


Abstract
Background/Aim: To review the current literature on pineal region gliomas, summarizing the clinical characteristics and treatment outcomes. Materials and Methods: PubMed, Scopus, and Cochrane databases were used to identify relevant articles. Comprehensive clinical characteristic review and survival analysis were conducted. Results: Twelve studies describing 81 patients were included. The median age was 39 years (male=54.3%). Fifty patients (61.7%) had obstructive hydrocephalus requiring cerebrospinal fluid diversion with either ventriculoperitoneal shunt (VPS) (40.0%) or endoscopic third ventriculostomy (ETV) (24.0%). Patients who underwent VPS had significant survival benefits compared to ETV (p<0.05). All patients in our review underwent surgery, and gross-total resection (≥98%) was achieved in 34.6%. The supracerebellar infratentorial approach was the most employed surgical approach (62.3%). Chemotherapy was administered in 32.1% of cases, and radiotherapy in 40.7%. The median overall survival (OS) was 12 months, and the overall one-year survival rate was 60%. Conclusion: This study could not establish a correlation between the extent of tumor resection and positive treatment outcomes. However, among cases with hydrocephalus, patients who underwent VPS placement had better survival as compared to ETV.
Pineal region gliomas are rare neoplasms with variable malignant activity, representing 14-22% of all pineal region tumors. Typically, they arise from the glial stroma of the pineal gland and its surrounding structures (1). Due to their invasive behavior in an anatomically complex region, pineal region gliomas (PRGs) can be challenging to manage and can have poor outcomes (2). Although survival data on gliomas affecting the Central Nervous System (CNS) have been examined, studies scoping in on survival outcomes of PRGs along with the effects of various relevant therapeutic strategies are largely absent in the literature (3).
As a result of PRGs paucity, a consensus standard of care has not been established, leading to various oncological diagnostic protocols and management strategies that have been practiced without unity (4-7). Current diagnostic workup primarily constitutes radiological modalities, such as MRI, for preliminary diagnosis and subsequent intraoperative histological examination for definitive diagnosis (8, 9). In combination with chemoradiotherapy, surgery remains the cornerstone treatment strategy, and several surgical techniques and approaches have evolved to maximize safe tumor resection (10-14).
Although it is a general assumption that the extent of resection and chemoradiotherapy correlate with survival rate, only a handful of case reports and series have studied these questions (4, 15-17). This study reviews the current literature regarding the clinical management of pineal region gliomas, focusing on clinical characteristics, treatment strategies, and survival outcomes.
Materials and Methods
Literature search. A systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (18). PubMed, Scopus, and Cochrane databases were searched from inception to December 2020. A medical subject headings (MeSH) term and keyword search of each database was conducted using the Boolean operators OR and AND. The terms used were as follows: “pineal” and “glioma.”
Study selection. Pre-established inclusion and exclusion criteria were followed. Studies were included with the following criteria: 1) were prospective or retrospective studies involving more than one glioma patient; 2) contained patients aged 18 years or older with histologically confirmed glioma involving the pineal region. Studies were excluded with the following criteria: 1) were meta-analyses, reviews, editorials, letters, or books; 2) contained insufficient clinical data (lacking two of the following: patient demographics, specific histological grading, typing, management and/or outcomes); 3) were not written in English.
Two authors (SR and OBA) independently assessed the titles and abstracts of all extracted papers based on the inclusion and exclusion criteria. Studies that met inclusion criteria were then further evaluated independently with full text review by the same two authors, and disagreements were resolved via a third author (ASH). References of the included articles were also screened to retrieve additional relevant articles.
Data extraction. Data from included studies were extracted by one author (OBA) and confirmed independently by two other authors (ASH and PP) to ensure accuracy. Extraction variables included: authors, date of publication sample size, patients’ age and gender, presenting symptoms, histological and radiological features, management course, treatments (i.e., radiotherapy, chemotherapy, or surgical approach), recurrence, and survival. Missing data are either not reported by the author or reported indistinctively with other data that could not be differentiated.
Data synthesis. The primary outcomes of interest were the clinical features, management course, and survival analysis of pineal region gliomas. Meta-analysis was precluded due to heterogeneity in outcome measures and the limited number of studies. For each study, the level of evidence was assessed using the 2011 Oxford Centre For Evidence-Based Medicine guidelines, and the risk of bias was evaluated with the Joanna Briggs Institute (JBI) checklists for case series (19, 20).
Statistical analysis. Means and ranges were used to summarize continuous variables, while frequencies and percentages were used to summarize categorical variables. Overall survival (OS) and progression-free survival (PFS) were illustrated using Kaplan–Meier curves. The log-rank test was used to compare survival curves. A two-sided p-value <0.05 was considered significant for all analyses. Analyses were performed using the statistical software SPSS v. 25 (IBM Corp, Armonk, New York, NY, USA).
Results
Study selection. The initial literature search yielded 517 citations from PubMed, 654 from Scopus, and 5 from Cochrane (Figure 1). After eliminating duplicates, there were 898 articles. Seven hundred and forty-two studies were excluded based on title and abstract. One hundred and fifty-six full-text articles were then evaluated for inclusion. Of these, 144 papers did not meet inclusion criteria and were subsequently excluded. Twelve articles were included in this systematic review, all categorized as level IV evidence (Table I and Table II) (4, 15, 21-30).

PRISMA flowchart illustrating the search strategy and data selection based on the inclusion and exclusion criteria.
Overview of the clinical characteristics of all included studies.
Overview of the management details of all included studies.
Demographics and clinical characteristics. A total of 81 pineal region gliomas, with slight male predominance (54.3%), were included (Table III). Age ranged from 18 to 82 years old, with a median of 39 years. Headache was the main presenting symptom (20.0%) followed by decreased visual acuity (16.9%) and nausea/vomiting (13.8%). Additionally, 50 patients had hydrocephalus, of whom 64.0% underwent shunting procedures. The Karnofsky Performance Status (KPS) was reported in 22 patients. The pre-operative and post-operative KPS were equal (KPS=60%), yet post-operative status was reported in only one case (KPS=60%).
Summary of clinical characteristics, management strategies and outcomes of all pooled patients.
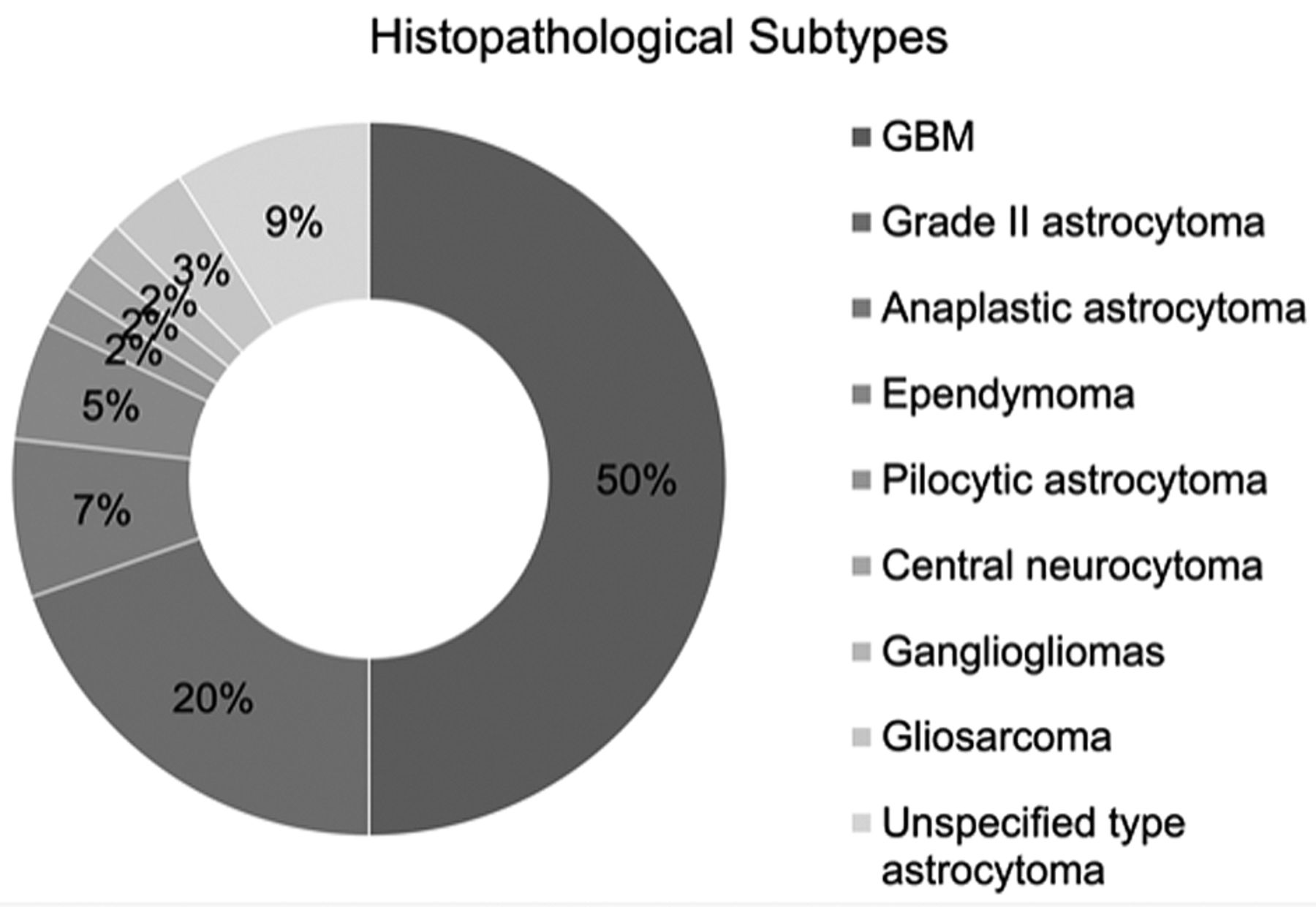
The median tumor size was 3.8 cm, ranging from 2 cm to 6 cm. Of cases with available data, the major histopathological subtypes of glioma included glioblastoma (n=28; 50.0%), grade II astrocytoma (n=11; 19.6%), anaplastic astrocytoma (n=4; 7.1%), ependymoma (n=3; 5.4%), gliosarcoma (n=2; 3.6%), pilocytic astrocytoma (n=1; 1.8%), ganglioglioma (n=1; 1.8%), and central neurocytoma (n=1; 1.8%), along with 5 astrocytoma cases with unspecified grade (Figure 2). Of all gliomas with available data, 38 (67.9%) were high-grade glioma (HGG – WHO III and IV), whereas 18 (32.1%) were low-grade glioma (LGG – WHO I and II).

Pie chart demonstrating histopathological subtypes of included gliomas. GBM, Glioblastoma multiforme.
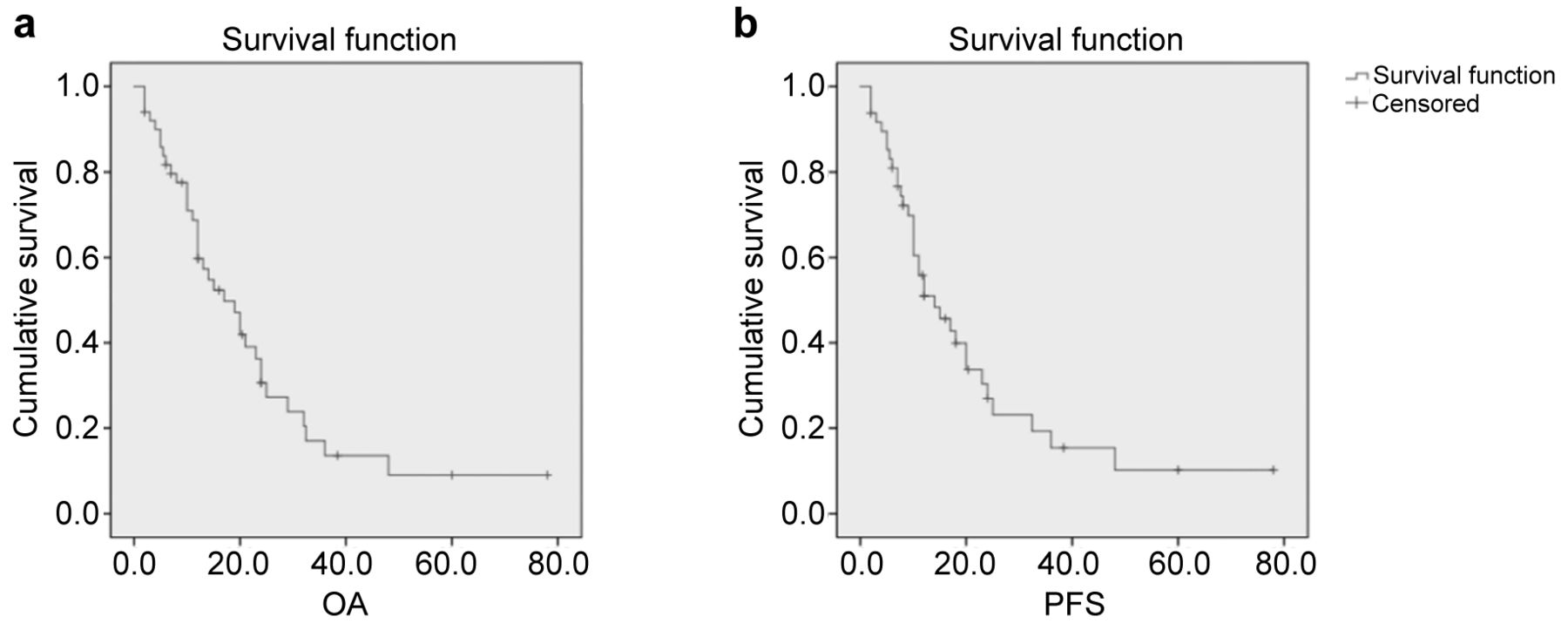
Management strategies and survival outcomes. Recurrence occurred in 12 (14.8%) patients, and death was documented in 70.6%. Median OS was 12 months (range=2-78), and median PFS was 11.3 months (range=2-78). The one-year OS and PFS rates were 60% and 51%, respectively (Figure 3); however, glioblastoma notably showed a one-year survival rate of 45%. LGG had better survival than HGG (p<0.01; Figure 4).

Kaplan-Meier survival curves for (a) OS (n=44) and (b) PFS (n=46) for the overall pooled cohort. OS, Overall survival; PFS, progression free survival.

Kaplan-Meier survival curves comparing low-grade and high-grade gliomas (Log-rank test, p<0.01).
Of all cases with hydrocephalus, twenty patients (40.0%) had VPS, and 12 (24.0%) had ETV; however, 18 patients (36.0%) did not undergo shunting. In addition, our results suggest a survival benefit for patients who underwent VPS compared to ETV (p<0.05; Figure 5).

Kaplan-Meier survival curves comparing ventriculoperitoneal shunt (VPS) and endoscopic third ventriculostomy (ETV) (Log-rank test, p<0.05).
All patients in our cohort underwent surgery, of which 14 (17.3%) underwent biopsy alone. Gross-total resection (GTR; removal of ≥98% of tumor) was achieved in only 34.6% of cases. Subtotal resection (STR; removal of 80-97%) and partial resection (removal of <80%) were achieved in 40.7% and 7.4% of cases, respectively. The most frequently used surgical approaches were the supracerebellar infratentorial approach (SCIT) (n=38; 62.3%), followed by the transcortical transventricular approach (TT) (n=11; 18.0%) and the transcallosal interhemispheric approach (TCIH) (n=8; 13.1%). Neither extent of resection (p=0.18) nor surgical approaches (p=0.17) demonstrated significant survival differences. Fifty-three patients (65.4%) received adjuvant therapy. While 32.1% of patients had chemotherapy, 40.7% received radiotherapy with a median dose of 5,770 cGy.
Discussion
This systematic review on PRGs sheds light on the clinical characteristics, treatment strategies, and survival outcomes. Our data support the overall poor prognosis of this rare group of neoplasms. We found no differences in OS based on surgical approach nor extent of resection. However, VPS showed a better survival benefit compared to ETV (p<0.05; Figure 5) in patients presenting with hydrocephalus.
Demographics and clinical characteristics. Our data indicated a male predominance (54.3%) and a median age of 39 years at presentation. In contrast, general data on gliomas indicate a 5-20 year older age of onset (17). We ascribe the early presentation in our cohort to the region’s complexity and confined anatomical space, especially in slow-growing subtypes. Clinical manifestations related to increased intracranial pressure presented largely as headaches (20.0%) with nausea and vomiting (16.9%), and they were similar to presenting symptoms of other pineal region tumors in adults and pediatric populations (31, 32). This is reasonable considering the proximity of the pineal region to the ventricular system, which puts patients at increased risk of obstruction.
Although our analysis failed to demonstrate significant survival benefits of shunting in hydrocephalus compared to cases without shunting, it remains an essential component of the management paradigm for hydrocephalus secondary to pineal region tumors (33, 34).
Our results show a variety of reported radiological features among different types of gliomas. While HGG tended to manifest with heterogeneous enhancement in the pineal region and sometimes infiltrated the surrounding structure, LGG presented well-demarcated mass lesions with minimal contrast enhancement. The median tumor size was 3.8 cm, presenting comparable results to pineal region meningiomas (15, 32). This is likely due to the confined, small space of the pineal region, with an expansion of the tumor resulting in clinical symptoms. Of available data in our cohort, HGG represents 67.9%, with glioblastoma being the most common type (73.7%) of HGGs. This finding is consistent with the overall prevalence of HGG and glioblastoma subtype among the general CNS gliomas and perhaps explains the poor overall survival (35).
Treatment modalities and survival outcomes. We found that only 14.8% of patients had recurrence after initial treatment, while 70.6% experienced death due to disease progression. This is reflective of the low rate of GTR and the malignant nature of most cases leading to the high rate of death in our cohort. In contrast to our results, Yamaki et al. systematically reviewed papillary tumors affecting the pineal region and reported higher recurrence rates (57%), yet recorded lower death rates (11%) (36). This discrepancy reflects the differences in the biological behavior between gliomas and papillary tumors and further emphasizes the malignant nature of gliomas.
Our results imply a poor median OS in our cohort (12 months), which is attributed to the predominance of HGG (67.9%); however, we find the wide survival range (2-78 months) reflective of the behavior variance among glioma subtypes. Additionally, we found a one-year OS rate of 60% among all PRGs, with glioblastoma showing the worst one-year survival rate of 45 percent. In contrast, supratentorial glioma literature shows a better median overall survival (5.9 years) and a higher one-year survival rate (72-94%), yet they reported a comparable glioblastoma one-year survival rate of 41% (3). These contrasting data support the role of the pineal region’s anatomical complexity in worsening the survival outcome due to the proximity of critical structures in such a dense, deep space (37). Lastly, we found that LGG achieved a better survival rate than HGG (p<0.01), in line with the general understanding of CNS glioma mortality (38).
Additionally, we found no difference in preoperative and postoperative KPS due to our scattered, scarce data; two studies reported KPS, containing only one case with postoperative data. Still, in one included article, Li et al. reported higher survival rates among LGG cases with KPS >60 than patients with KPS <60 (p=0.019) but failed to detect a significant difference in HGG (p=0.077) (4). Regardless, several studies in the literature examined the KPS prognostic value on gliomas of different CNS regions and concluded that a high preoperative KPS score (>60-80) along with a prolonged pre-hospitalization duration of symptoms (≥2 months) were associated with positive outcomes among glioma patients (39-41).
Data on the survival of shunting modalities among adults are scarce and controversial. Although most authors reported that ETV was more efficient despite its high failure rates, some argued that VPS is associated with prolonged survival and a better complication profile (42, 43). Interestingly, we found a superior survival benefit in patients who received VPS compared with cases who underwent ETV (p<0.05).
Our results showed that the supracerebellar infratentorial approach was the preferred surgical corridor (62.3%) as it provides direct access to the pineal region and third ventricle. This fundamentally offers a more uncomplicated dissection of the deep structures (25). In most cases, surgical resection failed to achieve GTR, documented in only 34.6% of our patients. These findings confirm the region’s related surgical challenges and further emphasize the neurosurgeons’ roles in navigating through available surgical approaches to achieve optimum tumor exposure and extent of resection.
In our review, 53 patients received adjuvant treatment; 32.1% received chemotherapy, and 40.7% received radiotherapy, with a median dose of 5,770 cGy. Although we did not find a survival correlation, adjuvant therapy has increased survival benefits in different cancers and has been a primary management element for different glioma subtypes (44-46). Therefore, avid research efforts, including clinical trials, have been employed to examine these therapeutic modalities (47, 48).
Limitations
This study has limitations. Our heterogeneous data and the small sample size challenged the statistical robustness, which further limited the pooled analysis. Although we detected significant survival differences, these results can be affected by confounding variables and potential bias. The inconsistency of study methodology and reported results of the included literature further limited our study findings.
Conclusion
Gliomas are malignant neoplasms that can involve the pineal region and can be excessively challenging to manage. Our data support the overall poor prognosis of HGG compared to LGG. Although we found a survival benefit in employing VPS in contrast to ETV, we failed to detect a significant survival benefit based on the extent of resection or surgical approach. To optimize pineal region glioma outcomes, a personalized medicine approach integrating clinical and histomolecular data is necessary. Large, prospective studies are needed to establish a standard management strategy and provide reliable prognostic conclusions.
Footnotes
Authors’ Contributions
Othman Bin Alamer: Conceptualization, Methodology, Data analysis, Writing – Original draft preparation; Navraj S. Sagoo, Scott E Rowe, and Aditya Dutta Gupta: Paper screening, Resources, Writing – Reviewing and Editing; Paolo Palmisciano, Maryam Haider, Mohammed Alduhaymi and Ali S. Haider: Resources, Data extraction, and Writing – Reviewing and Editing; Tarek Y. El Ahmadieh, Kenny Yu, Aaron A. Cohen-Gado, and Ali S. Haider l: Resources, Writing – Critically reviewing the final draft.
Conflicts of Interest
The Authors report no conflicts of interest concerning the materials or methods used in this study or the findings specified in this paper.
- Received December 20, 2021.
- Revision received January 22, 2022.
- Accepted January 26, 2022.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.