


Abstract
Background/Aim: We retrospectively evaluated the efficacy and toxicity of concurrent chemoradiotherapy (CCRT) with docetaxel, cisplatin, and 5-fluorouracil (TPF) for T3 N0 glottic carcinoma without vocal cord fixation. Patients and Methods: Twenty-five patients underwent TPF-CCRT without elective nodal irradiaion (ENI). After the RT of 40 Gy, five patients (20%) without tumor regression underwent surgery. Others underwent RT with a median total dose of 66 Gy. Results: Of the five patients who underwent surgery after the RT of 40 Gy, two showed residual carcinoma pathologically and the other three were confirmed to have complete pathological response to the treatment. The 5-year local control rate was 87%. No patients exhibited regional failure. No acute toxicities of grade 5 or late toxicities ≥grade 3 were observed. Conclusion: TPF-CCRT provides excellent tumor control with acceptable toxicities. CCRT while omitting ENI is a reasonable approach for T3 N0 glottic carcinoma without vocal cord fixation.
- Head and neck cancer
- glottic carcinoma
- radiotherapy
- chemoradiotherapy
- laryngeal preservation
- elective nodal irradiation
Squamous cell carcinoma (SCC) of the glottis is the most common laryngeal cancer (1). Since the sixth edition of the TNM staging system was proposed in 2002 by the Union for International Cancer Control (UICC), diagnostic imaging modalities such as computed tomography (CT) and magnetic resonance (MR) imaging in addition to physical examination have been required for T-staging (2, 3). The current eighth edition of the TNM staging system defines T3 disease as “tumor limited to larynx with vocal cord fixation and/or invades paraglottic space, and/or inner cortex of the thyroid cartilage,” which has no major revisions from the sixth edition.
T3 N0 glottic carcinoma without vocal cord fixation had been categorized into early T1-T2 N0 disease before the introduction of the sixth edition of the UICC TNM staging system. Radiotherapy (RT) alone has been recognized as a standard treatment for the disease; however, its treatment outcome is not sufficient, with a 5-year local control (LC) rate of 40%-50% (3, 4). Chemoradiotherapy (CRT) has been used to improve treatment results and recommended in the current NCCN guidelines (5). However, reports on the treatment results of CRT for this disease are limited.
Chemotherapy comprising docetaxel, cisplatin, and 5-fluorouracil (TPF) is one of the widely used regimens for head and neck SCC (6-8). A previous study suggested that concurrent CRT (CCRT) with TPF is more effective than induction chemotherapy with TPF followed by RT (9). In the present study, we evaluated the efficacy and toxicity of CCRT with TPF for T3 N0 glottic carcinoma without vocal cord fixation.
Patients and Methods
Patients. This retrospective study received the full approval from the institutional research ethics board of Kumamoto University Hospital (No. 2281). Between February 2006 and April 2019, 27 consecutive patients with pathologically confirmed T3 glottic SCC without vocal cord fixation matched eligibility criteria of TPF-CCRT. Of these, 26 were treated with TPF-CCRT at our hospital. One patient refused chemotherapy and underwent RT alone. One patient was excluded from the analysis because of a coexisting advanced hypopharyngeal carcinoma. After the exclusion was made, the final study population consisted of 25 patients. Prior informed consent was obtained from all the patients for the treatment and use of their medical information in future studies. Clinical staging was performed by the institutional head and neck tumor board of radiation oncologists, otolaryngologists, and radiologists. Pretreatment examination included physical, endoscopic, and ultrasonographic exminations with or without fine-needle aspiration cytology specimens in addition to MR imaging with or without gadolinium-based contrast agents. Whole-body CT imaging with or without [18F]-fluoro-2-deoxy-D-glucose positron emission tomography was also performed (10). The tumors were staged in accordance with the sixth to eighth edition of the UICC TNM staging system.
Eligibility criteria and treatment. To undergo treatment, the patients had to be 20-80 years of age; have a performance status of 0-2, and a life expectancy of at least 3 months; have adequate hematologic (white blood cell count ≥3,500/mm3, absolute neutrophil count ≥2,000/mm3, hemoglobin level ≥9.5 g/dl, and platelet count ≥100,000/mm3), renal (creatinine ≤1.2 mg/dl and creatinine clearance ≥60 ml/min), and hepatic functions [total bilirubin level of 1.5 mg/dl, aspartate aminotransferase level ≤2× upper limit of normal (ULN), and alanine aminotransferase level ≤2 × ULN]; and have no severe complications. Chemotherapy consisted of one or two cycles of TPF. The patients received an intravenous infusion of docetaxil (50 mg/m2) for an hour on day 1. More than 1 h after completing the docetaxel infusion, 5-FU (600 mg/m2/day) was delivered via continuous intravenous infusion on days 1-5. Cisplatin (60 mg/m2) was given intravenously on day 4 (9, 11). Subcutaneous granulocyte colony-stimulating factor was administered to patients with febrile neutropenia.
RT was delivered using a 4-MV linear accelerator. The patients underwent local irradiation with opposed lateral fields. The field size was typically 6×6-7×7 cm (median, 42 cm2) without elective nodal irradiation (ENI) (4). RT was delivered with a once-daily fraction of 2 Gy. After the delivery of 40 Gy and one cycle of chemotherapy, the head and neck tumor board performed an interim assessment to evaluate the tumor regression on the basis of endoscopic examination and MR imaging findings (4, 12). In the earlier period, five patients (20%) were judged as having no tumor regression and underwent surgery: total laryngectomy (n=3) and laryngeal preservation (n=2). The remaining 20 patients underwent RT with a radical total dose of 64-70 Gy (median, 66 Gy).
Follow-up. The details of the follow-up are described elsewhere (4). Briefly, after treatment completion, the patients were followed up every month during the first year, every 3 months during the second year, and every 6 months thereafter. Physical and endoscopic examinations were performed at each follow-up visit. Posttreatment ultrasonography, MR, and/or CT imaging were also performed within 2 months after treatment completion and every 6 months thereafter or when clinically indicated.
Evaluation of outcomes and statistical analysis. LC, laryngeal preservation (LP), and overall survival (OS) rates were calculated from treatment initiation by using the Kaplan–Meier method. The patients who underwent surgery and had a complete pathological response to the treatment were censored at the time of surgery for the calculation of LC in accordance with the previous reports of Mendenhall et al. (13). Treatment-associated toxicities were evaluated using the Common Terminology Criteria of Adverse Events Version 5.0 (CTCAE 5.0). Statistical calculations were performed using the SPSS version 26.0 software (IBM, Armonk, NY, USA).
Results
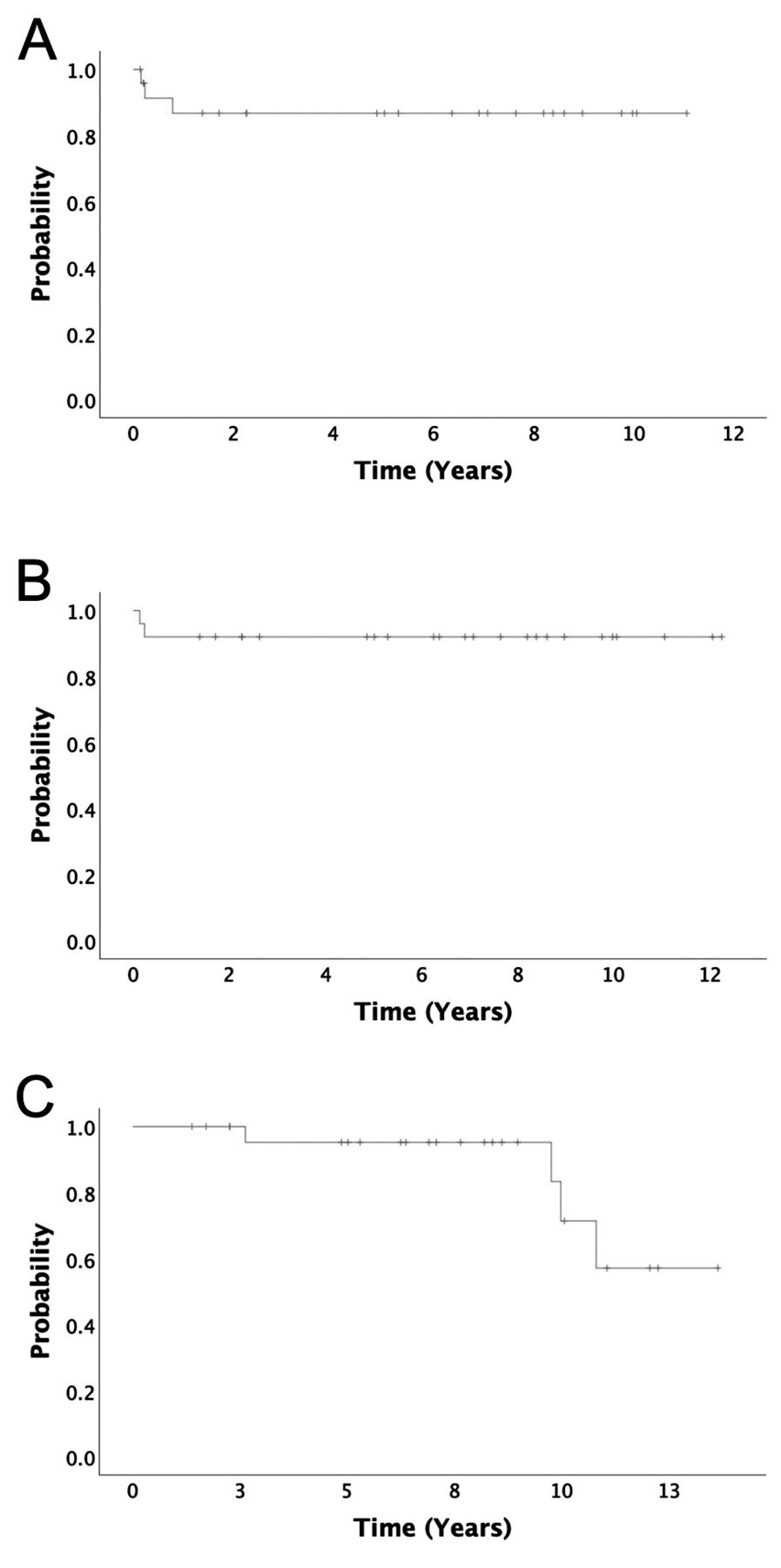
The patients’ characteristics are summarized in Table I. The median follow-up duration was 91.8 months (range=16.6-163.8 months). Of the five patients who underwent surgery after the delivery of 40 Gy, two had a residual carcinoma pathologically and the other three were confirmed to have a complete pathological response to the treatment. During the follow-up period after a series of therapies, one patient had local failure and died of pneumonia, probably owing to the local recurrence. Three patients died of other diseases. None of the patients exhibited regional or distant failure. The 5-year LC, LP, and OS rates were 87%, 92%, and 95%, respectively (Figure 1). Table II shows the details of acute and late toxicities ≥grade 2. Neutropenia was frequently observed during the treatment but was manageable in all the patients. Late toxicity of grade 1 laryngeal edema was observed in two patients (8%). No acute toxicities of grade 5 or late toxicities ≥grade 3 were observed.
Patients’ characteristics (n=25).
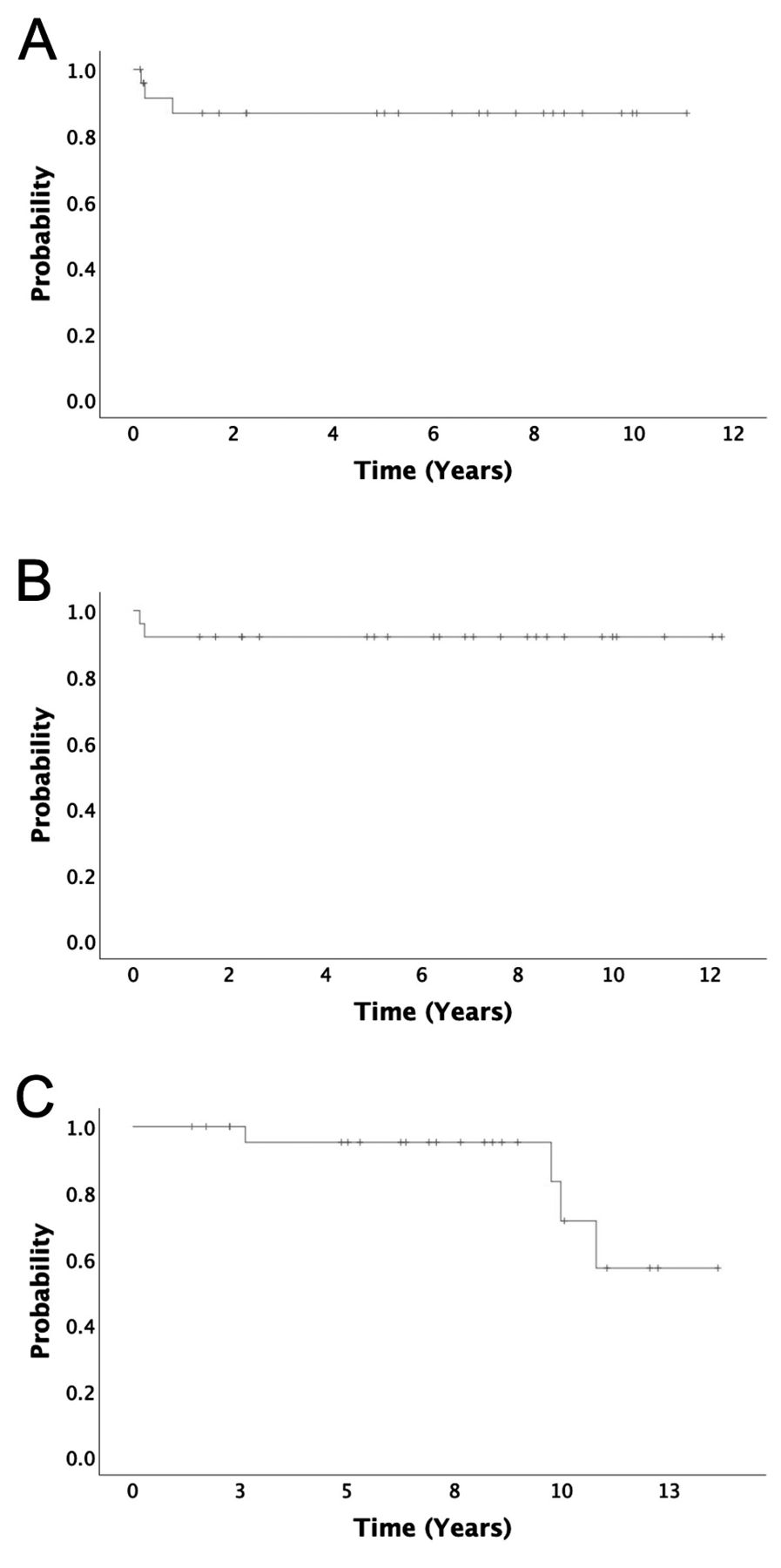
Kaplan–Meier curves. (A) Local control, (B) laryngel preservation, and (C) overall survival.
Details of adverse events.
Discussion
Owing to the reports of the insufficient outcomes of RT alone with conventional fractionation, more-intensive treatment strategies have been used for T3 N0 glottic carcinoma without vocal cord fixation. Okumura et al. reported the treatment results of 74 patients with T3 N0 glottic carcinoma without vocal cord fixation (14). They divided the patients into three groups according to treatment regimen as follows: accelerated fractionated RT (AFRT) with 63-65.25 Gy in 27-29 fractions (2.25-2.4 Gy per fraction, once daily) without ENI (AFRT group, n=41), CCRT using cisplatin or cetuximab with ENI of 40-46 Gy in 20-23 fractions (2 Gy per fraction, once daily) followed by boost irradiation with 24-30 Gy in 12-15 fractions (2 Gy per fraction, once daily; CCRT group, n=10), hyperfractionated RT (HFRT) with ENI of 40-46 Gy in 20-23 fractions (2 Gy per fraction, once daily) followed by boost irradiation with 24-30 Gy in 16-20 fractions (1.5 Gy per fraction, twice daily; HFRT group, n=23). The 3-year local failure and OS rates were 10% and 77%, 20% and 100%, and 26% and 87% for the AFRT, CCRT, and HFRT groups, respectively. Murakami et al. prospectively evaluated CCRT for T2 N0 glottic carcinoma staged according to UICC TNM staging system, fifth edition (15). The RT dose of 64 Gy was delivered with a once-daily fraction of 2 Gy using low-dose chemotherapy, including cisplatin and UFT. Of 51 cases, 24 were restaged as T3 N0 without vocal cord fixation according to UICC TNM staging system, sixth edition. Their 5-year LC and LP rates were 62% and 83%, respectively. Lin et al. evaluated the efficacy of CCRT for 17 patients with T3 glottic carcinoma (16). Of the 17 patients, 16 (94%) had N0 and one (6%) had N1 disease. Nine patients (53%) had vocal cord fixation. A median RT dose of 70 Gy (range=62-72.5 Gy) was delivered with a once-daily fraction of 2-2.07 Gy using cisplatin-based chemotherapy. The 5-year LC, laryngectomy-free survival, and OS rate were 87%, 81%, and 89%, respectively. The LC, LP, and OS rates in our study were considered as equivalent to or greater than those in the previous reports.
The major acute toxicities of TPF-CRT are hematologic toxicities and mucositis. Katori et al. performed TPF-CRT for 34 patients with advanced SCC of the head and neck (9). The chemotherapy regimens consisted of two cycles of docetaxel 60 mg/m2 (day 1), 5-FU 750 mg/m2/day (days 1-5), and cisplatin 70 mg/m2 (day 4) for induction chemotherapy (n=15, induction CRT group) and two cycles of docetaxel 50 mg/m2 (day 1), 5-FU 600 mg/m2/day (days 1-5), and cisplatin 60 mg/m2 (day 4) for CCRT (n=19, CCRT group), which were similar to or the same as ours. The total RT doses were 64-70 Gy (mean, 66.9 Gy) for the induction CRT group and 63-74 Gy (mean, 67.8 Gy) for the CCRT group. Grade 3-4 leukocytopenia, neutropenia, and mucositis were observed in 6 (40%), 9 (60%), and 6 patients (40%) in the induction CRT group and 10 (53%), 8 (42%), and 15 patients (79%) in the CCRT group. Komatsu et al. performed TPF-CCRT for 24 patients with nasopharyngeal carcinoma (11). Chemotherapy included two cycles of docetaxel 50 mg/m2 (day 1), 5-FU 600 mg/m2/day (days 1-5), and cisplatin 60 mg/m2 (day 4), which were the same as ours. RT included ENI with 40-45 Gy followed by boost irradiation, for a total of 70 Gy. Grade 3-4 neutropenia and mucositis were observed in 10 (42%) and 16 patients (67%), respectively. Our results on hematologic toxicities were similar with theirs. On the other hand, our results indicated obviously milder mucositis as compared with their results, probably because we omitted ENI. Overall, the toxicities we encountered were acceptable.
Currently, ENI for levels of II, III, and IVa is recommended and widely performed for patients with T3 N0 glottic carcinoma (17, 18). However, T3 N0 glottic carcinoma without vocal cord fixation was previously categorized into early T1-T2 N0 disease and usually treated with RT without ENI (15, 19). Regional failure after treatment completion was uncommon. We previously reported the recurrence pattern of staged or restaged T3 N0 disease without vocal cord fixation by reviewing 64 cases treated with RT with or without chemotherapy (4). Of the 64 patients, 22 (34%) underwent RT alone and 42 (66%) underwent CCRT with low-dose or TPF-chemotherapy. Ten patients (16%) underwent total laryngectomy or LP surgery after the delivery of 40 Gy because the tumor showed no regression. The remaining 54 patients received a total RT dose of 60-72 Gy (median, 66 Gy). Eighteen patients (28%) developed recurrence, and all of them were recorded as local failure alone. None of the patients developed regional and distant failure. Similarly, as mentioned earlier, Okumura et al. performed AFRT without ENI for 41 patients with T3 N0 glottic carcinoma without vocal cord fixation (14). Five patients (12%) developed disease progression. The initial recurrence site was local in three patients (7%) and regional in only two patients (5%). It is essential to maintain a fine balance between treatment intensity for tumor control and avoiding toxicities, especially mucositis, in head and neck cancer. From this point of view, intensive local treatment with CCRT while omitting ENI is a reasonable approach for T3 N0 glottic carcinoma without vocal cord fixation.
Previously, surgery was one of the main treatment modalities for T3 glottic carcinoma, and radical RT with or without chemotherapy was performed only for selected patients (20). Therefore, in the early part of our series, five patients underwent surgery after the delivery of 40 Gy, but more than half of the patients were confirmed to have complete pathological response to the treatment with RT of 40 Gy and one cycle of TPF. Considering the excellent LC in our study, complete cure can be obtained with radical TPF-CCRT even if patients have no tumor regression at the time of interim assessment.
Our study has some limitations. First, this was a retrospective study involving a relatively small number of patients. Second, five patients underwent surgery after the delivery of 40 Gy and one cycle of chemotherapy. The potential bias of surgical intervention might influence our conclusions.
In conclusion, TPF-CCRT provided excellent tumor control with acceptable toxicities for T3 N0 glottic carcinoma without vocal cord fixation. Intensive local treatment with CCRT while omitting ENI is a reasonable approach for the disease.
Footnotes
Author’s Contributions
RT developed the study design; collected, analyzed, and interpreted the data; performed the statistical analysis; and wrote the manuscript. TW developed the study design, collected and interpreted data; and performed the statistical analysis. DM collected and interpreted the data. TM, TS, YF, and KN developed the study design and analyzed and interpreted the data. YO and NO developed the study design and interpreted the data. All Authors have read and approved the final manuscript.
Conflicts of Interest
The Authors declare that they have no conflicts of interest related to this study.
- Received November 8, 2021.
- Revision received November 25, 2021.
- Accepted November 26, 2021.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.