


Abstract
Background/Aim: Radiotherapy (RT) related myocardial changes were analyzed by deformation imaging echocardiography in this study. Patients and Methods: Ninety-nine breast cancer patients were studied at baseline, after chemotherapy, after RT, and three years after RT (3Y). Eighty patients received RT only, and twenty patients had right-sided breast cancer. Echocardiography included cyclic variation of the integrated backscatter in the septum (sCV) and posterior wall (pCV), global longitudinal strain (GLS), and left ventricular ejection fraction (LVEF). Results: In patients with left-sided breast cancer, sCV declined from 11.3±3.3 dB at baseline to 10.3±2.9 dB after RT (p=0.001). No changes were observed after chemotherapy (p=0.211) or in patients with right-sided breast cancer after RT (p=0.977). No other parameters declined after RT. The decline in sCV was independently associated with the left anterior descending coronary artery radiation dose (β=–0.290, p=0.020). Conclusion: In contrast to other parameters, sCV correlated with heart radiation dose.
- Radiotherapy
- breast cancer
- myocardial imaging
- cyclic variation of the integrated backscatter
- speckle tracking echocardiography
- global longitudinal strain
Breast cancer is the most common cancer worldwide, with 2.26 million new cases annually (1). With effective screening programs and treatment protocols, breast cancer prognosis has improved, creating a large population of long-term survivors (2). However, adjuvant treatments, especially anthracycline-based chemotherapy and left-sided breast radiotherapy (RT), may induce late adverse cardiovascular effects, which may reduce the overall treatment benefit. In fact, breast cancer patients’ cardiovascular mortality exceeds cancer-related mortality in some breast cancer patient groups (3). This has raised concern regarding treatment-related toxicity and created a need for safer treatment protocols. Knowledge of anthracycline toxicity is comprehensive, but many aspects of RT treatment need further elucidation.
The late effects of RT-induced cardiotoxicity include coronary artery disease, valvular abnormalities, diffuse myocardial fibrosis, conduction and rhythm disorders, pericardial changes, and atherosclerosis (4). Clinical cardiotoxicity appears to have a latency of several years, and knowledge of the early cardiac changes is lacking. The aims of this study were to compare different left ventricular (LV) systolic parameters to evaluate which are the most sensitive for detecting RT-induced early subclinical myocardial changes.
Patients and Methods
Patient selection. This was a single-centre three-year prospective observational follow-up study conducted from May 2011 to June 2016. Eligible female patients with early-stage breast cancer were recruited unless they had other malignancy, severe lung disease, symptomatic heart failure, recent acute myocardial infarction (<6 months), atrial fibrillation, pacemaker, left bundle branch block, severe psychiatric disorder, pregnancy or breast feeding, or were under 18 or over 80 years of age. Overall, ninety-nine breast cancer patients were recruited. The patients were divided into three groups according to their clinical treatment protocols. Chemo patients had left-sided breast cancer treated with adjuvant chemotherapy and thereafter with radiotherapy (n=19). Patients with left-sided breast cancer (left, n=60) and patients with right-sided breast cancer (right, n=20) were treated with adjuvant RT, but they did not receive chemotherapy due to their tumour characteristics. The study complied with the Helsinki Declaration, and the local ethics committee approved the protocol (R11149). All participants signed an informed consent form before enrolment.
Cardiac examinations. All echocardiographic examinations were performed by the same cardiologist (SST) using a Philips iE33 ultrasound machine (Bothell, WA, USA) and a 1-5 MHz matrix-array X5-1 transducer according to a predefined protocol. All offline analyses were performed using Philips Qlab 10.1 software (Philips Qlab). The key systolic parameters were the left ventricular ejection fraction (LVEF) measured using the Simpson method, global longitudinal strain (GLS), and cyclic variation of the integrated backscatter derived from the septum (sCV) and posterior wall (pCV), as explained in detail in our previous publications (5, 6) and shown in Figure 1. Breast cancer patients were examined prior to treatment (baseline), within three days after RT (RT) and three years after RT (3Y). Additionally, chemo patients were examined after chemotherapy but prior to RT.

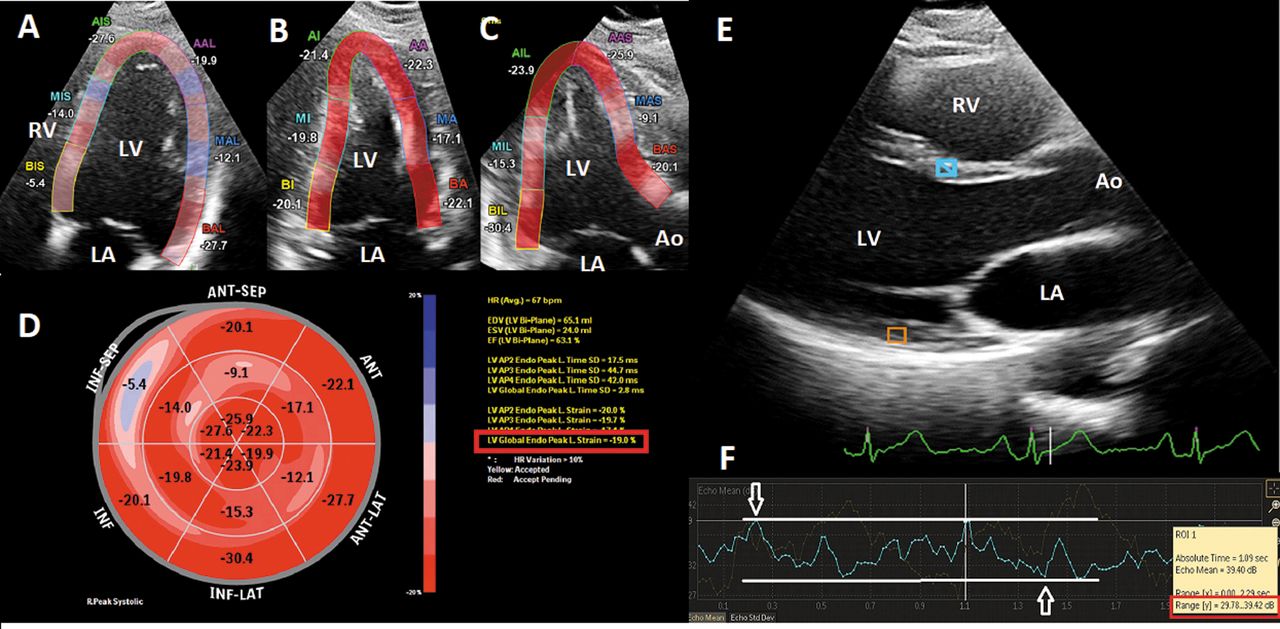
Myocardial deformation imaging. Speckle tracking analysis is displayed on the left side of the image (images A-D) and integrated backscatter on the right side of the image (E-F). Apical four-chamber (A), two-chamber (B), and three-chamber (C) views with colouring indicating the left ventricular regions that were analysed. The regional strain values are shown adjacent to the respective areas and as a bullseye configuration (D). The global longitudinal strain of -19.0% is highlighted with a red box in image D. A parasternal long axis view is shown in image E with regions of interest placed on the septum (blue box) and posterior wall (orange box). The right bottom of the image shows integrated backscatter values of the ROIs during the cardiac cycle. The lowest and highest values for the septal ROI are indicated by the white arrows. The lowest and highest values are highlighted with a red box. The cyclic variation of the septal integrated backscatter is the difference between the lowest and highest values; here, 39.42 dB – 29.78 dB=9.64 dB.
Adjuvant cancer treatment. All breast cancer patients received adjuvant RT according to normal clinical practice. Three-dimensional treatment planning computed tomography (CT) was performed in all patients. According to the CT images, optimal fields and shields were planned to spare the heart from radiation as much as possible. RT was given according to the normal institutional clinical guidelines either for a total of 50 Gray (Gy) with 2 Gy fractions or 42.56 Gy with 2.66 Gy fractions. The radiation doses and adjuvant hormonal therapy are displayed in Table I. Chemo patients were treated with adjuvant chemotherapy prior to RT treatment with 3 cycles of docetaxel and 3 cycles of cyclophosphamide, epirubicin and 5-fluorouracil.
Baseline characteristics.
Statistics. The data are presented as the means with standard deviations (SD) for variables with normal distributions, as medians with quartiles for nonnormally distributed variables, or as numbers with percentages for categorical variables. The baseline differences between groups were tested with the independent samples Kruskal–Wallis test or with the chi-square test when appropriate. To test the within-group measurement changes over time, mixed effect models were used. The patient was treated as a random factor, and the group and time were treated as fixed. A first-order autoregressive covariance structure was used as the structure of the covariation between measures. A multivariable analysis for systolic measurements was performed using linear regression analysis. The included covariants were the mean left anterior descending (LAD) coronary artery radiation dose, age at inclusion, absence of concurrent other diseases, current smoking, chemotherapy, and heart hospitalization during the follow-up period. All p-values are two-sided, and a p-value<0.05 is considered statistically significant. The analysis was performed with IBM SPSS version 25 (Armonk, NY, USA).
Results
General characteristics. The general characteristics of the breast cancer patients are displayed in Table I. Chemo patients were younger (p=0.037), ablation was a more common type of surgery (p<0.001) in these patients, and they used aromatase inhibitors more often (p=0.016) than other patients did. The heart radiation doses were lower in the right patients (p<0.001). All patients except one (99%) completed the three-year follow-up. None of the patients had cancer recurrence during the three-year follow-up time, while eleven patients (11.1%) had cardiac hospitalization due to cardiac problems (Table II).
Major adverse events during the three-year follow-up.
Septal cyclic variation of the integrated backscatter. In the whole group, sCV declined significantly (p<0.001) with an overall decline of 2.6±3.8 dB. The changes in chemo, left, and right patients are displayed in Table III and Figure 2. The associations of the systolic parameters with heart radiation doses are shown in Figure 3. In a univariate analysis of the whole group with clinically significant parameters, the mean LAD dose was significantly associated with sCV decline (β=–0.287, p=0.008). Each Gy into the LAD region worsened the sCV by 0.09 (–0.172, –0.015) during the three-year follow-up. In a multivariable analysis, the mean LAD dose was independently associated with sCV decline (β=–0.290, p=0.020).
Left ventricular systolic function in echocardiography.

Error bar images. The top row presents chemo patients, middle row left patients, and bottom row right patients. Columns from left to right represent the septal cyclic variation, posterior cyclic variation, global longitudinal strain, and left ventricular ejection fraction, respectively. Black asterisks indicate a significant change (p<0.05) after baseline.

The associations of the systolic parameters with heart radiation doses. The left-sided column presents associations with mean radiation dose of the left anterior descending coronary artery (LAD) and the right-sided column presents associations with mean heart radiation dose. From top to bottom, associations with radiation doses for cyclic variation of the integrated back scatter in the septum (sCV) and posterior wall (pCV), for left ventricular ejection fraction (LVEF) and for global longitudinal strain (GLS) can be observed, respectively.
In the chemo patients, no changes in sCV were observed after chemotherapy, but a significant decline in sCV of 2.7±3.9 dB (p=0.014) was found after RT and of 3.6±5.2 dB (p=0.001) at the three-year follow-up. Left patients had a significant decline in the sCV after RT of 1.4±3.5 dB (p=0.011), which persisted through the three-year follow-up (2.4±3.2 dB, p<0.001). Right patients also had a significant sCV decline at the three-year follow-up of 2.0±4.1 dB (p=0.035), but not earlier. In a univariate analysis, chemo patients’ current smoking was associated with sCV changes at the three-year follow-up (β=0.7.988, p=0.047). Chemo patients who smoked (n=3) had an sCV increase of 1.8±5.5 dB (p=0.617) compared to a decline of 4.8±4.5 dB (p=0.002) in non-smokers (n=14). The mean LAD dose was independently associated with the sCV decline in left patients (β=–0.334, p=0.029) in a multivariable analysis.
Posterior cyclic variation of the integrated backscatter. The overall pCV decline in the whole group was 1.4±4.1 dB (p=0.001), with a significant decline appearing at the three-year follow-up. In the univariate analysis with clinically significant parameters, the change in pCV was associated with smoking during RT treatment (β=2.641, p=0.047). Patients who smoked (n=11) during RT treatment had a non-significant increase in pCV of 0.8±4.8 dB (p=0.584), while non-smokers (n=76) had a pCV decline of 1.8±3.9 dB (p<0.001). In the multivariable analysis, the change in pCV had no independent associations.
Chemo patients had no significant overall change (p=0.885), while left patients and right patients had a significant decline in pCV of 1.7±3.5 dB (p<0.001) and 1.9±4.3 dB (p=0.035), respectively, at the three-year follow-up. In the multivariable analysis, a decline in pCV was independently associated with patients with no other concurrent diagnosis (β=–2.173, p=0.045) and with age (β=–0.190, p=0.019) in left patients. There were no significant independent associations in the other groups.
Global longitudinal strain. In the whole group, GLS declined significantly (p=0.011), with an overall decline of 1.1±3.5%. In a univariate analysis with clinically significant parameters, cardiac hospitalizations were significantly associated with GLS decline at the three-year follow-up (β=3.250, p=0.015). Patients with cardiac hospitalizations (n=11) had a higher GLS reduction of 4.1±5.1% vs. 0.8±3.4% in patients without cardiac hospitalization (p=0.015). However, the baseline and post-RT GLS values were not associated with later cardiac hospitalization (β=0.723, p=0.553 and β=1.882, p=0.088, respectively). Patients with a clinically significant cardiac event (n=11) had a baseline GLS of –17.3±4.2% vs. a baseline GLS of –18.1±3.2% in patients with an event-free follow-up (n=82, p=0.553). However, at the three-year follow-up the GLS was –13.3±2.7% vs. –17.4±2.7% (p<0.001) in patients with and without cardiac hospitalization, respectively. In the multivariable analysis, the GLS decline was independently associated with the clinical incidence of cardiac hospitalizations (β=–3.360, p=0.036).
Chemo and right patients displayed no significant difference in GLS during the follow-up. Left patients had a significant change in GLS at the three-year follow-up of 1.7±3.5% (p<0.001). In a univariate analysis, the change in GLS was associated with concurrent smoking (β=–7.824, p=0.014) in right patients and with cardiac hospitalization (β=–3.679, p=0.008) in left patients. Left patients with cardiac hospitalization during the three-year follow-up had a GLS decline of 4.9±5.0, while patients without cardiac hospitalization had a GLS decline of 1.2±3.0% (p=0.008). In the multivariable analysis, the change in GLS was independently associated with cardiac hospitalizations in left patients (β=–3.625, p=0.028) and with smoking in right patients (β=–8.152, p=0.019). Right patients who smoked (n=2) during RT treatment had a GLS decline of 7.0±5.7%, while non-smokers (n=17) had a GLS increase of 0.8±3.7% (p=0.014).
LVEF by the Simpsons method. LVEF declined significantly during the three-year follow-up (p<0.001), with an overall decline of 4.8±9.3%. There was no change from baseline to chemotherapy (p=0.221) or to RT (p=0.735). There were no factors associated with the LVEF decline either in univariate analysis or in multivariable analysis.
Chemo patients displayed no significant LVEF changes during the three-year follow-up (p=0.138), while left patients (p<0.001) and right patients (p=0.013) had a significant decline at the three-year follow-up of 5.2± 9.8% (p<0.001) and 4.8±9.5% (p=0.020), respectively. There were no factors associated with the LVEF decline in univariate or multivariable analyses.
Other conventional echocardiography parameters. The results for other conventional echocardiography parameters are displayed in Table IV. Right ventricular systolic function deteriorated transiently in chemo and left patients after RT by 2.5±3.9 mm (p=0.018) and 2.0±3.1 mm (p=0.030), respectively. All patients also experienced transient changes in LV mass of 9.0±22.8 g (p=0.035) and a late decline in the mitral E-wave of 6.8±13.3 cm/s (p=0.018) in right patients and an increase in the tricuspid gradient by 1.7±6.7 mmHg (p=0.002) in chemo patients and by 2.0±5.4 mmHg (p=0.005) in left patients at the three-year follow-up.
Other echocardiographic measurements.
Discussion
The GLS is considered to be an early sensitive marker of myocardial disorder over a wide range of cardiac conditions (7-9). However, our study shows that CV analysis might be even better and more specific for revealing early RT-related myocardial changes. This may have clinical implications for the surveillance and diagnosis of RT-treated patients as well as for RT treatment adjustment to a safer protocol.
Changes in LV systolic function after RT. In the assessment of cardiac function and disorders, one of the most important tasks is the determination of left ventricular systolic function. From several echocardiographic parameters, LVEF is most commonly used. However, in many cases with gradual worsening of LV function, a drop in the LVEF appears late and beyond the effective therapeutic window. To detect pathological changes before irreversible damage occurs, more sensitive methods are urgently needed. Direct myocardial deformation imaging, such as strain in speckle tracking echocardiography and CV measurements, might be better tools for this purpose.
In our study, LVEF declined at the three-year follow-up by 4.8±9.3% (p<0.001), which is below the level of variability and below what is usually considered clinically meaningful (10). sCV measurements showed an earlier decline than LVEF and GLS, and it was the only measurement associated with the radiation doses. sCV showed a decline immediately after RT in left-sided breast cancer patients (chemo and left), whereas the right-sided breast cancer patients and the posterior parts of the heart (pCV) had a late decline at the three-year follow-up.
Cyclic variation of the integrated backscatter. The molecular basis for the changes in the integrated backscatter (IBS) measurement is unclear, but it seems that the differences between the intra- and extra-cellular contents are central (11). In endomyocardial biopsies, increased values have been correlated with diffuse myocardial fibrosis and with increased myocardial collagen content (12-14). Cyclic variation of the IBS measures the difference between the highest and lowest values through the cardiac cycle, and is considered to reflect myocardial intrinsic contractility (15, 16). It is unclear whether the CV reflects cyclic changes in the myocardial fibres or other structures in a three-dimensional orientation. In several studies, the CV has not been associated with structural changes, and it has been speculated that the CV reflects other myocardial qualities (13, 17, 18).
Micardi et al. manipulated canine cardiac circulation with adenosine and partial stenosis in coronary arteries without affecting myocardial contractility (19). Adenosine increases blood volume in the small vessels by inducing vasodilatation, while partial epicardial stenosis depletes blood volume. The small myocardial arteria are filled during diastole and emptied during systolic myocardial contraction. With vasodilatation, the difference in myocardial blood volume between diastole and systole is increased, and with stenosis, it is decreased. As the CV increased with adenosine and decreased with epicardial stenosis, it was concluded that the CV has a close association with myocardial blood filling and with the number of patent myocardial microvessels (19). RT is known to cause rarefication of the myocardial capillaries and myocardial perfusion defects as an early phenomenon, which persists and increases with longer follow-up times (20-24). As myocardial capillary rarefication is one of the key RT-induced myocardial features, CV measurement might be a precise method to detect RT-induced changes in the heart. The sCV was measured in parasternal images of the left ventricular septum corresponding to the anteroseptal area of the LV, i.e., the area covered by the LAD coronary artery and, on the other hand, the area with the highest radiation doses in left-sided breast cancer patients, as shown by Taylor et al. (25). This might explain why in patients with left-sided breast cancer, RT caused changes in the sCV at the post-RT timepoint. Furthermore, the changes were associated with the mean LAD radiation dose, while spared posterior parts were not associated. In general, cardiac radiation exposure is significantly smaller in right-sided breast cancer patients than in those with left-sided cancer. This might explain why patients with right-sided breast cancer did not display significant changes in sCV after RT.
GLS and clinical events. Eleven patients (11.1%) were hospitalized due to cardiac problems during the three-year follow-up. Considering the variety of cardiac diagnoses and the relatively short time interval between RT and hospital admission, it is unlikely that the events were caused solely by adjuvant treatments. The decline in GLS was larger among patients with adverse cardiac events than that among those with no adverse events during the follow-up. However, it is probable that the GLS change was a consequence rather than a predictor of adverse cardiac events considering that the baseline or post-RT GLS was not associated with cardiac hospitalization.
Smoking. Concurrent smoking during cancer therapies has been associated with worse locoregional cancer control and decreased cancer-specific survival (26-30), but RT-related adverse events are also decreased (31). Thus, it has been suggested that smoking reduces the RT-induced tissue inflammatory response by suppressing effector cells. Additionally, smoking suppresses tissue oxygenation by inducing hypoxia through increased levels of carboxyhaemoglobin and vasoconstriction (27, 28, 31-33). It seems that concurrent smoking during treatment reduces the overall tissue effects of RT, which leads to therapeutic failure and reduces adverse cardiac effects (31).
In our study, the effects of smoking on the CV and GLS were strikingly different. Smokers and non-smokers had a significant difference in their CV changes during the three-year follow-up. Non-smokers had a reduction in sCV (chemo) and pCV (all patients), whereas smokers had either stable or even increasing CV values. In contrast to the smoking effects on CV, smokers in the right group had a reduction in GLS compared to the stable value in non-smokers, although the number of smokers was small. This difference may implicate that CV measurement reflects better RT-induced tissue effects, while the GLS is more closely related to the overall negative effects that smoking has on cardiovascular health. Smoking during therapy reduces tissue effects, which might explain why non-smokers had a reduction in the CV value and thus a higher tissue impact of the RT, while smokers did not have a decline in their CV values (31).
Other conventional echocardiography. The LV mass increased after RT with a subsequent normalization, most likely reflecting the early inflammatory myocardial oedema at the post-RT timepoint. At the longer follow-up, there were changes in diastolic parameters, such as a decline in mitral E in right patients and an increase in the tricuspid gradient in left-sided breast cancer patients (chemo and left), while the initial changes in TAPSE were transient.
Clinical implications. Early detection of adverse effects would allow us to use timely therapeutic interventions and prevent further damage. Our study indicates that CV analysis is closely correlated with RT-induced myocardial changes, and it might be a sensitive and specific tool for the detection of early RT-induced myocardial capillary rarefication and myocardial fibrosis. Its diagnostic power seems to surpass other systolic parameters, such as LVEF and GLS.
Limitations. This study has several limitations. No control group was included, and hence, confounding factors could have contributed to our results. The size of the study groups was uneven, and the baseline characteristics of the patients were not fully comparable, which may have influenced the results. Additionally, the analysis of patients’ smoking habits did not include factors such as pack years or possible passive smoking. Furthermore, this study was not powered to detect differences according to clinical cardiac events or smoking habits. Therefore, larger studies with adequate powering are needed. Finally, the follow-up time was short considering the late-appearing adverse RT-related cardiac effects. A longer follow-up of this patient group is ongoing for this purpose.
New piece of evidence. The ability of the CV analysis to reveal RT-induced functional myocardial changes seems to be superior compared to GLS and LVEF measurements. It may facilitate the evaluation of patients after RT and may serve as an accurate tool in the improvement of RT safety protocols.
Acknowledgements
This study was supported by nonprofit trusts: Paavo and Eila Salonen Legacy, Aarne Koskelo Legacy and Georg and Ella Ehrnroot Trust (Helsinki, Finland). The Authors would also thank the research nurses Virpi Palomäki, Hanna-Leena Näppilä, Kati Helleharju and Katri Mikkonen for their expert assistance during the study.
Footnotes
Authors’ Contributions
All the Authors have contributed significantly to the concept design of this manuscript and the work leading to the final manuscript. All Authors have reviewed the article and agreed with its content.
Conflicts of Interest
The Authors have no conflicts of interest to declare regarding this study.
- Received December 20, 2021.
- Revision received March 27, 2022.
- Accepted March 28, 2022.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).





{kind=link}
{kind=link}
{kind=link}