


Abstract
Background/Aim: The TP53-signature is a multi-gene signature that can predict TP53 structural mutations. It has presented remarkable ability to predict the prognosis of early-stage breast cancer. However, some samples presented discordance with the signature status and structure status. We aimed to investigate whether the mRNA expression levels or copy number variation (CNV) of MDM2 and CDKN2A influence the TP53-signature-score, subtype classification, and prognosis prediction in TP53 wild-type, luminal type early-stage breast cancer samples. Materials and Methods: We selected TP53 wild-type, luminal type early-stage breast cancer samples from The Cancer Genome Atlas (TCGA) and Molecular Taxonomy of Breast Cancer International Consortium (METABRIC) cohorts. Then, we analyzed the correlation between the TP53-signature-score and mRNA expression levels or CNV of MDM2 and CDKN2A. Results: The samples with MDM2 copy number (CN) amplification or those with CDKN2A CN deep deletion presented higher TP53-signature-score. Moreover, samples with MDM2 CN amplification or those with CDKN2A CN deep deletion had more characteristics of the luminal B type. In addition, they showed lower estrogen response early score, which correlated with response to endocrine therapy in breast cancer. However, MDM2 and CDKN2A mRNA expression did not present the same tendency. Furthermore, samples with MDM2 CN amplification or those with CDKN2A CN deep deletion had a worse prognosis in METABRIC cohort. Conclusion: The MDM2 or CDKN2A CNV may be useful for classifying subtypes and predicting prognosis more accurately in TP53 wild-type, luminal type early-stage breast cancer patients.
Breast cancer is the most common occurring cancer among women worldwide. The subtype classification of breast cancer plays a pivotal role in its treatment and the prediction of prognosis.
Breast cancer can be divided into luminal, human epidermal growth factor receptor 2 (HER2)-like, and Basal-like subtypes based on the immunohistochemical (IHC) status of estrogen receptor (ER), progesterone receptor (PgR), HER2, and Ki-67 clinically (1). Luminal type can be further divided into luminal A and luminal B. Luminal A type is both ER and PgR positive, HER2-negative, with low expression levels of the protein Ki-67. On the other hand, luminal B type is ER-positive, either PgR- and HER2-positive or -negative, with high expression levels of Ki-67 (1).
Several multi-gene signatures have been developed to predict prognosis and classify the breast cancer subtypes more accurately, like OncotypeDX, MammaPrint, and PAM50 (2-4). Among them, PAM50 can divide breast cancer into Luminal A, Luminal B, Normal-like, HER2-enriched, and Basal-like, five intrinsic subtypes with fifty genes, more accurately than IHC classification (5).
Luminal type patients are treated mainly with endocrine therapy clinically, and have a better prognosis than patients with other subtypes (6). However, luminal B type has a worse prognosis and is less sensitive to endocrine therapy than luminal A type (7, 8).
TP53 is a tumor suppressor gene, which encodes the p53 protein. p53 can regulate the expression of various downstream genes to maintain genomic stability (9). Mutations in TP53 can be found in the majority of solid tumors, and are correlated with tumorigenesis, tumor progression, and poor prognosis (10). The TP53-signature was constituted by differentially expressed genes (DEGs), which can predict the TP53 structural mutation in the breast cancer cohort (11).
Yamaguchi et al. demonstrated that the TP53-signature-score had a remarkable ability to predict the prognosis of early-stage breast cancer compared to other pre-existing multi-gene signatures (12). They indicated that TP53 structure mutated samples presented higher TP53-signature-score and defined them as TP53-signature mutant type. Interestingly, some patients presented with TP53-signature mutant type, although their TP53 structure was wild type. This discordance was mainly observed in luminal B type samples, which were classified using PAM50, and in some patients who had MDM2 mRNA over-expression.
MDM2 encodes an E3 ubiquitin ligase, MDM2 protein, which plays a critical role in regulating the normal function of p53 (13). It has been well studied that MDM2 and p53 form a negative feedback loop (14).
CDKN2A encodes p14ARF and p16INK4A proteins. Among them, p14ARF has been reported to bind to MDM2 and suppress its E3 ubiquitin ligase function, thereby stabilizing p53 (15). In addition, CDKN2A copy number (CN) loss and MDM2 CN amplification are mutually exclusive (16).
Although MDM2 and p14ARF can modulate the activity of p53, the relationship between the TP53-signature and MDM2 or CDKN2A remains unknown, because not all genes in the TP53-signature are downstream genes of p53.
In this study, we aimed to analyze whether MDM2 or CDKN2A mRNA expression levels or CNV influence the TP53-signature, and whether MDM2 or CDKN2A mRNA expression levels or CNV influence the features of luminal types and prognosis in The Cancer Genome Atlas (TCGA) and Molecular Taxonomy of Breast Cancer International Consortium (METABRIC) cohorts.
Materials and Methods
Clinical and transcriptomic data collection for breast cancer patients. TCGA (17) and METABRIC (18, 19) data were obtained from cBioportal (20, 21). We chose the female breast cancer patients who presented with TP53 structure wild type and early-stage luminal A or luminal B type from TCGA (n=189) and METABRIC (n=596) cohorts (Table I). In the downloaded clinical data, luminal A type and luminal B type were classified using the PAM50 method.
Clinical characteristics of the samples analyzed.
Estimation of the TP53-signature-score and estrogen response early score. Expression data of the thirty-one genes comprising the TP53-signature were obtained from TCGA and METABRIC (Supplementary Figure S1). The TP53-signature-score was calculated using a previously described method (12). The estrogen response early score was calculated using the method described before that employed R package “GSVA” (22-24).
Definition of CNV. The CNV in TCGA and METABIC cohorts analyzed were displayed as -2, -1, 0, 1, and 2. Following the instructions in cBioportal, we defined “-2” as deep deletion, “-1” as loss, “0” as diploid, “1” as low-levels gain, and “2” as amplification (25).
Statistical analysis. The Spearman’s rank correlation test was used to compare the relationship between the mRNA expression levels and signature score. The absolute values of rs>0.2 were defined as significantly correlated. Kruskal–Wallis test and Mann–Whitney U-test were used to compare group means. The p-value of the Kaplan– Meier survival curves was calculated using the log-rank test. Fisher’s Exact test was used for statistically analyzing patients’ characteristics except for age. All statistical tests were performed using R software (version 4.0.1) and EZR software (26). All plots were constructed by using the EZR software. A p-value less than 0.05 was considered statistically significant. Statistically significant results are shown in bold in figures and tables.
Results
MDM2 and CDKN2A mRNA expression levels were not significantly correlated with the TP53-signature-score or the features of luminal B type. To determine whether MDM2 or CDKN2A mRNA expression levels influence the TP53-signature-score, we analyzed the correlation between the TP53-signature-score and the mRNA expression levels of MDM2 and CDKN2A. We found that neither MDM2 nor CDKN2A mRNA expression levels showed a significant correlation with the TP53-signature-score (Figure 1A-D).

Correlation between TP53-sigature-score and the mRNA expression levels of MDM2 and CDKN2A. Correlation plots of the TP53-signature-score with the mRNA expression levels of MDM2 and CDKND2A in TCGA (A, B) and METABRIC (C, D) cohorts. p-Values were calculated using the Spearman’s rank correlation coefficient.
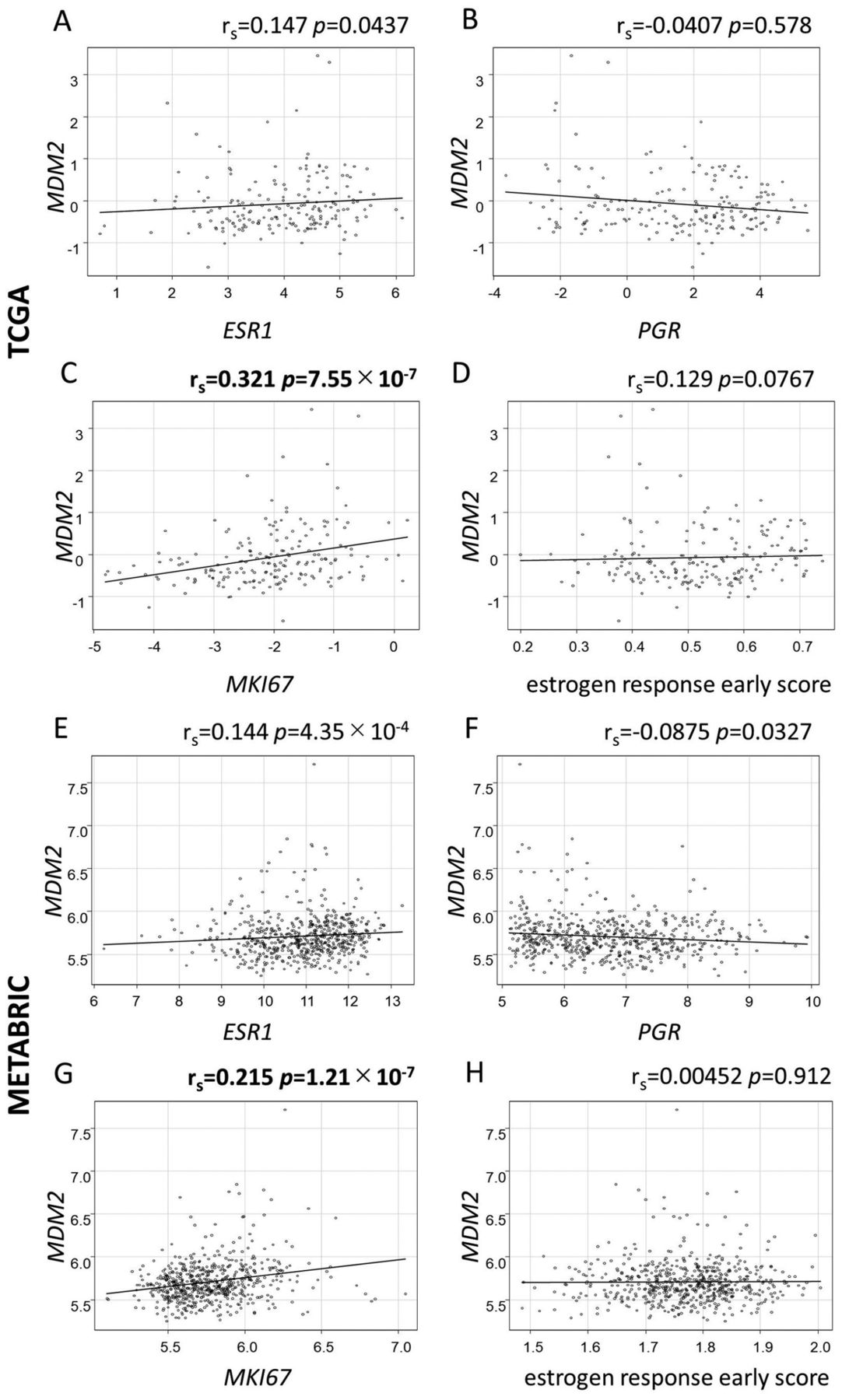
To study whether MDM2 and CDKN2A mRNA expression levels influence the features of luminal B types, we analyzed the correlation between MDM2 or CDKN2A mRNA expression levels and those of ESR1, PGR, and MKI67 mRNA expression levels, which encode ERα, PgR, and Ki-67, respectively (27). We found that MDM2 mRNA expression levels were not correlated with those of ESR1 or PGR mRNA expression levels (Figure 2A, B, E and F). However, MDM2 mRNA expression levels had a weak, positive correlation with those of MKI67 mRNA expression levels (Figure 2C and G). We also analyzed the relationship between the MDM2 mRNA expression levels and estrogen response early score, as it has been previously reported that a lower score may indicate resistance to endocrine therapy (20). We found that MDM2 mRNA expression levels were not significantly correlated with estrogen response early score (Figure 2D and H).

Correlation between MDM2 mRNA expression levels and the mRNA expression levels of ESR1, PGR, MKI67, and estrogen response early score. (A-C, E-G) Plots showing correlations between MDM2 mRNA expression levels and those of typical genes for luminal type (ESR1, PGR, MKI67) in both TCGA and METABRIC cohorts. (D, H) Plots showing correlations between MDM2 mRNA expression levels and the estrogen response early score. p-Values were calculated using Spearman’s rank correlation coefficient.
In TCGA cohort, CDKN2A mRNA expression levels presented a weak, negative relationship with those of ESR1 mRNA expression levels, but not in METABRIC cohort (Figure 3A and E). In addition, CDKN2A mRNA expression levels were not correlated with those of PGR or MKI67 mRNA expression levels (Figure 3B, C, F and G). CDKN2A mRNA expression levels were not correlated with estrogen response early score in neither TCGA nor METABRIC cohorts either (Figure 3D and H).
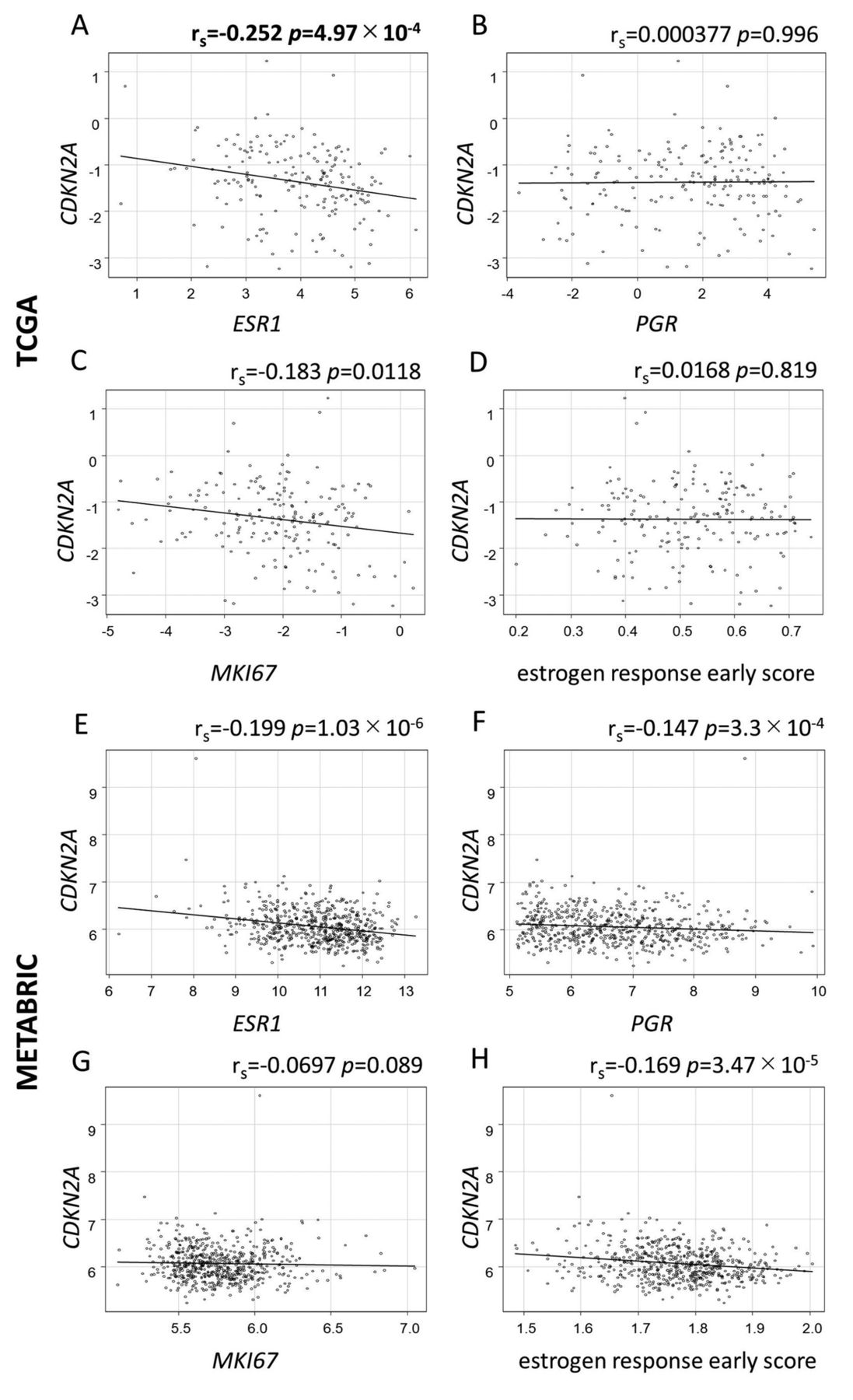
Correlation between CDKN2A mRNA expression levels and the mRNA expression levels of ESR1, PGR, MKI67, and estrogen response early score. (A-C, E-G) Plots showing correlations between CDKN2A mRNA expression levels and those of typical genes for luminal type (ESR1, PGR, MKI67) in both TCGA and METABRIC cohorts. (D, H) Plots showing the correlations between CDKN2A mRNA expression levels and the estrogen response early score in both TCGA and METABRIC cohorts. p-Values were calculated using Spearman’s rank correlation coefficient.
MDM2 and CDKN2A CNV were correlated with the TP53-signature-score and the features of luminal B type. We analyzed whether MDM2 and CDKN2A CNV influence the TP53-signature-score. In our results, samples with MDM2 CN amplification or those with CDKN2A CN deep deletion presented higher TP53-signature-score than other CNV samples (Figure 4A-D).

The TP53-signature-score is associated with the CNV of MDM2 and CDKN2A. (A, C) Boxplots of the comparison of the TP53-signature-score with the MDM2 CNV [(2) amplified, (1) gain, (-1, 0) not amplified] in both TCGA and METABRIC cohorts. (B, D) Boxplots of the comparison of the TP53-signature-score with the CDKN2A CNV [(-2) deep deletion, (-1) loss, (0, 1, 2) not deleted] in both TCGA and METABRIC cohorts. p-values were calculated using Kruskal–Wallis test and Mann–Whitney U-test. CNV: Copy number variation.
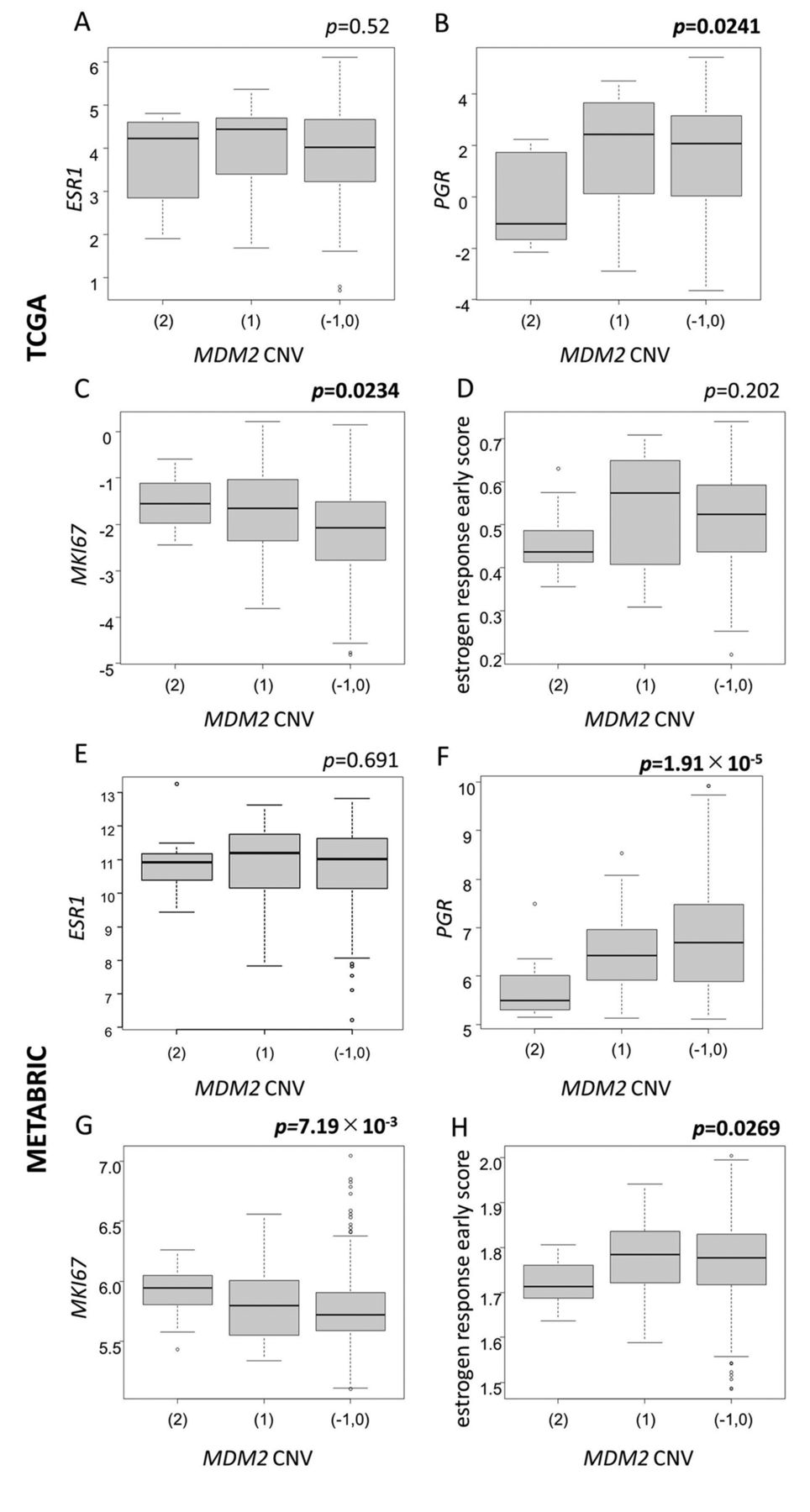
There were no significant differences regarding ESR1 mRNA expression levels (Figure 5A and E). However, the samples with MDM2 CN amplification presented lower PGR mRNA expression levels (Figure 5B and F) and higher MKI67 mRNA expression levels (Figure 5C and G). Estrogen response early score was lower in the samples with MDM2 CN amplification in both TCGA and METABRIC cohorts, and was statistically significant in the METABRIC cohort (Figure 5D and H).

The association between the MDM2 CNV and the mRNA expression levels of ESR1, PGR, MKI67, and estrogen response early score. (A-C, E-G) Boxplots of the comparison of typical genes for luminal type (ESR1, PGR, MKI67) with the MDM2 CNV [(2) amplified, (1) gain, (-1, 0) not amplified] in both TCGA and METABRIC cohorts. (D, H) Boxplots of the comparison of the estrogen response early score with the MDM2 CNV [(2) amplified, (1) gain, (-1, 0) not amplified] in both TCGA and METABRIC cohorts. p-Values were calculated using Kruskal–Wallis test and Mann–Whitney U-test. CNV: Copy number variation.
The samples with CDKN2A CN deep deletion presented higher ESR1 mRNA expression levels in TCGA cohort, but not in METABRIC cohort (Figure 6A and E). They also presented lower PGR mRNA expression levels, but not higher MKI67 mRNA expression levels (Figure 6B, C, F and G). The samples with CDKN2A CN deep deletion also presented lower estrogen response early score, but there were no statistically significant differences (Figure 6D and H). These results indicated that samples with MDM2 CN amplification or those with CDKN2A CN deep deletion defines better the luminal B type than their mRNA expression levels. These samples may present resistance to endocrine therapy.

Association between the CDKN2A CNV and the mRNA expression levels of ESR1, PGR, MKI67, and estrogen response early score. (A-C, E-G) Boxplots of the comparison of typical genes for luminal type (ESR1, PGR, MKI67) with the CDKN2A CNV [(-2) deep deletion, (-1) loss, (0, 1, 2) not deleted] in both TCGA and METABRIC cohorts. (D, H) Boxplots of the comparison of the estrogen response early score with CDKN2A CNV [(-2) deep deletion, (–1) loss, (0, 1, 2) not deleted] in both TCGA and METABRIC cohorts. p-Values were calculated by Kruskal–Wallis test and Mann–Whitney U-test. CNV: Copy number variation.
Samples with MDM2 CN amplification or those with CDKN2A CN deep deletion had worse prognosis. We compared the overall survival in TCGA and METABRIC cohorts with MDM2 and CDKN2A CNV.
In the METABRIC cohort, the Kaplan–Meier survival curves revealed that samples with MDM2 CN amplification or those with CDKN2A CN deep deletion presented worse prognosis (Figure 7A and B). The results of the samples with MDM2 CN amplification were consistent with those in previous reports (28, 29).

The Kaplan–Meier survival curves of MDM2 and CDKN2A CNV in METABRIC cohort. (A) Kaplan–Meier survival curves for overall survival between MDM2 CN (2) amplified (black), (1) gain (red), and (-1,0) not amplified (green). (B) Kaplan–Meier survival curves for overall survival between CDKN2A CN (-2) deep deleted (black), (-1) loss (red), and (0, 1, 2) not deleted (green). p-Values were calculated using the log-rank test. CNV: Copy number variation; CN: copy number.
However, there were no statistically significant differences in the median cut-off values of MDM2 and CDKN2A mRNA expression levels (Supplementary Figure S2A-D). About 10% of the samples had MDM2 CN gain and amplification in the METABRIC cohort, and 15% in the TCGA cohort (Supplementary Table S1 and Table S2). Therefore, we defined the samples with the top 10% and 15% of high MDM2 mRNA expression as the high group and the others as the low group, and then compared their overall survival. However, no significant differences were found (Supplementary Figure S3A-D). Regarding the inconsistent results of MDM2 mRNA expression levels and CNV, we found that some samples presented higher mRNA expression levels with CN not amplified, however, MDM2 mRNA expression levels were comparable with the CNV in most of the samples (Supplementary Figure S4A, B).
About 15% of the samples had CDKN2A CN loss and deep deletion in the METABRIC cohort, and 20% in TCGA cohort (Supplementary Table S1 and Table S2). Therefore, we defined the samples with the bottom 15% and 20% of low CDKN2A mRNA expression as the low group and the others as the high group, and then compared overall survival between these two groups. There were no statistically significant differences in TCGA cohort (Supplementary Figure S5A, C). However, the low group presented poor prognosis in METABRIC cohort (Supplementary Figure S5B, D).
Discussion
In this study, we demonstrated that the CNV of MDM2 or CDKN2A, but not their mRNA expression levels were correlated with the TP53-signature-score.
We also demonstrated that the samples with MDM2 CN amplification or those with CDKN2A CN deep deletion presented more characteristic of luminal B type than their mRNA expression levels. Especially, the samples with MDM2 CN amplification presented statistical significantly lower estrogen response early score in METABRIC cohort. A previous report demonstrated that MDM2 can degrade ERα (30). According to this relationship between MDM2 and ERα, we assumed that the amplified functional MDM2 destroys the ERα and results in a decrease in the dependency of the ER signal.
In regards to the inconsistent results of MDM2 mRNA expression levels and CNV, the splice variants of MDM2 were considered. It has been reported that MDM2 has several types of splice variants, and some of them have distinct functions from full-length MDM2 (31-33). However, many MDM2 splice variants functions are still not yet completely understood. Therefore, further research is required.
In contrast to MDM2, the CDKN2A mRNA expression levels presented the same tendency with their CNV to some extent. However, these results indicate that it is exceedingly difficult to set a common cut-off value for mRNA expression levels in clinical settings with different cohorts.
As this was a retrospective study, there are also some limitations. The major limitation was that we analyzed only two big cohorts. Moreover, the proportion of the samples that presented MDM2 CN amplification or CDKN2A CN deep deletion was less than 5%, therefore, the available data were limited.
Despite the small number of samples with MDM2 CN amplification or CDKN2A CN deep deletion, they are still worth measuring. Especially samples with MDM2 CN amplification have been reported to be correlated with a worse outcome after immune checkpoint inhibitor treatment in a pan-cancer analysis (34). We believe that they should be one of the indicators for considering a treatment plan more accurately.
In conclusion, our results demonstrated that the MDM2 or CDKN2A CNV may be more useful than their mRNA expression levels for classifying the subtypes and predicting the prognosis more accurately in TP53 wild-type, luminal type early-stage breast cancer patients.
Acknowledgements
This work was carried out (in part) at the Intractable Disease Research Center, Juntendo University, Tokyo, Japan. The Authors thank the Laboratory of Molecular and Biochemical Research, Biomedical Research Core Facilities, Juntendo University Graduate School of Medicine, Tokyo, Japan for technical assistance.
Footnotes
Authors’ Contributions
Min Han: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Validation, Visualization, Writing - original draft; Shigeo Yamaguchi: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – review & editing; Mai Onishi: Formal analysis, Software, Writing – review & editing; Tomoaki Fujii: Methodology, Resource, Writing – review & editing; Masaki Hosoya: Formal analysis, Writing – review & editing; Xuan Wen: Writing – review & editing; Hidenori Kido: Writing – review & editing; Shunsuke Kato: Conceptualization, Project administration, Writing – review & editing.
Supplementary Material
Supplementary material can be obtained at: <https://www.dropbox.com/sh/ndv7g89vuxnw0hs/AABkq7LPZUU-bOxJ2GQ7DvDoa?dl=0>
Conflicts of Interest
The Authors declare no conflicts of interest in relation to this study.
- Received February 25, 2022.
- Revision received March 16, 2022.
- Accepted March 18, 2022.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.