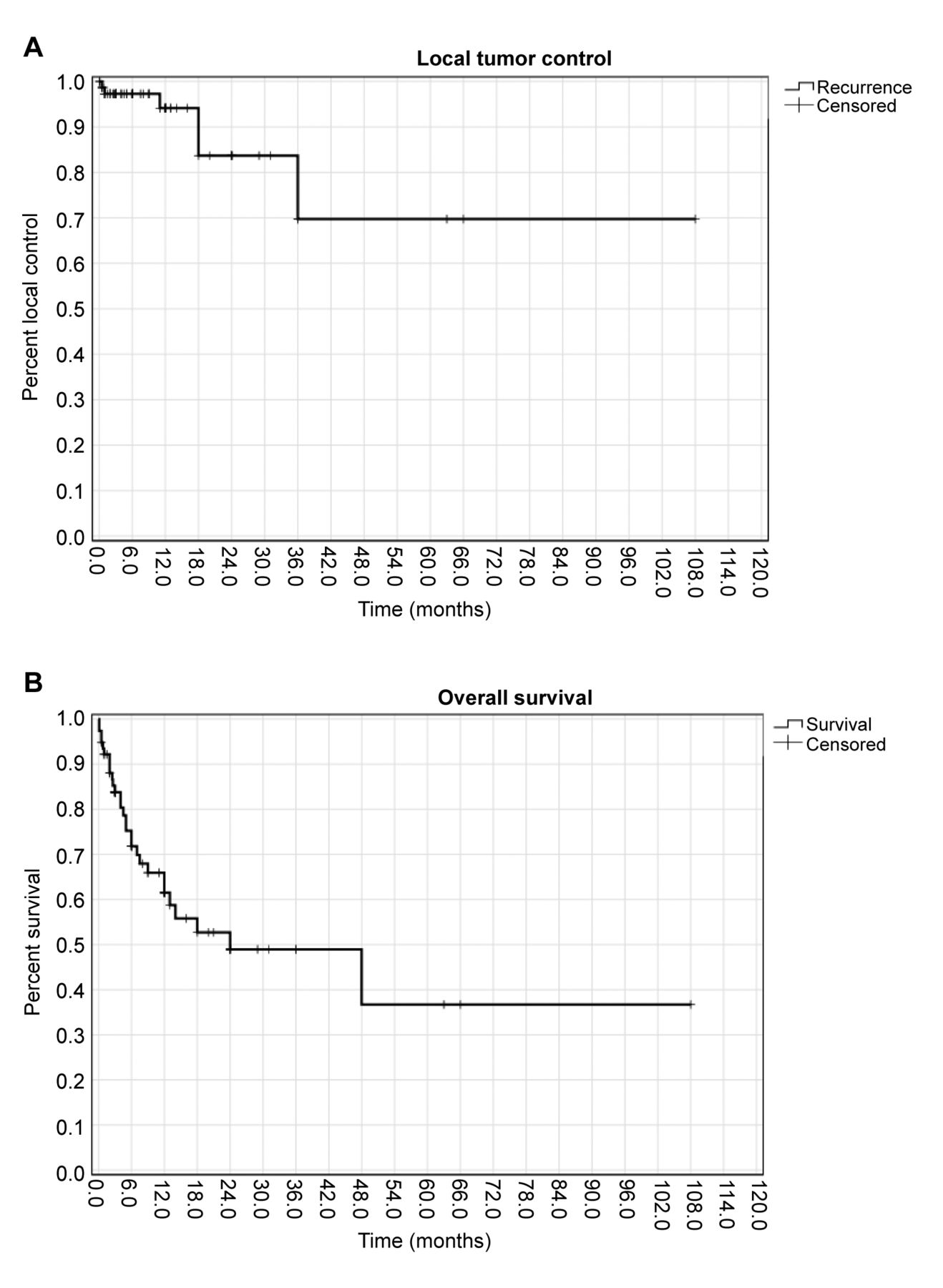
Post-treatment clinico-radiological outcomes and survival. Patients were followed-up for a median of 6.7 months (range=0.1-108 months) (Table III). Most patients (70.8%) achieved post-treatment symptom improvement. Recovery of the ambulatory status occurred in 13 of the 18 patients with pre-treatment paraparesis (72.2%). Documented radiological responses were: CR in 18 patients (15%), PR in 59 (49.2%), SD in 22 (18.3%), and PD in 21 (17.5%). IESM recurrences occurred in 4 patients (8.5%), with median LC of 14.5 months (range=0.1-36.0 months) (Figure 1). A 50% of patients died at last follow-up, with a median OS of 6.7 months (range=0.1-108 months).
Summary of treatment strategies and outcomes.

Kaplan-Meier curves of (A) local tumor control and (B) overall survival of the pooled cohort.
Discussion
Non-neurogenic IESMs may occur at later stages of advanced systemic tumors, often causing debilitating alteration of patients’ functional status. Advances in imaging and treatments may offer timely management, but clinical outcomes and survival have remained dismal. We found that IESMs frequently manifest with severe sensory and motor deficits, causing acute CES when involving the lumbar-sacral spine. Current therapies are mostly palliative, offering short-term clinico-radiological improvement. This review aimed to provide useful insights for managing IESMs within the context of other extradural and intramedullary spinal metastases.
IESMs comprise only 1-2% of all metastatic spine lesions, occurring less frequently than both vertebral (68) and intramedullary (69) spine metastases. In this review of non-neurogenic IESMs, the most common primary neoplasms comprised lung, renal, and breast carcinomas, reflecting their overall prevalence among oncological patients and/or patients with spine metastases (70, 71). Several mechanisms of IESM’s metastatic spread have been suggested, including: hematogenous spread via the arteriovenous system, the Batson’s plexus, or the perineural lymphatic system, cerebrospinal fluid (CSF) dissemination with leptomeningeal spread and drop subarachnoid metastases, and direct invasion from adjacent structures with dural seeding (7, 25). We assumed that the most common origin of non-neurogenic IESMs derives from hematogenous tumor spread, owing to the prevalence (58.5%) of concomitant systemic metastases noted in our pooled patients. Leptomeningeal spread is expected to be more common for the occurrence of neurogenic IESMs from primary central nervous system tumors. However, the high rates of concurrent brain metastases (67.1%) found in this cohort suggest that CSF dissemination may be a common route also for IESMs. Direct tumor invasion with dural seeding has been documented less frequently, especially in patients with melanomas or urologic neoplasm with concurrent vertebral metastases (31, 59). The most common metastatic routes may account for the late onset of IESMs from the diagnoses of primary tumors, as reported across all pooled studies (median 18 months). In some cases, aggressive carcinomas may show different metastatic mechanisms accountable for synchronous IESMs, which characterized the initial clinical event that led to the diagnosis of primary tumors in 16 of our pooled patients (12.3%) diagnosed with late-stage melanoma (53, 54), lung (36, 42), and renal (45, 46) cancers.
Similar to intramedullary spinal cord metastases, most IESMs are symptomatic but non-specific in terms of clinical presentation, causing delay in diagnosis with consequent worsening of patients’ functional status (5, 69). Accurate evaluation of sensorimotor deficits and regional axial pain may assist in localizing affected spine levels, but may be underestimated at early stages in case of lesions with moderate growth and non-severe spinal cord compression (7, 44). As found in this pooled cohort, acute CES has been frequently reported in lesions involving the lumbar-sacral spine, which may facilitate a differential diagnosis with other intramedullary tumors (17, 72). Although CES-related symptoms, such as lumbar or radicular leg pain, and mild motor deficits with preservation of sphincter functions, may simulate lumbar disc diseases, their quick progression may serve as an important red flag mandating further, prompt diagnostic assessments (73). Spine myelography and CT scans were the most commonly used diagnostic tools in early series. Contrarily to intramedullary lesions, spine myelography allowed for the detection of contrast dye block within the spinal canal, suggesting the location and suspicion of IESMs, especially in patients with a known history of cancer (6, 10, 17, 65). The introduction of T1-contrast MRI scans improved the pre-operative diagnostic accuracy, representing the current diagnostic standard. IESMs are frequently identified as single or multiple contrast-enhancing masses located outside the spinal cord and often attached to the dura, causing compression or infiltration of spinal nerve roots particularly when occurring within the conus medullaris (5, 10, 43). MRI and CT may yield low specificity to distinguish primary from metastatic intradural extramedullary lesions, particularly in cases with no prior cancer history (10). However, the importance of early spine imaging relies in clearly distinguishing intramedullary versus extramedullary lesions in patients with non-specific sensorimotor deficits, guiding the design of timely surgical management to avoid irreversible neurological deficits. Furthermore, imaging of the whole spine is also useful to detect concomitant LMs (66) or vertebral metastases (11), offering additional valuable information to plan accurate patient-tailored treatments.
In patients with intradural and extradural spine metastases, the primary treatment goals focus on providing symptom relief with improvement in functional status and/or walking rehabilitation (74). Compared to other spine tumors, such as vertebral metastases, the main difficulties in IESM’s management mostly stem from their complex surgical anatomy, owing to their close relationship with the surrounding spinal cord and spinal nerve roots (5, 6, 11). When feasible, decompressive laminectomy with tumor resection should be performed to confirm the diagnosis and to provide symptom relief (57, 64). However, most IESMs entangle the spinal nerve roots and/or are strictly attached to them, lacking a distinct cleavage plane and posing some risks to cause post-surgical complications when attempting complete tumor resection (1). Similar to a series of patients with intramedullary spinal tumors (69), partial tumor resection was preferred in patients with IESMs, achieving optimal symptom improvement with fewer risks of post-operative neurological complications (57). In some studies, total en-bloc IESMs resection was performed by transecting the infiltrated nerve roots, with no post-operative deficits noted (33, 36, 44, 56). Intraoperative neuromonitoring assistance proved fundamental to evaluate the preserved sensorimotor functions of involved spinal nerves, planning patient-tailored surgical techniques to minimize iatrogenic complications. Similar to other spine metastases, adjuvant treatments have been reported to offer superior survival benefits compared to surgery alone (69, 73). Across our included studies, systemic therapies mostly differed based on primary neoplasms, whereas radiotherapy protocols were mainly consistent. Spine EBRT proved to be effective in patients with metastatic spinal cord compression to reduce post-surgical residual tumor volumes and prolong local control (75). In these pooled patients, locoregional spine EBRT mainly targeted the lesions of interest, but was also extended to other spine regions in case of multiple simultaneous IESMs and/or concurrent vertebral metastases (54, 55, 60). Targeted adjuvant SRS (with a 10 Gy dose) was used in the recent report of Pagano et al. (64) with no radiation-induced adverse events, suggesting the feasibility and safety of this protocol for the management of IESMs. Newer immunotherapy and targeted molecular therapies have been studied and are currently used in the multidisciplinary management of systemic cancers, but their benefits in patients with IESMs have yet to be evaluated (72, 76).
Despite the available therapies, patients with IESMs have poor prognoses, which mainly depend on primary cancer’s histology and treatments (5, 11, 64). Similar to patients with intramedullary metastases (69), the pooled low LC and OS rates in IESMs likely derive from their late-onset and delayed diagnosis, as they have been frequently detected in patients with high tumor burden and multiple systemic metastases. These elements, added to the lack of available systemic therapies selectively directed against IESMs, may account for the differences in survival noted in comparison to patients with vertebral metastases, with OS up to 2 years when receiving immunotherapy or targeted molecular therapies (71). Tumor resection and locoregional radiation were mostly intended for palliation, achieving desirable short-term rates of clinical (70.8%) and radiological (64.2%) improvement, superior than those described in patients with spine LMs (72). Optimal outcomes were obtained by performing decompressive laminectomy and tumor resection in patients with paraparesis and ambulatory difficulty, which led to walking improvement and quality of life amelioration in most cases (27, 65, 67). However, owing to the better prognosis and survival in oncological patients, with the consequent increasing incidence of spine metastases, novel patient-tailored therapies should be developed and evaluated also for IESMs, aimed at reducing patients’ morbidity and improving their quality of life.
Limitations
All included articles were retrospective case reports and small case series, potentially subjected to publication and selection biases. Included articles covered a 40 year time period encompassing major changes in imaging diagnostic tools and available treatments, likely to have generated some between-study heterogeneity in the final analysis. By selectively including only histology-proved cases, this review may have underestimated IESMs’ overall prevalence and related outcomes, accounting for possible detection bias. However, our predetermined inclusion criteria were defined to minimize the risks of introducing confounding variables related to misdiagnoses of IESMs obtained only from clinical and radiological evaluations. Due to the lack of granular data, performance status scores could not be analyzed nor compared pre- and post-treatment. Despite these limitations, we present a methodologically accurate and replicable individual patient data meta-analysis of IESMs to advice clinicians on their management.
Conclusion
Non-neurogenic IESMs may occur at later stages in systemic oncological diseases, determining significant neurological and functional deficits in affected patients. IESMs mostly derive from lung, renal, and breast carcinomas, often causing sensory and motor impairments and acute CES when involving the lumbar-sacral spine. Decompressive laminectomy and tumor resection, in particular if associated with adjuvant locoregional radiation and/or systemic therapies, show good rates of shortterm symptom improvement. However, LC and OS remain discouraging. Future studies are needed to evaluate newer molecular and immune therapies in IESMs’ multimodal management.
Footnotes
Authors’ Contributions
Paolo Palmisciano: Conceptualization, Methodology, Data analysis, Writing - Original draft preparation, Andrew L. Chen: Resources, Writing - Reviewing and Editing, Othman Bin-Alamer: Resources, Writing - Reviewing and Editing, Gianluca Ferini: Resources, Writing - Reviewing and Editing, Mayur Sharma: Resources, Writing - Reviewing and Editing, Giuseppe E. Umana: Resources, Writing - Reviewing and Editing, Salah G. Aoun: Resources, Writing - Reviewing and Editing, Ali S. Haider: Methodology, Resources, Writing - Reviewing and Editing, Supervision.
Conflicts of Interest
The Authors have no relevant financial or non-financial interests to disclose in relation to this study.
- Received May 29, 2022.
- Revision received June 14, 2022.
- Accepted June 15, 2022.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.