


Abstract
Background/Aim: Pathological fractures are rare, suspicious and in some cases mentioned as the first sign of a malignant tumor. We present an uncommon case with a pathological fracture of the tibia diaphysis as the first sign of severe hyperparathyroidism. Case Report: We report the case of a female patient who was referred to the emergency department with a history of progressively worsening pain in the lower left leg and an inability to fully bear weight. No history of trauma or any other injury was reported. An x-ray revealed an extensive osteolytic lesion in the tibial shaft with cortical bone destruction. Conclusion: Our case, together with very few cases described in the current literature, emphasizes that in the presence of hypercalcemia and lytic lesions primary hyperparathyroidism should always be considered as a differential diagnosis. Lytic bone lesions can lead to pathological fractures and severe impairment of quality of life.
Bone disease in severe primary hyperparathyroidism (PHPT) is described as osteitis fibrosa cystica (OFC). It was first described by von Recklinghausen in 1891 (1). However, at first von Recklinghausen did not suspect a relationship between OFC and a disease of the parathyroid glands (2). Despite the fact that OFC is a highly rare and uncommon condition, clinically it is characterized by bone pain and radiographically by subperiosteal bone resorption, osteolysis of the distal clavicles, a “salt and pepper” appearance of the skull, bone cysts, and brown tumors of the bones (3).
Primary hyperparathyroidism (PHPT), also known as “brown tumor”, also involves unifocal or multifocal bone lesions, which represent a terminal stage of hyperparathyroidism-dependent bone pathology (4). This focal lesion is not a real neoplasm. In localized regions where bone loss is particularly rapid, hemorrhage, reparative granulation tissue, and active, vascular, proliferating fibrous tissue may replace the healthy marrow contents, resulting in a brown tumor.
Histologically, the tumor shows bland spindle cell proliferation with multinucleated osteoclastic giant cells and signs of bone resorption. The brown coloration is due to hemosiderin-laden macrophages. Multiple bony lesions representing brown tumors are often misdiagnosed as metastatic carcinoma, bone cysts, osteosarcoma, or giant-cell tumors. Histomorphologically, they might show high resemblance. Clinical information concerning hypercalcemia, hyper - phosphatemia and hyperparathyroidism is indispensable for pathologic diagnosis and differentiation from giant cell tumor of the bone (5). Since the radiological features (e.g., cyst-like radiolucency) overlap and can be characteristic of these other diseases, diagnosis can be difficult (6-8). Parathyroidectomy is the treatment of choice in severe PHPT (9).
We report a case of primary hyperparathyroidism in which the first clinical manifestation of the disease was a pathological fracture of the tibia that masqueraded as a malignancy. The presence of large osteolytic lesions gave rise to the initial diagnosis of primary or metastatic cancer. Declaration of patient consent. All appropriate patient consent forms were obtained. In the form, the patient gave her consent for her images and other clinical information to be reported in the journal. The patient understands that neither her name nor her initials will be published and due efforts will be made to conceal her identity, but that anonymity cannot be guaranteed.
Case Report
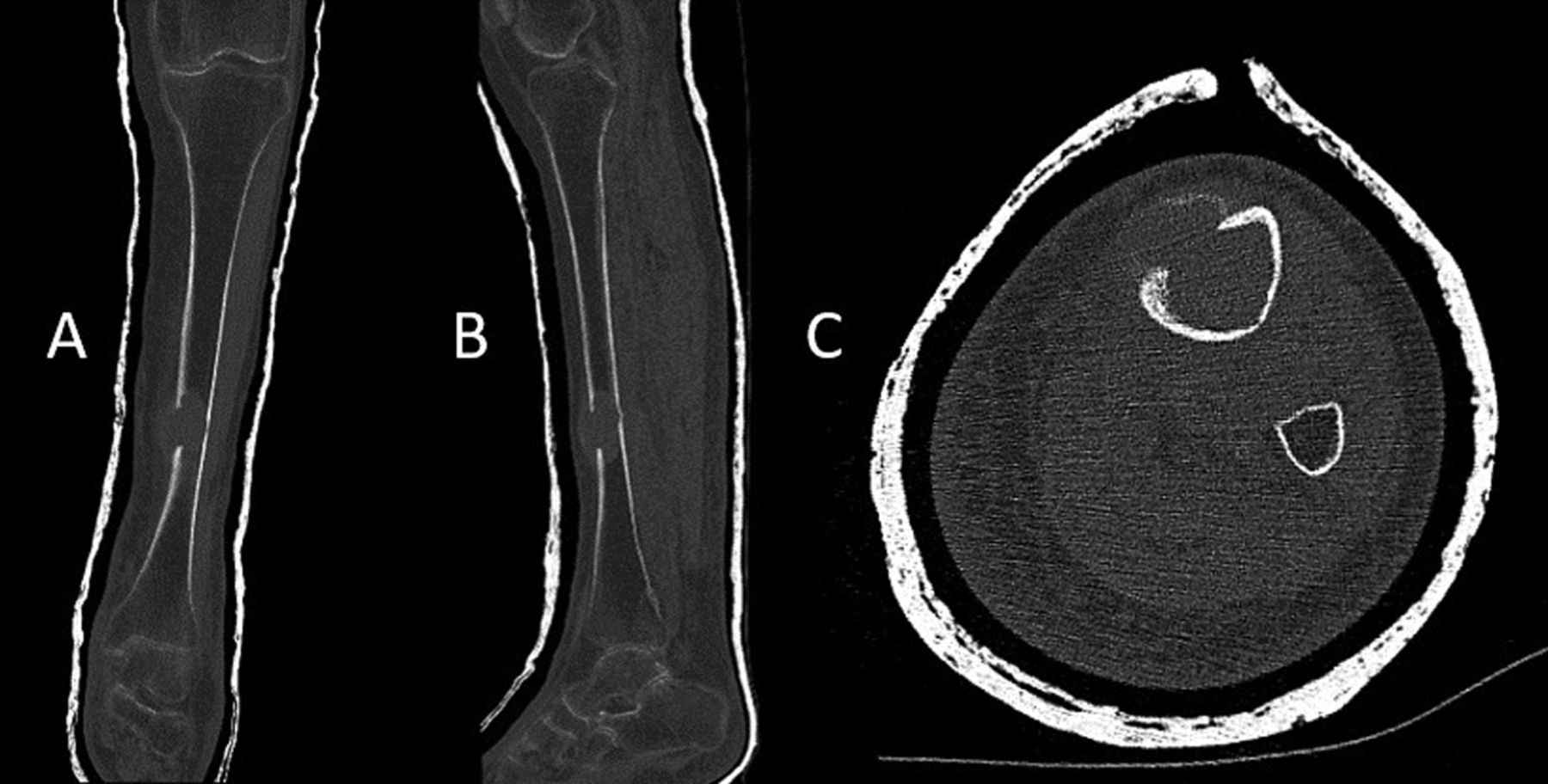
An 88-year-old Austrian Caucasian woman was referred to the emergency department with a history of progressively worsening pain in the left lower leg and inability to fully bear weight on the affected side. The patient reported no history of trauma, fall, or any other injury. An x-ray revealed an extensive osteolytic lesion in the tibial shaft with cortical bone destruction along with moth-eaten features (Figure 1). The patient had no history of weight loss, fever, or night sweats and had a negative family history for any tumors or disorders of calcium homeostasis. However, severe malnourishment and a cachectic nutritional condition were apparent. Despite her advanced age, the patient had no medical record of relevant pre-existing illnesses, and apart from inpatient stays for hip arthroplasty, the patient had never been in inpatient medical treatment. She lived alone at home, looked after by 24-h care, and was independently mobile with a rollator. Computed tomography (CT) scan showed a pathological fracture of the tibia in the distal third, with no dislocation. At the level of the pathological fracture, an approx. 4.7×2.7 cm malignant bone lesion with approx. 23×14 mm osteolysis on the ventral tibial corticalis, osseous thinning/beginning osteolytic dissolution of the dorsal tibial corticalis, and extraosseous soft tissue components with marginal calcification of the extraosseous soft tissue component were observed. Further distal (approx. 5.7 cm above the ankle joint), a second osteolysis of the medial tibial corticalis measuring approx. 17×7 mm was seen, with accompanying soft tissue components, indicating a differential diagnosis of bone metastases or plasmacytoma (Figure 2). Initially, the fracture was stabilised with a leg cylinder cast and the patient was referred to a tertiary orthopaedic oncological center for further treatment and diagnostic findings.

X-ray with an anterior-posterior view (A) and lateral view (B) of the osteolytic lesion in the tibial shaft with cortical bone destruction along with moth-eaten features.
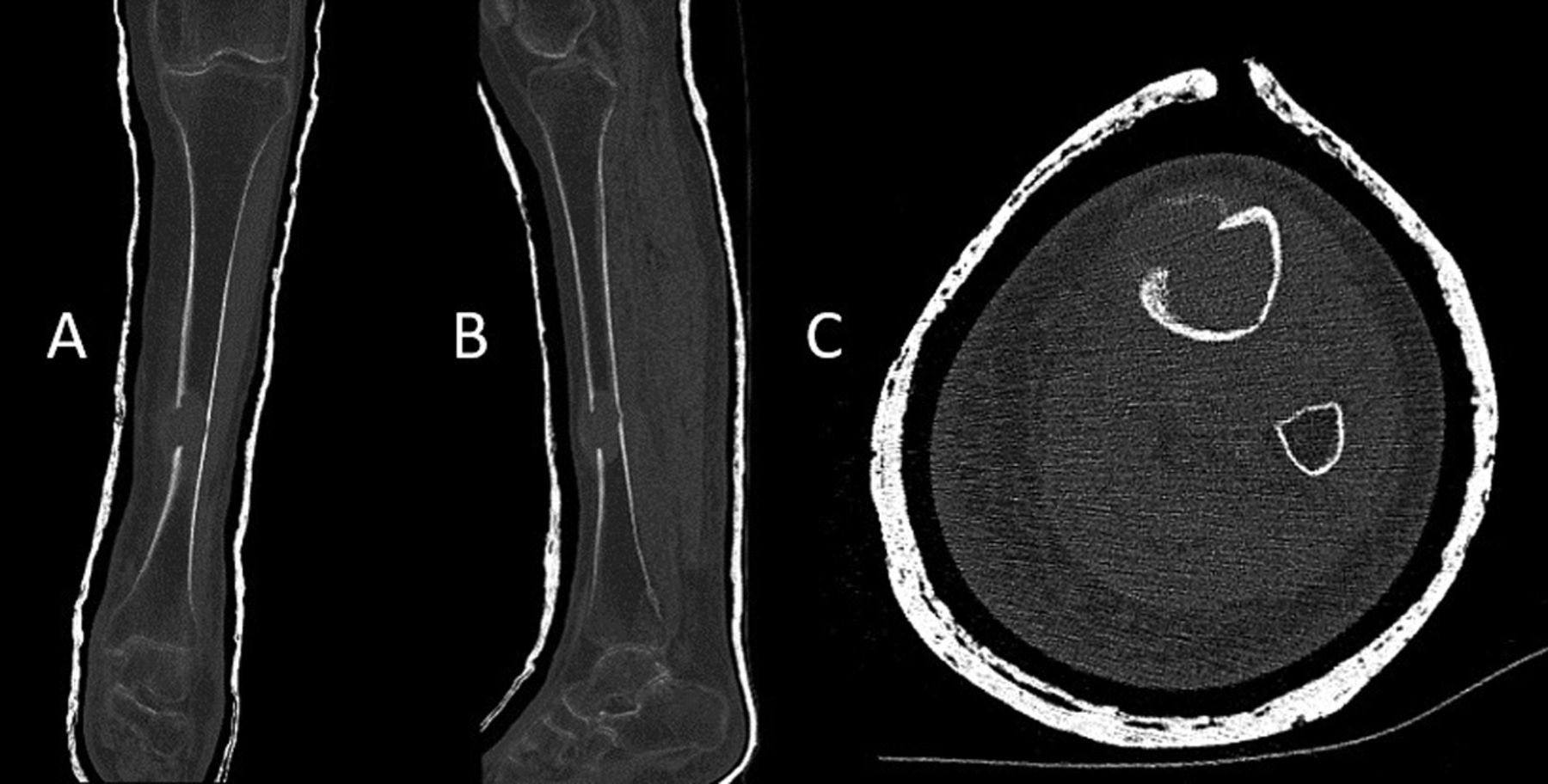
CT scan with coronary (A), sagittal (B) and axial (C) view of the bone lesion in the tibial shaft with soft tissue components. Soft tissue involvement can be clearly seen.
Due to the pathological fracture, a haemato-oncological consultation was performed, as well as a sonographically targeted biopsy with further laboratory investigation. A whole-body CT scan as well as a CT scan of the skull and neck were performed, which revealed inhomogeneous texture of the cranial bone with numerous osteolytic destructions of the Tabula interna on both sides with small osteolytic defects also in the rest of the calvaria and minor osseous inhomogeneities in the mandible. No primary thoracic or abdominal malignancy was evident. Thus, radiologically the differential diagnosis of multiple myeloma was established.
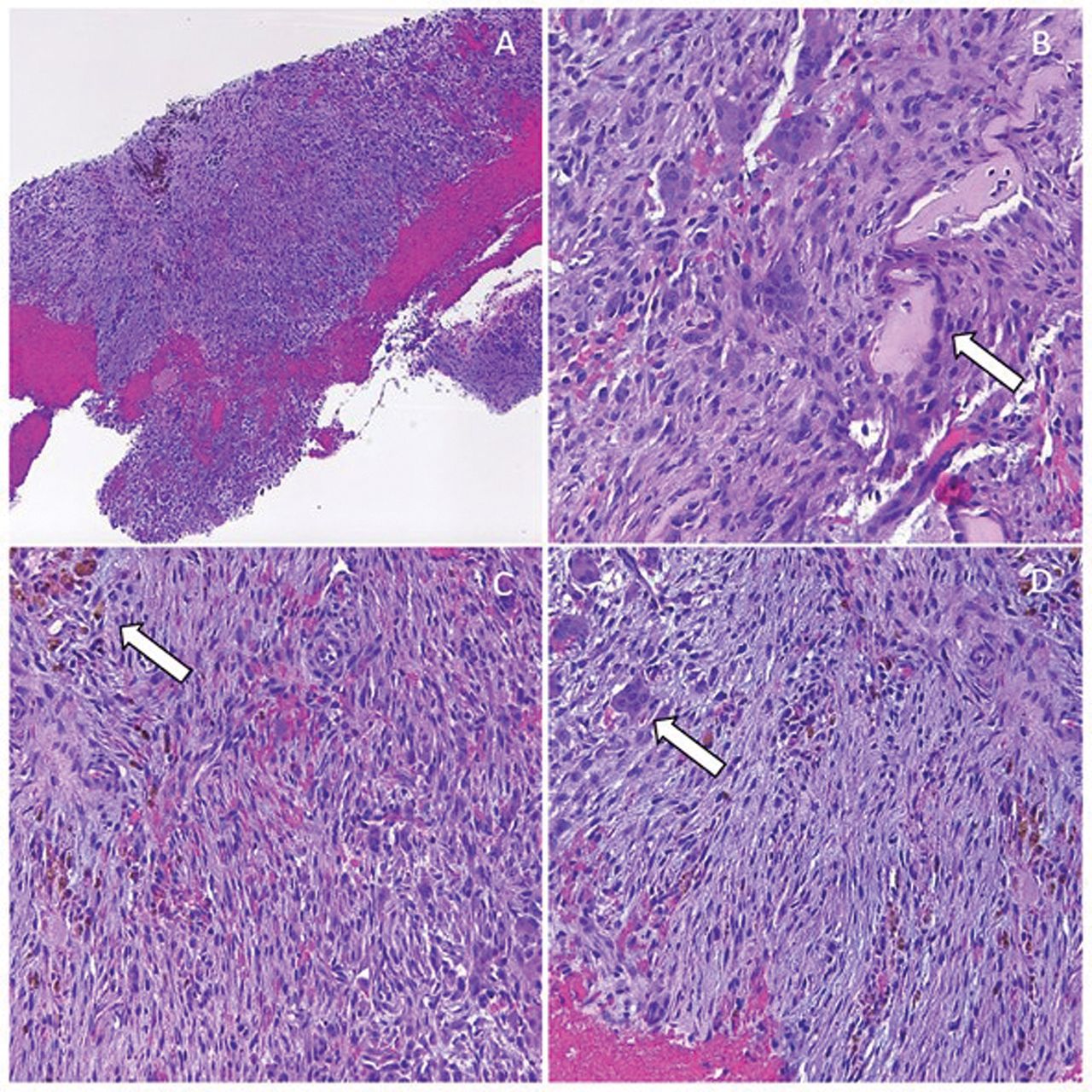
However, the bone biopsy was consistent with a brown tumor, differential diagnostic giant cell tumor, or aneurysmatic bone cyst. The laboratory tests showed clearly deflected laboratory parameters with highly elevated parathyroid hormone (PTH) levels, lowered vitamin D3 levels, lowered folic acid levels, and lowered vitamin B12. In detail, PTH was highly elevated at 1,224 pg/ml (norm 15-65 pg/ml), while serum calcium was only slightly elevated at 2.60 mmol/l (norm 2.20-2.55 mmol/l). Serum phosphorus was 0.5 mmol/l (norm 0.81-1.45 mmol/l), albumin was 3,030 mg/dl (norm 3560-4,610 mg/dl) and alkaline phosphatase activity was 676 IU/l (norm 35-104 IU/l). In view of the given laboratory findings, careful re-evaluation of the biopsy indicated a brown tumor (Figure 3). Endocrinological, gastrological, and dental consultation were performed and previously unknown hyperparathyroidism with normocalcemia, vitamin D deficiency, and latent hypothyroidism was diagnosed.

Histology of bone biopsy shows brown tumor with bland spindle cell proliferation, brown pigmentation, multinucleated giant cells, signs of bone resorption and haemorrhage. A) biopsy overview in HE at 50×, B) signs of bone resorption, HE 100×, C) brown pigmentation in macrophages, HE 100×, D) multinucleated giant cells, HE 100×.
The patient was presented to the interdisciplinary orthopaedic-oncological board and in a synopsis of the clinical, radiological as well as pathological, and laboratory findings, the decision was made for surgical treatment with an intramedullary nail osteosynthesis (Figure 4). Vitamin D was substituted.
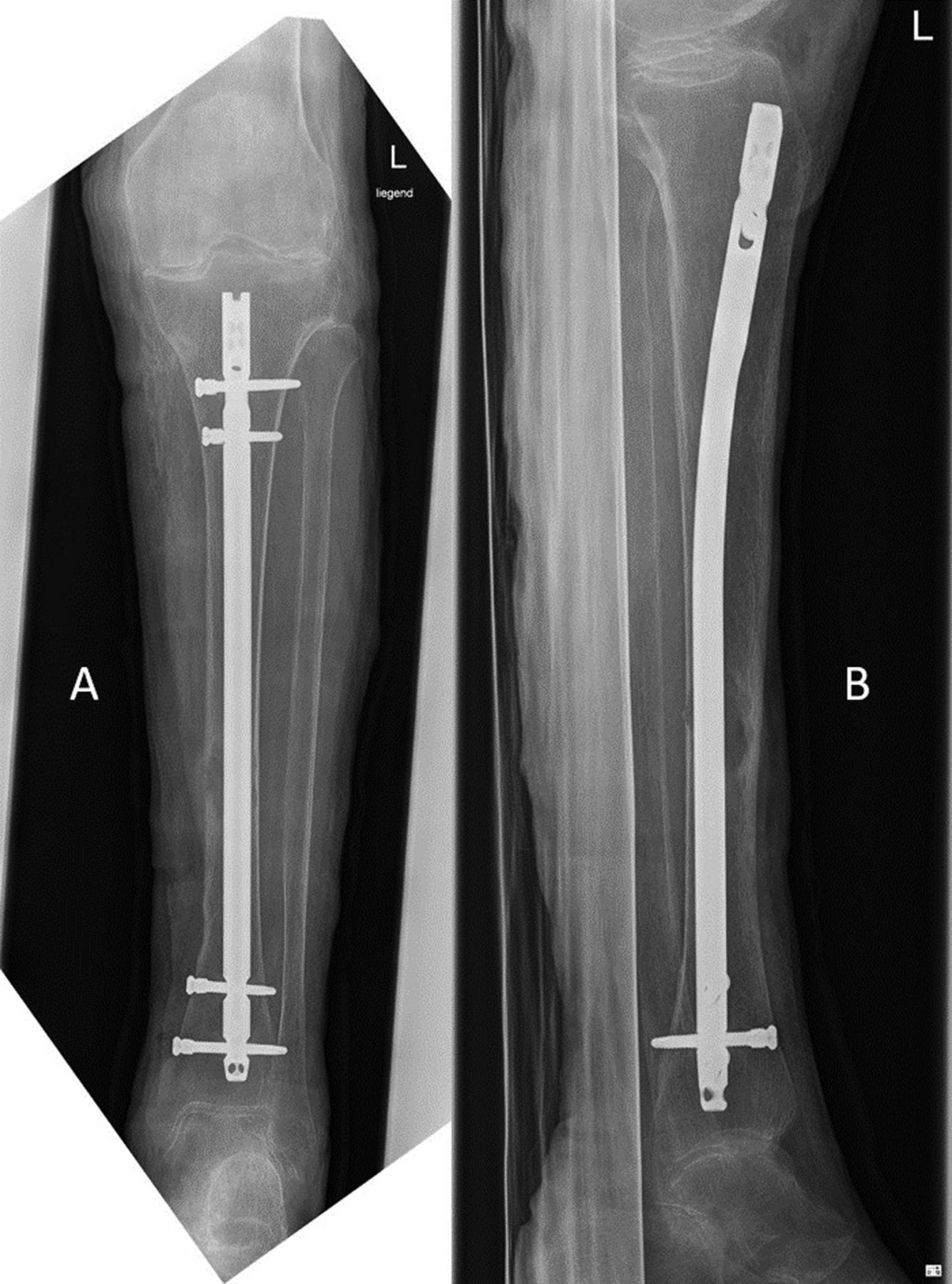
X-ray with an anterior-posterior view (A) and lateral view (B) after implantation of an intramedullary tibial nail with osteolysis in the middle tibia.
Immediately after the operation the calcium levels clearly slipped away, but the peri- and post-operative course was uncomplicated and the patient was able to be fully mobilised in a satisfactory manner. After two weeks of hospitalisation, the patient was discharged to home care in good general condition.
Discussion
According to the literature (Table I), OFC is a rare presentation of both primary and secondary hyperparathyroidism (2), and was first described by von Recklinghausen in 1891 (1). Due to the elevated parathyroid hormone, there is excessive activation of osteoclasts, which can lead to transformation and degradation processes in the bones (10). This forms a cystic change in the bone, which appears as a brown tumor and can cause an increased risk of fracture. In everyday clinical practice, the presence of hyperparathyroidism is in some cases diagnosed only after a pathological fracture has occurred. Histopathologically, the tumor can be assigned to the group of giant cell tumors (11). However, because of its rarity and the way it typically presents, metastatic cancer is often the first diagnostic impression (2).
Summary of the literature review illustrating characteristics of patients with brown tumor [reference values according to the National Library of Medicine (19)].
OFC is uncommon in clinical practice, and its clinical symptoms and imaging findings are easily confused with malignant bone tumors. However, brown tumors are difficult to diagnose, leading to delayed treatment (12). Histology cannot guarantee a certain diagnosis, as other lesions, such as giant cell tumor, giant cell granuloma, aneurysmal bone cyst, and some variants of osteosarcomas show similar macroscopical and microscopical features because all these conditions contain giant-cell lesions (2, 13, 14). Moreover, if hypercalcemia is present, the first impression is often that of malignancy itself (2). Even positron emission tomography (PET) scanning does not reliably distinguish between a skeletal malignancy and benign disease (15).
Multiple skeletal lesions (brown tumors) represent a rare clinical manifestation of prolonged hyperparathyroidism and are reported in approximately 2%-5% of patients with primary hyperparathyroidism (12, 16). We therefore performed a literature search on the characteristics of bone brown tumors caused by secondary to primary hyperparathyroidism. We gathered and searched for similar cases reported from 2016 to 2021. The primary database used for the search was PubMed. As suggested in previous studies, further publications were identified by cross-searching the article references. Thus, a backward and forward citation search was performed. PubMed was searched as follows: with the keywords (brown tumor) AND (primary hyperparathyroidism) AND (case report). Published articles during 2016-2021 were included. Meta-analyses and non-English-language articles were excluded. Finally, only articles where full text was available were included. The characteristics of all cases are shown in Table I.
Serum calcium, parathyroid hormone, and alkaline phosphatase were significantly elevated in most patients. Serum phosphorus was correspondingly reduced. In most cases, osteolytic lesions were classified as primary or metastatic tumors. The authors report that PHPT with osteitis fibrosa was hardly ever diagnosed in all of the cases and symptomatic hypercalcaemia was considered to be an accompanying symptom of the malignancy itself (17). In some cases, palliative cancer treatment was initiated and even amputation of the leg was considered (17). In another case, where a patient suffered from recurrent painful jaw swelling, an incision biopsy of the lesion suggested giant cell reparative granuloma and the patient underwent transoral curettage of the lesions (18). Only when the patient again sought clinical attention for recurrent jaw swelling further investigation was performed and blood biochemistry revealed abnormally high serum calcium, relatively low phosphate and grossly elevated parathyroid levels (18).
In accordance with most cases reported in the literature, the first diagnosis in the current case was bone metastasis and the patient was presented for haemato-oncological consultation. A sonographically targeted biopsy was performed and even after bone biopsy diagnosis was not clear. After a whole-body CT scan and a CT scan of the skull and neck, which revealed numerous osteolytic destructions with osteolytic defects, the differential diagnosis of multiple myeloma was established. Now, one might possibly ask how in the synopsis of the radiological and laboratory findings an “obvious” brown tumor could not be recognised. These misinterpretations of the radiological imaging and the resulting mistreatment may be explained by the rarity of these skeletal lesions.
Diagnosis of a brown tumor could especially be difficult, when there is a history of a malignant tumour disease in a patient’s medical record (9). Bone lesions could be erroneously interpreted as bone metastases. Even if a brown tumor is suspected, there could be great concern not to miss a concomitant malignant disease (9). This is aggravated by the fact that the first biopsy, like in the presented case, is sometimes not diagnostic for either malignancy or brown tumor. Therefore, biochemistry laboratory examinations might in some cases be more useful than biopsies and histopathology (9).
In conclusion, brown tumors are a rare clinical manifestation of prolonged hyperparathyroidism. As seen from the literature, they are often overseen and misinterpreted. In some cases, even palliative cancer treatment or amputation was initiated. Therefore, we conclude that in the case of hypercalcemia and lytic lesions, primary hyperparathyroidism should always be considered as a differential diagnosis. Further biochemical evaluation and bone scan can help in the management. We strongly suggest and absolutely encourage physicians to admit patients with an unclear osteolytic lesion and pathological fracture to a tertiary orthopaedic oncological center for further treatment and diagnostics.
Acknowledgements
Professional language editing of the manuscript by Mary Margreiter is acknowledged. Radiological images are used with kind permission of the local Department of Radiology.
Footnotes
This article is freely accessible online.
Authors’ Contributions
All of the Authors made relevant contributions to the conception of the study, to the acquisition, analysis or interpretation of data, and to the development of the final work. Each of the Authors has read and concurs with the content of the final manuscript.
Conflicts of Interest
The Authors declare that they did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The Authors declare that they have no conflicts of interest in relation to this study.
- Received April 8, 2021.
- Revision received April 22, 2021.
- Accepted April 23, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.





{kind=link}
{kind=link}
{kind=link}
{kind=link}