


Abstract
Background/Aim: We investigated the predictive value of scoring systems of peritoneal disseminations for complete surgery (CS) at primary debulking surgery (PDS) in advanced ovarian cancer. Patients and Methods: We retrospectively enrolled eligible patients with clinical stages III or IVA selected for PDS from January 2015 to December 2019. Concern variables were predictive index value (PIV) and peritoneal cancer index (PCI) from operative and pathological reports. Primary endpoints were cutoffs to predict operative completeness using the receiver operating characteristic curve. Results: Among 111 patients, PIV ≥8 and PCI ≥13 were the best predictors of incomplete PDS, including optimal and suboptimal surgeries (AUC=0.821 and 0.855, respectively). CS rates in PIV ≤6 and PCI ≤12 were significantly higher than in PIV ≥8 (89.3% vs. 47.2%; p<0.05) and PCI ≥13 (90.9% vs. 41.2%: p<0.05). Conclusion: PIV and PCI are potential predictors for CS at PDS.
- Advanced ovarian cancer
- complete surgery
- primary debulking surgery
- predictive index value
- peritoneal cancer index
Every year, numerous patients suffer from ovarian cancer, the seventh most prevalent malignant tumor in women, with almost 240,000 newly diagnosed cases annually, as well as the eighth most common cause of female cancer death, with almost 150,000 deaths annually worldwide (1). In Japan, the incidence of ovarian cancer has been increasing up to 15.0 per 100,000 women, almost half of whom were newly diagnosed as advanced ovarian cancer (AOC) with International Federation of Gynecology and Obstetrics (FIGO) stage III and IV (36.2% and 10.0%, respectively) (2).
Complete resection in primary debulking surgery (PDS) is considered the most favorable therapeutic option for AOC (3). Recently, several randomized control trials (RCTs) compared the postoperative prognosis between PDS and interval debulking surgery (IDS) after neoadjuvant chemotherapy (NAC) (4-7). Of these trials, the EORTC and CHORUS studies showed non-inferiority of IDS to PDS (4, 5). In the SCORPION trial, NAC + IDS was not superior to PDS in improving prognosis, but the authors considered NAC + IDS as an acceptable strategy for patients with large dissemination burdens because the incidence of operative complications was less than that for PDS (7). Although other RCTs are ongoing to clarify therapeutic superiority of PDS to overcome the limitations in previous studies, such as the low rate of complete surgery (8, 9), gynecologists need to pursue complete surgery in PDS (complete PDS), and if it seems difficult, consider NAC + IDS. Therefore, in deciding on operative options for AOC, a reliable predictive model for operative completeness in PDS based on preoperative examinations should be established.
Recently, diagnostic laparoscopy has been indicated as the safest method for tumor biopsy in AOC cases, and it has been also established as a potential strategy for detecting cases with large disseminations likely to result in suboptimal surgery in PDS (10). Furthermore, some quantitative scoring systems for abdominal disseminations, such as predictive index value (PIV) and Peritoneal Cancer Index (PCI), have been used to predict operative results (11, 12). However, the validation of their predictive value could differ between institutions, depending on factors such as the rate of complete PDS, number of surgeries of AOC, and familiarity with these scores. Moreover, because most of them focus on the predictive value for suboptimal surgery in PDS, any valid consensus for predicting complete PDS have not been established. Therefore, data on their value for predicting operative completeness need to be collected. Additionally, although a recent Cochrane review pointed out that the laparoscopic predictive models resulted in suboptimal surgery at PDS in some cases, even after a diagnostic laparoscopy indicated that optimal debulking surgery was feasible (13), reports on limitations of these scores in predicting operative outcomes have been limited.
In this study, we retrospectively investigated the value and limitations of PIV and PCI for the prediction of operative completeness in PDS.
Patients and Methods
Patients. In this retrospective study, we enrolled patients who were all selected for PDS at our affiliated hospitals from January 2015 to December 2019. These patients were diagnosed with AOC, including fallopian tube and peritoneal cancers, with clinical stage III or IVA by preoperative examinations, such as computed tomography (including positron emission tomography-computed tomography), and magnetic resonance imaging. If necessary, diagnostic laparoscopy and pleural cytology were also performed. Patients who had no staging surgery, who were diagnosed with double ovarian and endometrial or cervical cancers, who underwent primary diagnostic surgery, such as hysterectomy or bilateral salpingo-oophorectomy, at a previous hospital, and who had insufficient operative or pathological reports for peritoneal dissemination were excluded. Additionally, according to our previous report (14), we conventionally selected NAC + IDS as a therapeutic option for those with extensive tumor disseminations or a tumor in the right triangular ligament identified by preoperative imaging examinations or diagnostic surgeries. We planned to gather almost 100 eligible patients, referring to previous studies (11, 15, 16). This study was approved by the institutional review board for clinical research of the Jikei Medical School of Medicine (Approval Number: 31-234[9733]). We obtained informed consent from patients by posting the opt-out at the outpatient office of our department.
Surgical procedure. Standard PDS at our institutions usually includes hysterectomy, bilateral salpingo-oophorectomy, omentectomy, retroperitoneal lymphadenectomy, and appendectomy. If necessary, we perform peritonectomy, visceral resection, diaphragmatic procedure, hepatectomy, splenectomy, pancreatectomy, or cystectomy with the cooperation of surgeons. Complete surgery is defined as complete resection of all abdominal tumors without macroscopic residues. Optimal surgery is defined as incomplete resection of all abdominal tumors, leaving macroscopic residues ≤1 cm in maximal diameter. Additionally, suboptimal surgery is defined as incomplete surgery of all abdominal tumors, leaving macroscopic residues ≥1 cm in maximal diameter, including surgeries that were initially planned PDS but ended in probe laparotomy because of large tumor dissemination.
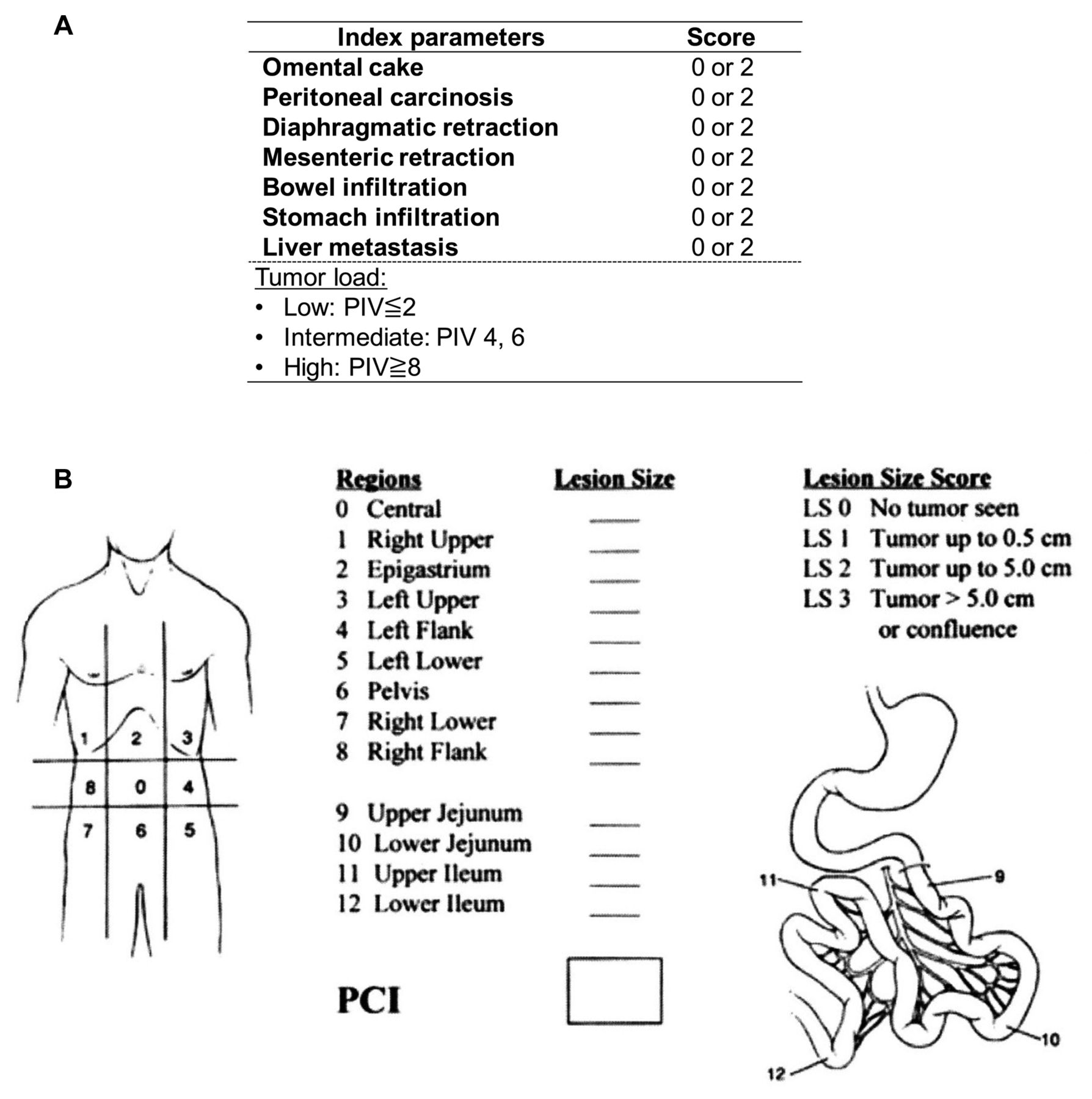
Predictive index value and peritoneal cancer index. We applied PIV (11) and PCI (17) (Figure 1A and B) in assessing intraoperative peritoneal dissemination, referring to operative and histopathological reports. PIV was reported by Fagotti et al. (11) in 2006 as a laparoscopic scoring system for predicting suboptimal surgery for AOC. Omental cake, peritoneal carcinomatosis, diaphragmatic carcinomatosis, mesenteric retraction, bowel and stomach infiltration, and liver metastasis are evaluated intraoperatively during diagnostic laparoscopy. If each category is positive, an index value of 2 is assigned, with a possible total score of 14. Fagotti et al. found that PIV ≥8 could predict suboptimal surgery with a positive predictive value of 100%. PCI was reported by Sugarbaker et al. (15) in 1995 for the quantitative assessment of peritoneal carcinomatosis in advanced colon cancer. In PCI scoring, the abdominopelvic cavity (regions 0-8) and small bowels (regions 9-12) are divided into 13 regions. The lesion size score (LSS) in each region is then calculated. LSS 0 is defined as no visible tumor in each region. LSS 1, 2, and 3 are assigned according to the maximum size of tumor dissemination in each region, namely, 0-0.5 cm, 0.5-5 cm, and >5 cm, respectively. The possible total LSS was 39 points.
Endpoints. The primary endpoints were the best cutoff values of both scores for predicting operative completeness in PDS and the rates of complete PDS in each category of both scores. The secondary endpoints were clinicopathological features between the groups under and over the cutoffs of both scores and the correlation between them. Moreover, we investigated the characteristics of cases that resulted in suboptimal surgery with lower than the two cutoffs to understand limitations of these scores in predicting operative results.
Statistical analysis. First, the receiver operating characteristic (ROC) curve was used to determine the best cutoff values for PIV and PCI to identify patients likely to have incomplete PDS (optimal and suboptimal surgery in PDS) as an alternative indicator for the prediction of complete PDS. Next, the comparison of the rates of complete surgery in each category of both scores was assessed by χ2 test. The correlation was assessed by Spearman’s rank correlation coefficient test. Continuous data were presented as means±standard deviation and analyzed using Student’s t-test. Categorical data were presented as percentages and analyzed using χ2 test. We considered p-values <0.05 to be statistically significant. Statistical analyses were conducted using Stata SE 14 (STATA Corp., College Station, TX, USA). Additionally, Prism 8.01 software (GraphPad Inc.) was also used for preparing column figures.
Results
Demographic and operative characteristics. A total of 111 patients were eligible for the analysis (Figure 2). Patient characteristics are shown in Table I. The mean age was 56.8±10.6 years old. The number of patients with clinical stages IIIA, IIIB, IIIC, and IVA were 17 (15.3%), 28 (25.2%), 65 (58.6%), and 1 (0.9%), respectively. According to the final histopathological reports, 72 (64.9%) patients had high-grade serous carcinoma and 19 (17.1%) were diagnosed with clear cell carcinoma. Complete surgery was achieved in 84 patients (75.7%), optimal surgery in 7 patients (6.3%), and suboptimal surgery in 20 patients (23.8%), including 16 cases ended in probe laparotomy.

Flow diagram for patient selection.
Patient clinicopathological characteristics.
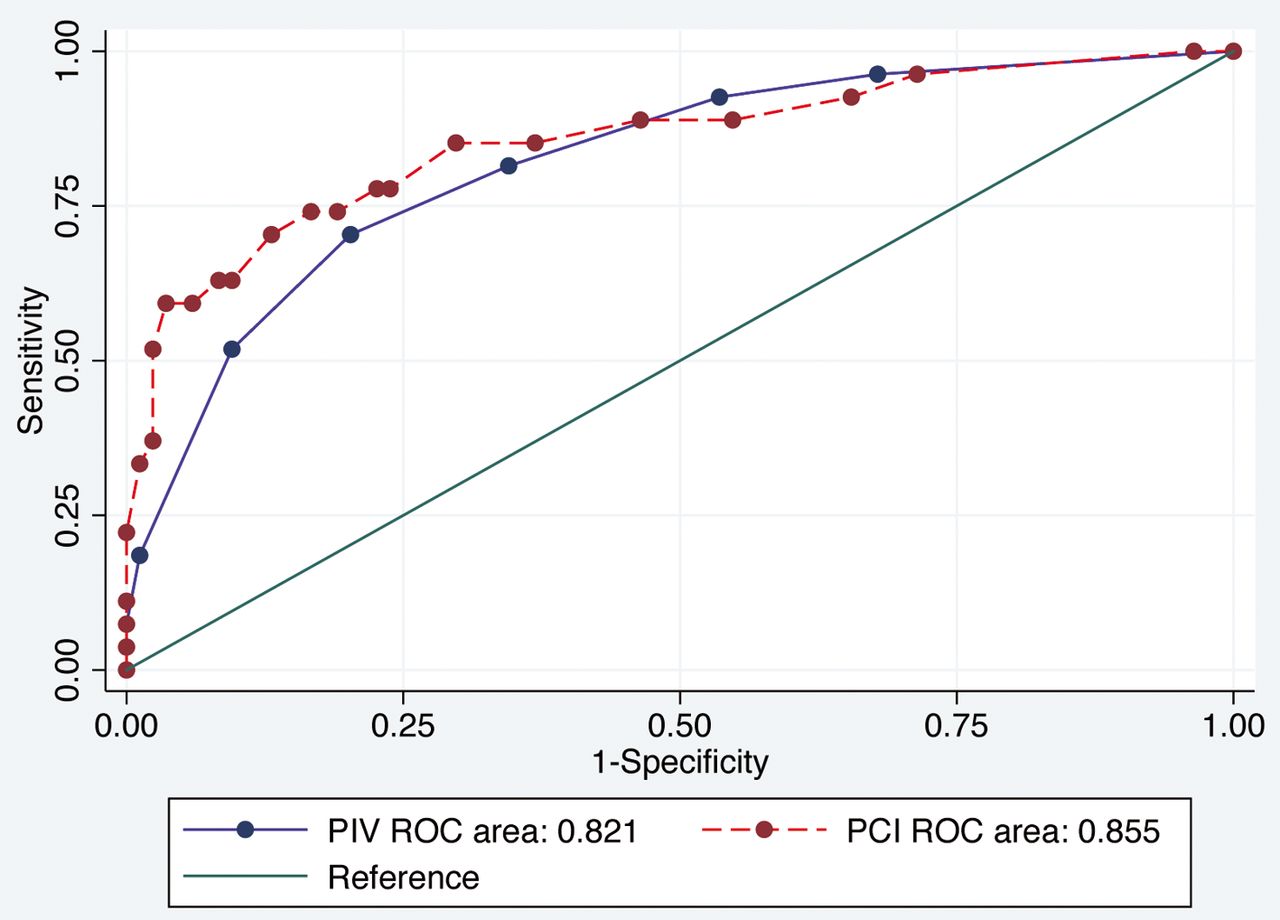
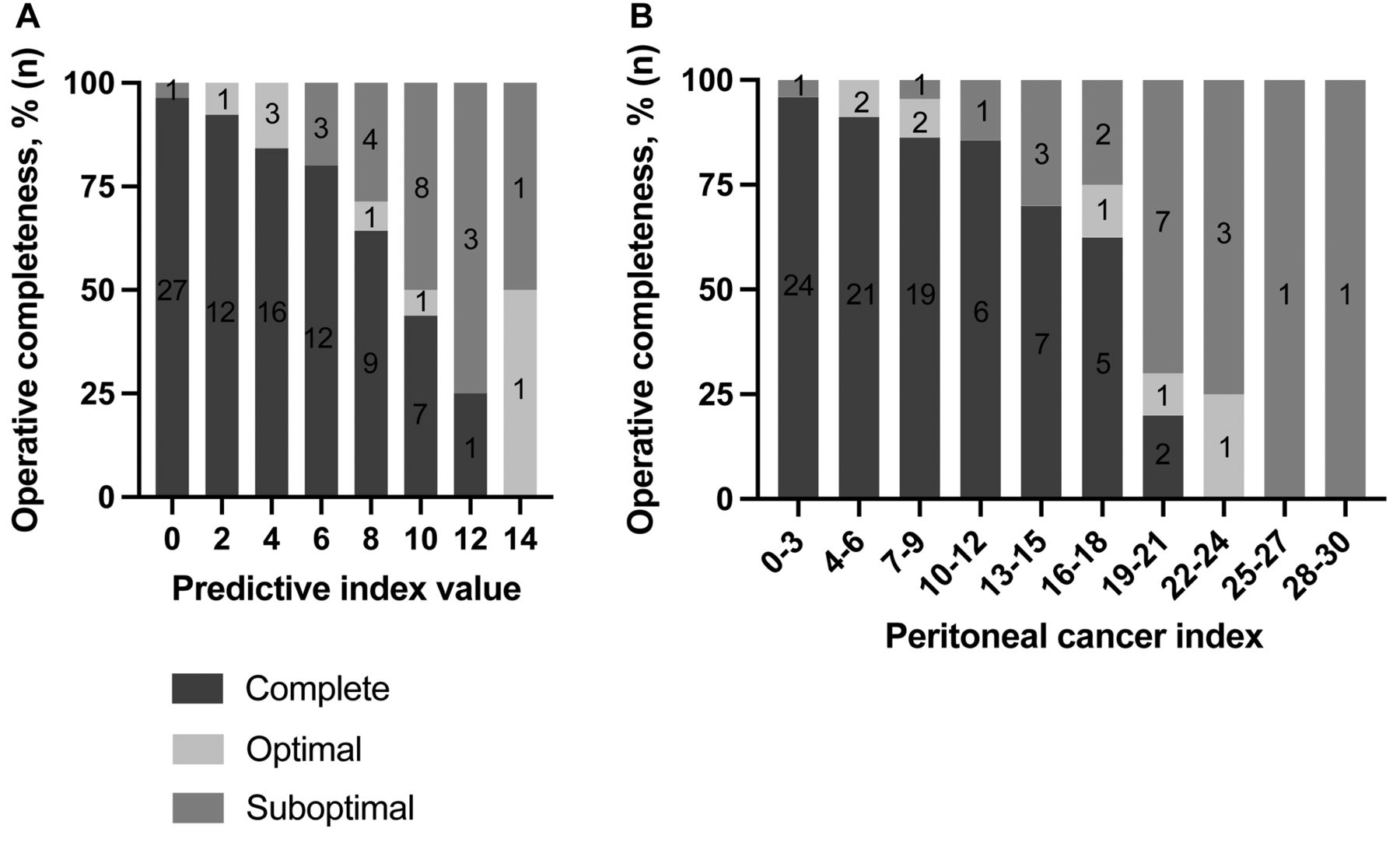
Primary endpoints. The best cutoffs of both scores are shown in Figure 3, and the rates of complete PDS for each category are shown in Figure 4A and B. A PIV cutoff value ≥8 was determined as the best predictor of incomplete PDS [area under the curve (AUC)= 0.821; 95%confidence interval (CI)=0.731-0.911; sensitivity, 70.4%; specificity, 79.8%; positive predictive value, 52.8 %; negative predictive value, 89.3%] (Figure 3). The rate of complete PDS among patients with PIV ≤6 was significantly higher than that in those with PIV ≥8 (89.3% vs. 47.2%; p<0.05). Complete PDS was achieved in 64.3% of patients even with a PIV of 8 (Figure 4A). Additionally, a PCI cutoff value ≥13 was determined as the best predictor of incomplete PDS (AUC=0.855; 95%CI=0.763-0.947; sensitivity, 74.1%; specificity, 83.3%; positive predictive value, 58.8%; negative predictive value, 90.9%) (Figure 3). The rate of complete PDS among patients with PCI ≤12 was significantly higher than that in those with PCI ≥13 (90.9% vs. 41.2%; p<0.05). Complete PDS was achieved in 62.5%-70% of patients, even in those with PCI between 13 and 18 (Figure 4B).

Optimal cutoff values of predictive index value (PIV) and peritoneal cancer index (PCI) for the prediction of incomplete PDS. A PIV cutoff value ≥8 was determined as the best predictor of incomplete PDS (AUC=0.821; 95%CI=0.731-0.911; sensitivity, 70.4%; specificity, 79.8%; positive predictive value, 52.8%; negative predictive value, 89.3%), whereas a PCI cutoff value ≥13 was determined as the best predictor of incomplete PDS (AUC=0.855; 95%CI=0.763-0.947; sensitivity, 74.1%; specificity, 83.3%; positive predictive value, 58.8%; negative predictive value, 90.9%). PIV: Predictive index value; PCI: peritoneal cancer index; PDS: primary debulking surgery.
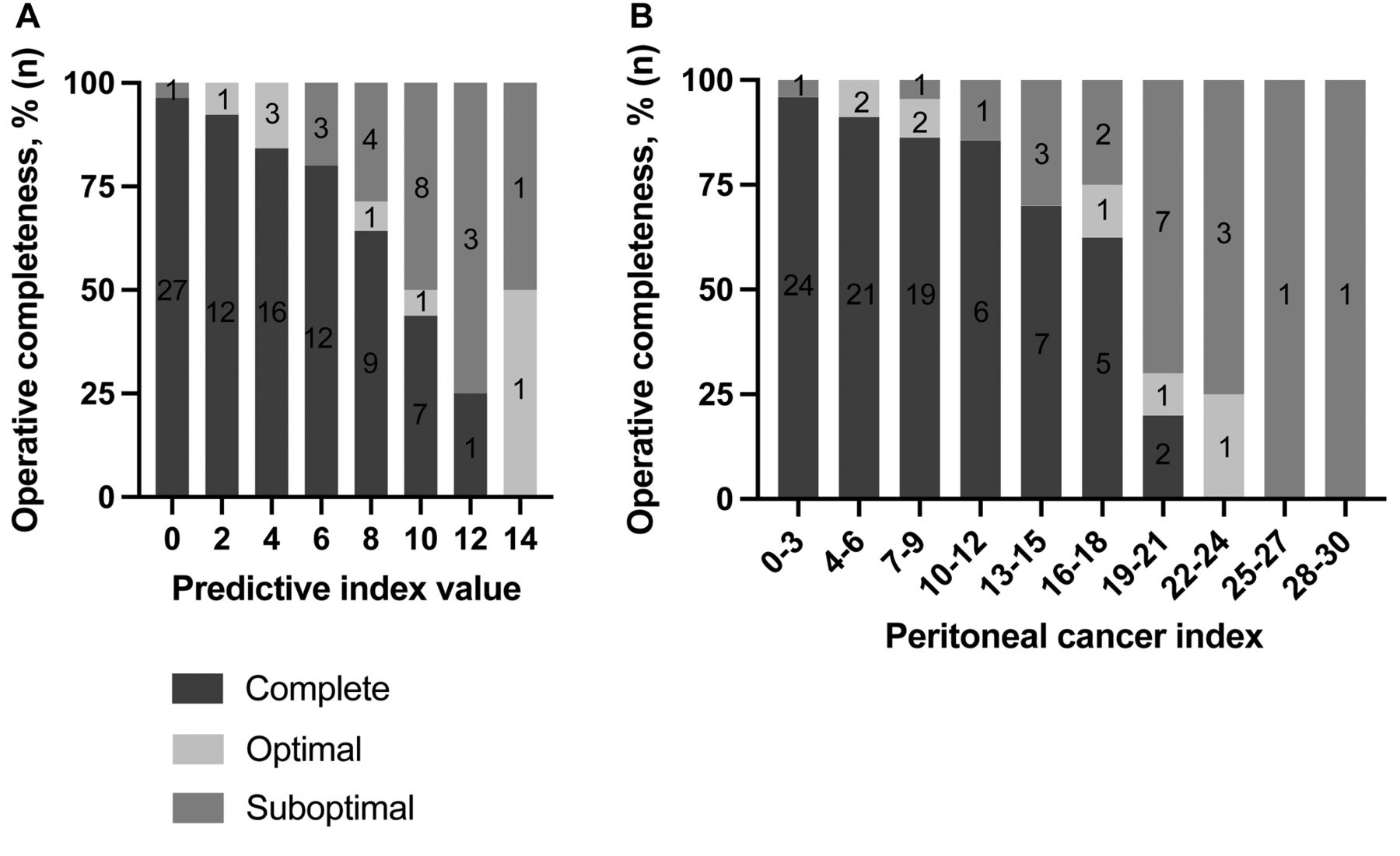
Operative outcomes and distribution of PIV and PCI. (A) The rate of complete surgery among patients with PIV ≤6 is significantly higher than that among patients with PIV ≥8 (89.3% vs. 47.2%: p<0.05). (B) Additionally, the rate of complete surgery among patients with PCI ≤12 is also significantly higher than that among patients with PCI ≥13 (90.9% vs. 41.2%: p<0.05). No case had PCI ≥31 points. Operative completeness is shown as the rate of residual tumor burden after primary debulking surgery (complete, optimal, or suboptimal surgery) presented as percentage (%). The number of patients is presented in the column of each operative category (n). PIV: Predictive index value; PCI: peritoneal cancer index.
Secondary endpoints. A strong correlation was found between PIV and PCI (correlation coefficient=0.899; p<0.05). The clinicopathological features of the groups under and over the cutoffs are shown in Table II and Table III. The patients with PIV ≥8 or PCI ≥13 had significantly higher preoperative CA125 levels, rate of positive ascites, and FIGO stage, whereas no significant differences were found in age and histology. In the further analysis, four cases ended in suboptimal surgery with lower than either cutoff for PIV or PCI. The findings of tumor disseminations in these patients are shown in Table IV. Among the four cases, three had deep tumor infiltrations to retroperitoneal organs (ureters, bladder, and vertebrae), which were not detected on preoperative imaging tests and could not be assessed by PIV and PCI. One case had widespread mesenteric retractions and disseminations in the small bowel that were not detected on preoperative imaging examinations.
Clinicopathological features of patients under and above the cutoff value of PIV=6.
Clinicopathological features of patients under and above the cutoff value of PCI = 12.
Suboptimal surgery cases with PIV ≤ 6 or PCI ≤ 12.
Discussion
Several previous studies developed scoring systems for predicting operative results in PDS for patients with AOC (16, 18-21). Among them, the predictive value has been mainly focused on suboptimal surgery, and the data on their predictive values for complete PDS are controversial. Our analysis showed that PIV ≤6 and PCI ≤12 had reliable predictive values for complete PDS.
The study by Fagotti et al. (22) on operative outcomes in PDS and PIV concluded that, at PIV ≥8, the rate of complete and optimal surgery was less likely at their institution. One retrospective analysis showed that PIV was not reliable in the prediction of complete PDS (AUC=0.51) (16), whereas another prospective study showed that PIV had a moderate predictive value (AUC=0.702) (23). However, our retrospective study found that PIV was highly predictive (AUC=0.821) for complete PDS and determined a cutoff value of ≤6. Thus, PIV can be a valuable tool in predicting complete PDS. Regarding the operative outcomes in PDS and PCI, several studies showed that patients with PCI ≤10 had a higher rate of complete PDS (over 90%) than those with PCI >10 (16, 24). A prospective study by Elzarkaa et al. (25) showed that the rate of complete PDS was 78.6% in patients with PCI ≤13, compared with 26.9% in those with PCI > 13, similar to our results. Thus, PCI seems to be an informative tool for predicting operative results, and the data on its predictive value are consistent between our study and previous ones. According to these considerations, PIV ≤6 and 10 ≤PCI ≤13 seem to be generally useful as predictive indicators for complete PDS.
Furthermore, we found that patients with larger tumor dissemination, PIV ≥8 or PCI ≥13, had higher CA125 levels, rate of positive ascites, and advanced FIGO stage, which is clinically logical. Since the diagnosis and assessment of tumor dissemination in patients with stage IIIA or IIIB are not complicated, these predictive scores should be more important in those with stage IIIC. Therefore, we further conducted a sub-analysis of cases with clinical stage IIIC (Figure 5A and B). In 65 patients with stage IIIC, the rates of complete PDS with each PIV and PCI agreed with the results of the primary analysis, and over 90% of complete PDS was achieved when these scores were under the cutoffs. This sub-analysis showed that both scores were useful for predicting operative outcomes in the subgroup with advanced FIGO stage. Furthermore, although a strong correlation was found between PIV and PCI, the result of the ROC curve for PCI was a little higher than that for PIV. Similarly, two previous reports showed that PCI had a slightly higher predictive value than PIV for complete PDS (16, 23), possibly because PCI has more detailed scoring points on tumor diameter compared with PIV. However, PCI could be underestimated by approximately 2 points in diagnostic laparoscopy compared with that in laparotomy (26). Since our results were based on abdominal findings of disseminations at laparotomy, PCI in diagnostic laparoscopy should be interpreted carefully.

Operative outcomes and distribution of (A) PIV and (B) PCI in patients with FIGO stage IIIC. No case had PCI ≥31 points. Operative completeness is shown as the rate of residual tumor burden after primary debulking surgery (complete, optimal, or suboptimal surgery) presented by percentage (%) and the number of patients presented in the column of each operative category (n). PIV: Predictive index value; PCI: peritoneal cancer index; FIGO: International Federation of Gynecology and Obstetrics.
Diagnostic laparoscopy is performed worldwide as preoperative assessment of unresectable dissemination, such as in the small bowel. Recent reports made a consensus that diagnostic laparoscopy before PDS could decrease futile PDS resulting in suboptimal surgery (13, 27, 28). However, the scoring systems for abdominal dissemination cannot precisely exclude some cases that ultimately resulted in suboptimal surgery, even if the systems indicated that complete and optimal surgery were feasible at PDS. Our evaluation on the limitations of PIV and PCI found four cases with PIV ≤6 that resulted in suboptimal surgery, one of which had massive dissemination in the small bowel and mesentery, and the other three with deep tumor infiltration to retroperitoneal organs. To minimize the cases with PIV or PCI under the cutoff values that result in suboptimal surgery in PDS, we emphasize the importance of preoperative imaging examinations and developing a modified assessment system focusing on the small bowels and mesentery, such as the modified PIV (20). Further investigation is needed to establish a more precise preoperative scoring model that overcomes current limitations and improves the predictive ability by combining data from diagnostic operative features and preoperative imaging, which also might be helpful in the reduction of severe operative complications after PDS (29).
Recently, a new predictive model for complete PDS using artificial intelligence (AI) was reported by Laios et al. and yielded slightly higher accuracy of predicting complete PDS (30). Moreover, to integrate the reliability of these scoring systems at each institution, a free application for calculating PIV and PCI can be made available on the Internet (31). When AI can precisely assess PIV and PCI depending on a movie of laparoscopy for AOC and be linked to such free-access internet applications, these scoring systems become more generalized, and worldwide discussion of these scores for consensus could be held.
This study has some strengths. First, our study was one of the largest studies conducted with more than 100 eligible patients. Second, since we assessed both PIV and PCI, we can provide valuable data on the correlation and limitations of these scores. Contrarily, our research also has several limitations. First, because we gathered the data about disseminations by referring to operative and pathological records, we should recognize the possibility of an underestimated extent of disseminations. Second, because of the retrospective design, a selection bias can exist in the selection of therapeutic options, meaning that eligible patients tended to have a smaller degree of abdominal dissemination and those with larger disseminations on preoperative imaging examinations or diagnostic surgeries who were candidate for NAC+IDS could be substantively excluded. Third, since the skills and maximal effort in the surgical procedure are thought to be important for a safe and sufficient complete PDS (32), we should recognize the existence of this uncontrollable bias between each facility. In the consideration of over 70% of the complete PDS rate in our institutions, our results might be applied to other high-volume hospitals specializing in PDS. Finally, although PIV was originally designed for the laparoscopic prediction model of suboptimal surgery, we applied it in laparotomy. Therefore, a prospective study using PIV and PCI should be conducted to assess the relationship between the extent of disseminations in both laparoscopic and laparotomic findings and operative outcomes.
Conclusion
PIV and PCI, quantitative scoring systems for abdominal tumor disseminations, may be valuable in predicting operative completeness in AOC. Further multicenter prospective studies will be needed to validate the predictive values of these scores.
Acknowledgements
The Authors would like to thank Enago (www.enago.jp) for the English language review.
Footnotes
Authors’ Contributions
SH initiated the concept, collected and analyzed the patient’s data, and wrote the first draft. KU and SO initiated the concept, interpreted the data, supported the implementation of this study and revised the first draft. KO supported and gave comment on the statistical analysis and revised the draft. HK and TS supported the data collection and data analysis. MT, MS, KY, and HT also gave critical comments on the interpretation and revised the draft. YI and NY gave critical comments on the study design and interpretation and revised the draft. AO revised the draft and supervised this project. All Authors approved the final manuscript
Conflicts of Interest
The Authors declare that they have no competing interests related to this study.
- Received October 24, 2021.
- Revision received November 11, 2021.
- Accepted November 12, 2021.
- Copyright © 2022 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}