


Abstract
Background/Aim: We compared three-dimensional conformal RT (3D-CRT), intensity-modulated radiotherapy (IMRT), and volumetric modulated arc therapy (VMAT) for gastric mucosa-associated lymphoid tissue (MALT) lymphoma using four-dimensional computed tomography (4D-CT) images. Patients and Methods: Three treatment plans of 3D-CRT, IMRT, and VMAT with 30 Gy were created based on 4D-CT images of seven patients. We calculated D95, homogeneity index (HI), and conformity index (CI) of planning target volume, and organs at risk doses. Results: There was no significant difference among the three plans in D95. HI of the IMRT plan was significantly better than that of the VMAT (p=0.047) and 3D-CRT (p=0.047) plans. CIs of the IMRT and VMAT plans were significantly better than those of the 3D-CRT plan (p=0.047 and p=0.047, respectively). Dmean of the liver for 3D-CRT was significantly higher than that for the IMRT (p=0.047) and VMAT (p=0.047) plans. Conclusion: The IMRT plan yields the best plan quality for gastric MALT lymphoma.
- Gastric mucosa-associated lymphoid tissue lymphoma
- radiotherapy
- planning study
- intensity-modulated radiotherapy
- volumetric modulated arc therapy
- four-dimensional computed tomography
- respiratory motion
Gastric mucosa-associated lymphoid tissue (MALT) lymphoma is an indolent B-cell lymphoma, which can arise in almost all organs, but the stomach is the most frequent site. Stage IE accounts for 70%-80% of all gastric MALT lymphoma cases (1). Radiotherapy (RT) is a curative treatment for localized gastric MALT lymphoma and particularly in persisting cases or those with relapse after
Helicobacter pylori (HP) eradication when HP is negative. National Comprehensive Cancer Network (NCCN) guidelines recommend an RT dose of 30 Gy in 20 fractions for the treatment of this condition (2).
The target volume for gastric MALT lymphoma is very large. Clinical target volume (CTV) is defined as the gross tumor volume (GTV) plus whole stomach volume, outlined from the gastroesophageal junction to beyond the duodenal bulb. Furthermore, an additional margin is required to cover variations in stomach size and shape, respiratory motion, and set-up errors (3). As patients with gastric MALT lymphoma have a long-term prognosis, with an approximate 10-year overall survival of 90% (4), late adverse events from RT should be avoided.
The goal of RT for gastric MALT lymphoma is to deliver a sufficient dose to the large target volume while avoiding the organs at risk (OARs), such as the kidneys and the liver. Two-dimensional RT (2D-RT) and three-dimensional conformal RT (3D-CRT) have been traditionally used for the treatment of gastric MALT lymphoma (5). In this decade, intensity-modulated radiotherapy (IMRT) has been increasingly used for the treatment of abdominal tumors (6, 7). IMRT can provide the desired intensity modulation by using several gantry angles and dividing each radiation beam into numerous beamlets whose intensities are adjusted individually (8). More recently, volumetric modulated arc therapy (VMAT) has been introduced for the treatment of various tumors (9). VMAT can provide the full range of beams by gantry rotation, and change the parameters of dose rate, field shape, and speed of gantry rotation as the beam is rotated (8). Some groups performed a planning study and reported that these state-of-the-art RT techniques provide a better dose distribution for gastric MALT lymphoma than that provided by 2D and 3D-CRT (5, 10). However, they performed planning and evaluated plans based on three-dimensional computed tomography (3D-CT) images, which do not contain the information of the respiratory motion, which changes not only the position, but also the shape and volume of the stomach (11, 12). Another group compared 3D-CRT, IMRT, and VMAT under the deep-inspiration breath hold (DIBH) technique and suggested the dosimetric superiority of IMRT and VMAT over 3D-CRT (13). However, DIBH can only be performed in a limited number of institutions.
Four-dimensional computed tomography (4D-CT) images, which provide information on the variability of respiratory motion, have been introduced into RT planning. Jang et al. compared the target volume, volume of OARs, and dose distribution of 3D- and 4D-CT images from 18 patients with gastric MALT lymphoma (14). They reported that the target volume and volume of the liver and kidneys, contoured using free-breathing 3D-CT images, were significantly smaller than those contoured using 4D-CT. The reason for this was that the respiratory motion of the target volume and OARs is not reflected into free-breathing 3D-CT images. They also found that 3D-CT image-based planning may result in inadequate dose coverage of the target volume and OAR dose underestimation. The International Lymphoma Radiation Oncology Group recommends determining the target volume by 4D-CT or by fluoroscopy, to track variations in stomach position during respiration (3). However, to our knowledge, the plan quality of modern treatment techniques has not been evaluated and compared based on 4D-CT images.
The purpose of this study was to evaluate and compare the quality of 3D-CRT, IMRT, and VMAT plans for gastric MALT lymphoma patients based on 4D-CT images.
Patients and Methods
Patients. This retrospective study was approved by the institutional research ethics board of our hospital. All patients were enrolled with prior written informed consent to treatment and the use of image data. We used 4D-CT images of seven patients with stage IE gastric MALT lymphoma who received RT at our institution between February 2019 and June 2020.
CT simulation procedures. To minimize variations in stomach volume, patients were instructed to fast for at least eight hours before planning simulation. They underwent CT simulation by using a Discovery RT CT scanner (GE Healthcare, Chicago, IL, USA) in the supine position with their arms raised. 4D-CT scan was performed using a Smart Deviceless 4D application with the parameters of 120 kV, 70 mA, a gantry rotation time of 0.5 s, a slice thickness of 2.5 mm, and cine mode (15). The cine durations were set to the respiratory cycles plus the gantry rotation time, and the cine images were sorted into 10 respiratory phases by a phase-binning algorithm. The average intensity projection (AIP) of CT images was generated from projection data of all respiratory phases. All CT images were exported to the treatment planning system (Eclipse, Version 15.6; Varian Medical Systems, Palo Alto, CA, USA) and registered by the hardware arrangement.
Definition of target volumes and OARs. Two radiation oncologists with an experience of 5 and 17 years defined the target volumes and OARs, after reaching a consensus according to the Radiation Therapy Oncology Group contouring atlases (16). In all patients, GTV was identified based on the endoscopic examination findings, and we confirmed that GTV was contained within the whole stomach. The CTV was defined as the whole stomach, which was delineated on the AIP CT image data sets using fused 4D-CT images to cover the stomach in all 10 respiratory phases (CTV-4D) (15). A margin of 10 mm, which included intra- and inter-fractional variations in the stomach volume, respiratory movement, and patient set-up, was added to CTV-4D for generating the planning target volume (PTV) (3, 17). OARs defined as the kidneys, liver, small bowel, and spinal cord were also delineated on the AIP CT images (15).
Treatment planning procedures. 3D-CRT, IMRT, and VMAT plans were generated based on AIP CT images. The 3D-CRT plan consisted of four beams (gantry angles of 0˚, 90˚, 180˚, and 270˚) with 15-MV X-ray. Multileaf collimator apertures were created, encompassing the PTV with a 5 mm margin in all directions. The IMRT plan using sliding window technique consisted of seven beams (gantry angles of 24˚, 75˚, 126˚, 177˚, 231˚, 282˚, and 333˚) with 6-MV X-ray. The VMAT plan consisted of a double arc of 360˚ with 6-MV X-ray (13). The prescribed dose was 30 Gy in 20 fractions. The goal of each plan was as follows: the minimum coverage dose for 95% of the PTV (D95), > 95% of the prescribed dose, mean dose (Dmean) of the liver <12.5 Gy, Dmean of each kidney <10 Gy, maximum dose (Dmax) of the spinal cord <30 Gy, and Dmax of the small bowel <31.5 Gy (13). The dose calculation was performed with the anisotropic analytical algorithm and a gird size of 2.5 mm.
Dosimetric parameters for plan evaluation. Each plan was analyzed using a dose-volume histogram (DVH). The PTV coverage was evaluated base on D95. The homogeneity index (HI) of the PTV was calculated as follows (18):

where D1 and D99 are the minimum dose covering 1 and 99% of the PTV, respectively; and Dp is the prescription dose. The lower HI suggests a better homogeneity.
The conformity index (CI) of the PTV was calculated as follows (13):

where BV95 is the volume of the body receiving 95% of the prescribed dose. The closer CI is to 1, the better conformity.
The OAR dose was evaluated by the Dmean for parallel organs (kidneys and liver), and the Dmax for serial organs (small bowel and spinal cord).
We used an RT plan analysis software; Plan IQ (Version 2.3.2; Sun Nuclear, Melbourne, FL, Australia), which obtains a comprehensive and objective assessment of treatment plans by calculating the plan quality metric (PQM). The PQM score settings were based on previous reports and clinical importance (Table I) (13, 18). The PQM score (%) was calculated as follows (13):

Plan quality metric scores for each dosimetric parameter.
where PQMraw means the total score of each dosimetric parameter, and PQMmax means the sum of the perfect score of each dosimetric parameter, which was set to 120.
Statistical analysis of dosimetric parameters. For the comparison of treatment plans, the Friedman test was used for analysis of variance (ANOVA), and the Wilcoxon signed-rank test was used for post-hoc analysis with a Bonferroni correction. Differences with p-values of <0.05 were considered to be statistically significant. Statistical analyses were performed with the SPSS software (Version 26.0; IBM, Armonk, NY, USA).
Results
The results of the DVH parameters and the PQM scores of the three treatment plans are shown in Table II. Examples of dose distributions for each plan are shown in Figure 1.
Dosimetric parameters and plan quality metric scores of the three plans (mean±standard deviation).

Examples of dose distributions for (a) 3D-CRT, (b) IMRT, and (c) VMAT. CTV of all respiratory phases (CTV-4D) and PTV are shown in pink and red, respectively. 3D-CRT: Three-dimensional conformal radiotherapy; IMRT: intensity-modulated radiotherapy; VMAT: volumetric modulated arc therapy; PTV: planning target volume.
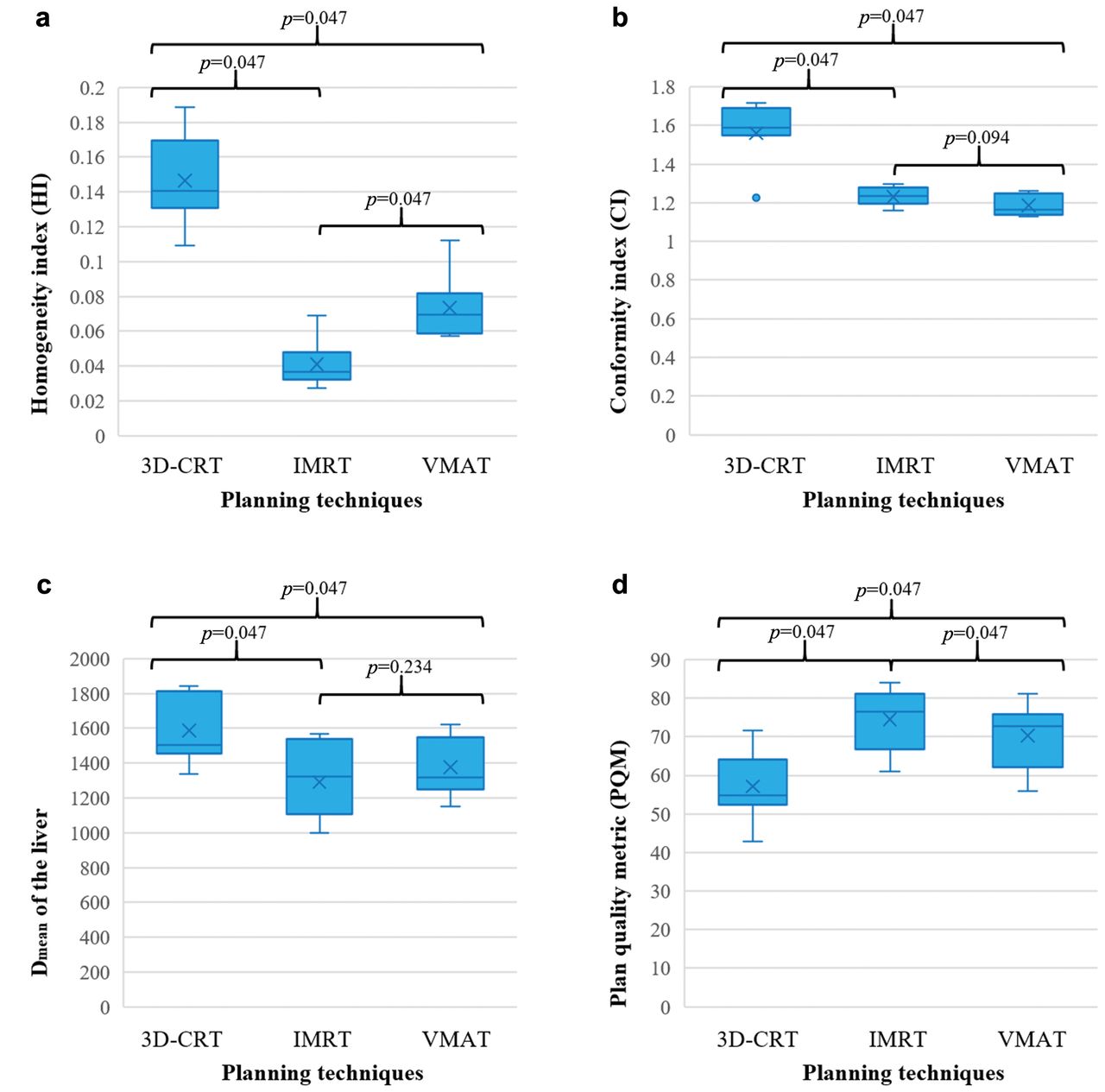
PTV coverage, homogeneity, and conformity. There was no significant difference in D95 among the three plans (p=0.368). The box plots of HI and CI are shown in Figure 2. The HI of the IMRT plan was significantly lower than that of the VMAT (p=0.047) and 3D-CRT (p=0.047) plans. The HI of the VMAT plan was significantly lower than that of the 3D-CRT (p=0.047) plan. CIs of the IMRT and VMAT plans were significantly lower than those of the 3D-CRT plan (p=0.047 and p=0.047, respectively). There was no significant difference in CI between the IMRT and VMAT plans (p=0.094).

Boxplots of the (a) homogeneity index, (b) conformity index, (c) Dmean of the liver, and (d) plan quality metric score for 3D-CRT, IMRT, and VMAT. 3D-CRT: Three-dimensional conformal radiotherapy; IMRT: intensity-modulated radiotherapy; VMAT: volumetric modulated arc therapy.
OAR dose. The box plots of Dmean of the liver are shown in Figure 2. Dmean of the liver for 3D-CRT was significantly higher than that for IMRT (p=0.047) and VMAT (p=0.047). There was no significant difference between the IMRT and VMAT plans in the Dmean of the liver (p=0.234). There was no significant difference among the three plans in the Dmean of the right kidney (p=0.066) and the left kidney (p=0.368), Dmax of the spinal cord (p=0.066), and Dmax of the small bowel (p=0.276).
PQM score. The PQM score box plots are shown in Figure 2. The PQM scores of the VMAT and IMRT plans were significantly higher than that of the 3D-CRT plan (p=0.047 and p=0.047, respectively). The PQM score of the IMRT plan was significantly higher than that of the VMAT plan (p=0.047).
Discussion
Our study based on planning 4D-CT images suggested that the IMRT and VMAT plans have a dosimetric superiority over the 3D-CRT plan, in terms of homogeneity and conformity of the PTV, dose to the liver, and PQM score. Choi et al. performed a planning study to compare four-fields 3D-CRT, seven-fields step-and-shoot IMRT and double arc VMAT in nine patients based on free-breathing 3D-CT images (13). They added an isotropic margin of 15 mm to the whole stomach to account for respiratory movement during treatment and an additional isotropic margin of 5 mm to cover set-up errors. The prescribed dose was 30 Gy in 20 fractions. They reported that the IMRT and VMAT plans provided significantly better CI of PTV and significantly lower Dmax of the spinal cord compared with the 3D-CRT plan, and that other dosimetric parameters were similar among the three treatment plans. By using 4D-CT images, we confirmed a similar tendency, whereby the IMRT and VMAT plans achieved a dosimetric superiority over the 3D-CRT plan in point of appropriate dose to PTV and reduced dose to OARs.
In terms of plan quality superiority among the IMRT and VMAT plans, Choi et al. found no significant difference in PTV coverage, homogeneity, conformity, and OAR doses between the IMRT and VMAT plans. On the other hand, our results suggested that the IMRT plan provides better dose distributions than the VMAT plan in terms of homogeneity of the PTV and PQM score. A possible reason for the difference between their result and ours is a difference in our definitions of the target volume. Unlike the study by Choi et al., we defined target volumes based on 4D-CT images. Respiratory movement is not isotropic; Uchinami et al. estimated the motion of the stomach in 10 patients with gastric lymphoma using 4D-CT and reported that the average respiratory amplitudes of the centroid stomach were 4.1 mm, 2.9 mm, and 10.1 mm in the anterior-posterior, left-right, and superior-inferior direction, respectively (12). Another possible reason is that Choi et al. used the step-and-shoot technique, while we used a sliding window technique for the IMRT plan. It is reported that sliding window IMRT provides better plan quality compared with step-and-shoot IMRT under certain conditions (19).
Although VMAT had been introduced after IMRT, the results of the previous reports on dosimetric superiority of these techniques are conflicting between the studies. Yoo et al. compared seven-field IMRT with single and double arc VMAT in ten prostate cancer patients with or without pelvic lymph nodes (20). The RT dose of 46.8 Gy was prescribed for primary PTV (PTVP), which contained prostate, seminal vesicles, and pelvic lymph nodes. It was followed by an RT dose of 28.8 Gy for boost PTV (PTVB), which contained prostate and seminal vesicles. For the primary plan, HI and CI of PTVP for the IMRT plan were significantly better than those for the single arc VMAT plan, whereas those for the IMRT plan were similar with those for two arc VMAT plan. The Dmean of the bladder, rectum, and small bowel for the IMRT plan was significantly lower than that for the single and two arc VMAT plans. For the boost plan, the HI of PTVB for the IMRT plan was significantly better than that for the single arc VMAT plan and was almost the same as that for the two arc VMAT plan. The CI of PTVB for the IMRT plan was similar to that for the single arc VMAT plan and was significantly worse than that for the two arc VMAT plan. The Dmean of the bladder and rectum for the IMRT plan was significantly lower than that for the single arc VMAT plan, whereas that for the IMRT plan were similar to that for the two arc VMAT plan. Their results may suggest that the dose distribution of the IMRT plan is superior to that of the VMAT plan in cases where the target volume is large and complex, which is applicable to gastric MALT lymphoma in our study.
The dosimetric superiority of the IMRT plan over the VMAT plan is demonstrated in our study; however, the dose distributions of the VMAT plan were sufficiently better than those of 3D-CRT. The advantages of VMAT over IMRT are confirmed in the shorter treatment time and fewer monitor units (9, 21). Therefore, considering these advantages and the significantly better dose distribution of IMRT and VMAT, these plans could be appropriate for the treatment of gastric MALT lymphoma.
As comparison of the quality of treatment plans requires the evaluation of many DVH parameters, it is difficult to make a direct comparison between treatment plans. To resolve this issue, we used Plan IQ for a comprehensive and objective assessment of the treatment plans. Our results suggested that the PQM score appropriately and comprehensively reflected the tendency of each DVH parameters. This type of RT plan analysis software may be useful to improve and evaluate the quality of treatment plans.
There are some limitations to our study. Firstly, it was a single center retrospective study with a relatively small sample size. Secondly, as this is a planning study, the effects of respiratory motion, such as deformation of the structures and the interplay effect in a real clinical setting, on the dose distribution were not considered (22, 23). Similarly, the clinical superiority of IMRT and VMAT over 3D-CRT was not demonstrated and further studies are underway to address issues.
Conclusion
In this planning study, we compared the quality of the 3D-CRT, IMRT, and VMAT plans for patients with gastric MALT lymphoma based on 4D-CT images. The IMRT and VMAT plans had a dosimetric superiority over the 3D-CRT plan in terms of homogeneity and conformity of the PTV, dose to the liver, and PQM score. The IMRT plan provides better dose distributions than the VMAT plan in terms of homogeneity of the PTV and PQM score. Considering the advantages of VMAT over IMRT in terms of shorter treatment time and fewer monitor units, we recommend the implementation of the IMRT and VMAT plans, rather than 3D-CRT, for patients with gastric MALT lymphoma.
Footnotes
This article is freely accessible online.
Authors’ Contributions
TM developed the study design; collected, analyzed, and interpreted data; performed statistical analysis; and drafted the manuscript. RT developed the study design; collected, analyzed, and interpreted data; and revised the manuscript. YS developed the study design; performed radiotherapy planning; and collected, analyzed, and interpreted data. TW and YK developed the study design; collected and interpreted data. TM, TS, YF, and NO developed the study design and interpreted data. All Authors have read and approved the final manuscript.
Conflicts of Interest
The Authors declare that they have no conflicts of interest related to this study.
- Received June 17, 2021.
- Revision received July 3, 2021.
- Accepted July 5, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Influence of Respiratory Motion on Dose Distribution in Gastric Mucosa-associated Lymphoid Tissue Lymphoma Radiotherapy
- Long-term Outcomes of Early-stage Non-stomach Gastrointestinal Mucosa-associated Lymphoid Tissue Lymphoma Treated With Radiation Therapy
- Implementation of 99mTc-GSA SPECT Image-guided Inverse Planning into Palliative Radiotherapy for Diffuse Liver Metastases: A Novel Approach