


Abstract
Background/Aim: Our laboratory pioneered the patient-derived orthotopic xenograft (PDOX) model. An important goal of PDOX-model development is facile visualization of metastasis in live mice. In the present report we evaluated tumor growth and metastasis in pancreatic cancer PDOX NOG [Non-obese diabetes (NOD)/Scid/IL2Rγnull]-and nude-mouse models using red fluorescent protein (RFP)-expressing tumor stroma to visualize the primary tumor and metastasis. Materials and Methods: A patient-derived pancreatic cancer was initially implanted in transgenic RFP-expressing nude mice. Then, tumor fragments, which acquired RFP expressing stroma while growing in RFP-expressing nude mice were orthotopically implanted in nude and NOG mice. The primary pancreatic tumor and metastasis were observed 8 weeks after implantation. Results: Lymph-node metastases expressing red fluorescence were detected only in NOG mice. Significantly faster growth of primary pancreatic tumors and a higher incidence of lymph-node metastasis occurred in NOG mice compared to nude mice. Conclusion: RFP-expressing tumor stroma, which traffics together with cancer cells to lymph nodes, is useful to observe tumor behavior, such as lymph-node metastasis in a PDOX NOG-mouse model which can be used for evaluation of novel anti-metastatic agents, as well as personalized therapy to identify effective drugs.
- pancreatic cancer
- patient-derived orthotopic xenograft (PDOX)
- NOG mouse
- nude mouse red fluorescent protein (RFP)
- lymph-node metastasis
- intravital imaging
- personalized therapy
- drug discovery
The patient-derived xenograft (PDX) model with subcutaneous tumors is being used to develop individualized treatment of patients with cancer as precision medicine (1). However, subcutaneously-implanted tumors rarely metastasize. Implantation at an orthotopic site is needed to observe tumor behavior more similar to that observed in patients, particularly metastasis, which occurs due to the tumor microenvironment (TME) (2). Our laboratory pioneered the patient-derived orthotopic xenograft (PDOX) model of major tumor types (3-9). A clinical study demonstrated that a gastric-cancer PDOX model had metastasis to the same organs as the patient donors of the PDOX tumor (7).
Our laboratory established transgenic nude mice expressing green-, red-, and cyan-fluorescent protein (10-12). Tumor fragments implanted to these transgenic nude mice can acquire fluorescent-protein-expressing tumor stroma, which can allow visualization of tumor location including distant metastasis in PDOX models by fluorescence imaging (13-17).
A major feature of the PDOX model is the possibility to observe the true metastatic potential of the patient tumor. In the preset study, we showed that in NOG [non-obese diabetes (NOD)/Scid/IL2Rγnull] mice, red fluorescent protein (RFP)-expressing orthotopically-implanted patient tumors, which acquired red fluorescent stroma from previous growth in RFP-transgenic nude mice, enabled detection of lymph-node metastasis by fluorescence imaging.
Materials and Methods
Mice. Athymic nu/nu nude mice, transgenic RFP-expressing athymic nu/nu nude mice (11), and NOG mice (AntiCancer, Inc., San Diego, CA, USA) were used in the present study. Mice were housed in a barrier facility equipped with high efficiency particulate air (HEPA)-filters at 22°C and 12-h light/dark cycles. Mice were fed an autoclaved laboratory rodent diet ad libitum. Mice were observed daily and humanely sacrificed by CO2 inhalation if they met the humane endpoint criteria: severe tumor burden (more than 20 mm in diameter), prostration, significant body-weight loss, difficulty breathing, rotational motion and body-temperature drop. All experiments were performed under an AntiCancer, Inc. Institutional Animal Care and Use Committee (IACUC) protocol approved for the present study, and under the principles and procedures provided in the National Institutes of Health Guide for the Care and Use of Animals under Assurance Number A3873-1.
Establishment of an imageable PDOX (iPDOX) model with red fluorescent stroma. A pancreatic-cancer PDOX model was previously established using surgical orthotopic implantation (SOI) (18). A patient-derived pancreatic-cancer growing subcutaneously in a nude mouse was harvested, and tumor fragments implanted subcutaneously in transgenic RFP-expressing nude mice. The subcutaneous tumor growing in the transgenic RFP expressing mouse was harvested and divided into approximately 5 mm3 fragments for SOI to nude and NOG mice (Figure 1A). RFP-expressing tumor fragments were confirmed with the FluorVivo imaging system (INDEC Biosystems, Santa Clara, CA, USA) before implantation (Figure 1B). For SOI, a 7 mm transverse incision was made on the left flank of nude and NOG mice under anesthesia with subcutaneous injection of a 0.02 ml solution comprising 0.25 mg ketamine, 0.38 mg xylazine, and 0.012 mg acepromazine maleate. The pancreas tail and spleen were exposed, and a single tumor fragment was implanted orthotopically into the pancreas tail with a 7-0 polypropylene suture (AD Surgical, Sunnyvale, CA, USA) (Figure 1C) (4). The incision was closed with a 6-0 nylon suture (AD Surgical). Tumor volume was calculated by the following formula: Tumor volume (mm3)=length (mm) × width (mm) × width (mm) ×1/2.
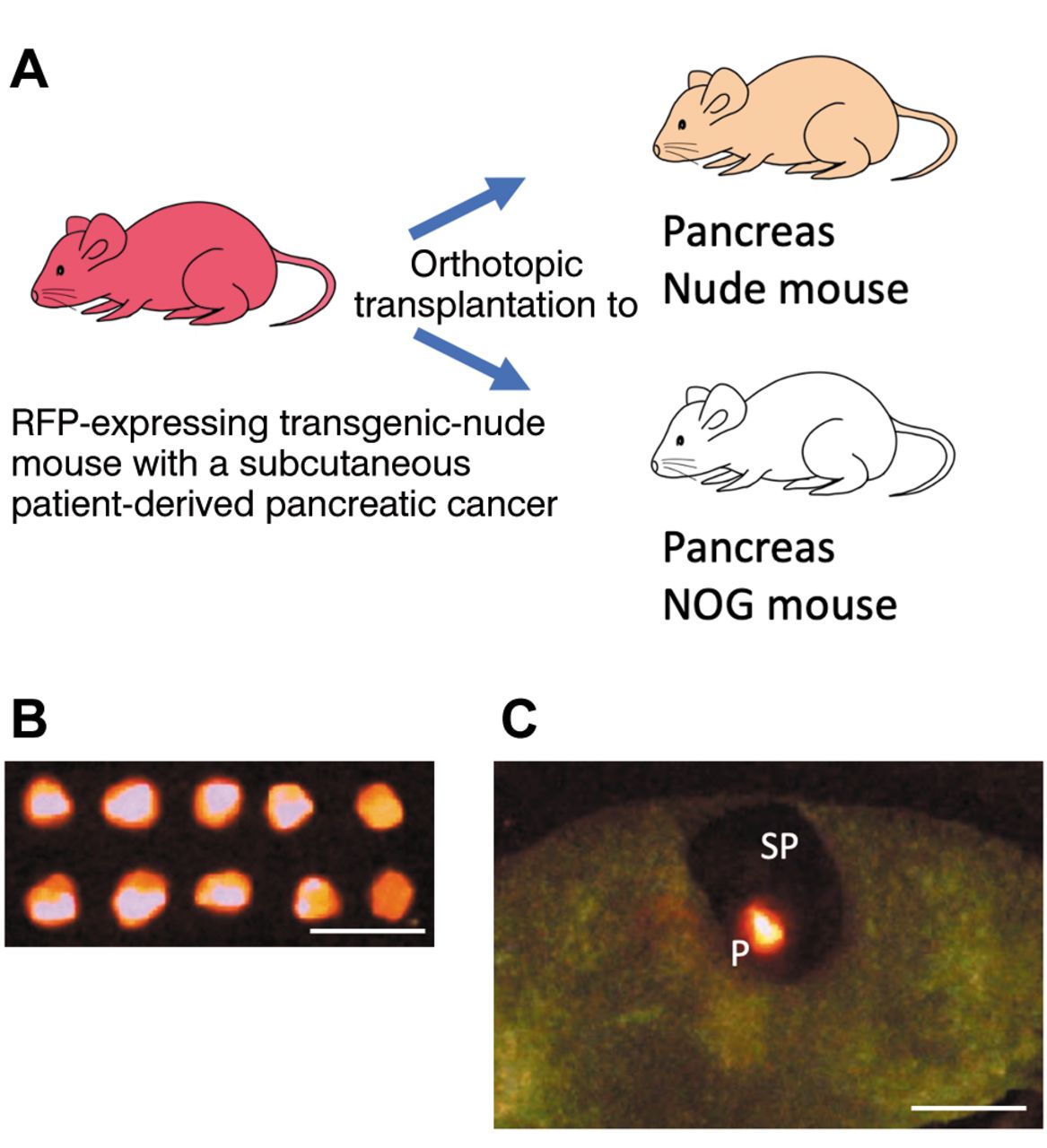
Establishment of an imageable PDOX (iPDOX) model with red fluorescent stroma. a: A pancreatic-cancer tumor, growing in a subcutaneous pocket of a transgenic red fluorescent protein (RFP)-expressing nude mouse, was harvested. Then, the tumor fragments, grown subcutaneously, were implanted to the pancreas of nude and NOG mice. B: Resected tumor fragments from the RFP nude mouse had red fluorescence as visualized by the FluorVivo imaging system. Scale bar: 10 mm C: A red-fluorescent tumor fragment was implanted to the pancreas tail. P: pancreas, SP: spleen. Scale bar: 10 mm.
Imaging of the tumor with red fluorescent stroma. All mice were sacrificed 8 weeks after tumor implantation. RFP fluorescence was detected with the FluorVivo imaging system after opening the chest and abdomen of each nude and NOG mouse.
Histological examination. All tumors were resected and immediately fixed in 10% formalin. These samples were embedded in paraffin, and then hematoxylin and eosin (H&E) staining was performed on 4 μm tissue sections. The H&E-stained slides were observed with a BH2 Olympus microscope (Olympus Corp., Tokyo, Japan).
Statistical analysis. Tumor volume is presented as the mean±SD, and the Student’s t-test was performed to evaluate the differences between the means. Fisher’s exact test was performed to evaluate statistical significance in the number of mice with lymph-node metastasis between nude and NOG mice. p-values ≤0.05 are considered to be statistically significant. Statistical analyses were conducted with GraphPad Prism 7 (GraphPad Software, Inc., San Diego, CA, USA).
Results
Primary cancers and lymph-node metastasis detected by RFP expression in a pancreatic-cancer PDOX model. RFP-expressing primary pancreatic tumors were detected in both nude and NOG mice (Figure 2A, B). However, abdominal, mediastinal, and neck lymph-node metastases, expressing RFP, were detected only in NOG mice (Figure 2B). Histological examination confirmed primary pancreatic cancer (Figure 2C) and lymph-node metastasis as pancreatic cancer (Figure 2D), using H&E- stained slides made from paraffin-embedded tissues.

Representative fluorescence images acquired with the FluoroVivo imaging system 8 weeks after orthotopic transplantation to an NOG mouse of a patient pancreatic cancer previously grown in an RFP-expressing nude mouse. All images were obtained after opening the chest and abdomen. A: nude mouse. B: NOG mouse. Scale bars: 10 mm. Primary pancreatic tumors are shown within white dotted circles. White arrows show lymph-node metastases expressing red fluorescence. Scale bars: 10 mm. H&E-stained slides of primary and metastatic tumors imaged with a BH2 Olympus microscope. C: Pancreatic tumor, D: Lymph node metastasis. Scale bars: 100 μm.
Comparison of primary pancreatic-tumor growth and incidence of lymph-node metastasis between nude and NOG mice. All tumor fragments grew in the pancreas of nude and NOG mice by 8 weeks after orthotopic tumor implantation. Pancreatic tumor size was significantly larger in NOG mice (281±61 mm3) than in nude mice (88±25 mm3) (p=0.012) (Figure 3A). Five NOG mice (62.5%) had lymph-node metastasis expressing RFP. However, no RFP-expressing lymph nodes were observed in any of the 8 nude mice. There was a significant difference in incidence of lymph node metastasis between nude and NOG mice (p=0.026) (Figure 3B).

Comparison of primary pancreatic-tumor growth and incidence of lymph-node metastasis between nude- and NOG-PDOX-mouse models. A: Volume of primary pancreatic tumors 8 weeks after implantation in nude and NOG mice. Error bars: ±SD *p<0.05. B: Number of mice with lymph-node metastasis detected by red fluorescence. *p<0.05.
Discussion
In the present study, faster growth of the primary pancreatic tumor and higher incidence of lymph-node metastasis were observed in NOG mice compared to nude mice. In addition, lymph-node metastasis expressing RFP was detected by intravital imaging and confirmed in H&E-stained histological slides slides. The present findings indicate that cancer cells with surrounding stroma such as cancer-associated fibroblasts (CAFs) (19) and tumor-associated macrophages (TAMs) (20) trafficked together from the pancreas to lymph nodes in NOG mice.
Lymph-node metastasis in PDOX models has been already demonstrated ex vivo (7, 21), and the present study showed lymph-node metastasis expressing RFP that can be detected by intravital imaging. A previous study that used a pancreatic-cancer PDOX model with fluorescent-protein expressing stroma in nude mice showed metastasis in the peritoneum and liver, but not in lymph nodes (22). In the clinic, most pancreatic cancers metastasize to lymph nodes first, and then metastasize to distant organs, such as liver and lung, through the blood circulation. In the present study, lymph-node metastasis was observed by 8 weeks after tumor implantation in NOG mice. If a longer observation time were allowed, liver and lung metastasis may have occurred.
For metastatic colonization to occur, cancer cells must change their TME to that of distant organs (23, 24). CAFs modulate cancer metastasis through synthesis and remodeling of the extracellular matrix (ECM) and production of growth factors (25, 26). However, the precise function of CAFs for metastasis is incompletely understood (26). The present study indicates that both pancreatic-cancer cells and tumor- stromal cells traffic together into the lymphatic circulation, and then propagate in lymph nodes. Therefore, cancer cells possibly need to traffic along with CAFs in order to metastasize to lymph nodes.
In conclusion, RFP-expressing tumor stroma, which can traffic together with cancer cells to lymph nodes, is useful to observe tumor behavior such as lymph-node metastasis in a PDOX NOG-mouse model. NOG mice may be superior to observe tumor growth and metastasis in PDOX models. The present PDOX model of metastatic pancreatic cancer can be used for evaluation of novel anti-metastatic therapeutics and for personalized medicine.
Acknowledgements
This paper is dedicated to the memory of A. R. Moossa, M.D., Sun Lee, M.D., Professor Li Jiaxi, Masaki Kitajima, M.D., and Joseph R. Bertino, M.D.
Footnotes
Authors’ Contributions
Project development: NS and RMH. Data collection: NS and KM. Analysis and interpretation of data: NS, KM, TH, HO, JHP, KK, MB, MU, and RMH. Writing, review, and revision of the manuscript: NS and RMH.
Conflicts of Interest
The Authors declare that there are no potential conflicts of interest. AntiCancer, Inc. uses patient derived orthotopic xenograft (PDOX) mouse models for contract research. NS, KM, TH, HO, JHP, and RMH are or were unsalaried associates of AntiCancer, Inc.
Funding
This research was funded in part by the Robert M. Hoffman Foundation for Cancer Research.
- Received December 11, 2021.
- Revision received January 4, 2022.
- Accepted January 5, 2022.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.