


Abstract
Background/Aim: Although surgical thoracoscopy is recommended in the diagnosis of malignant pleural mesothelioma (MPM), the invasiveness of this procedure is of strong concern. Our review aimed to evaluate the accuracies of medical thoracoscopy (MT), computed tomography (CT)-guided biopsy, and ultrasound (US)-guided biopsy in the diagnosis of MPM among patients with pleural effusion. Materials and Methods: We searched the MEDLINE, Embase, Central, and International Clinical Trials Registry Platform databases for studies evaluating the diagnostic accuracy of at least one of the biopsy procedures among patients with pleural effusion of unknown aetiology who had undergone thoracentesis and/or blind biopsy. A hierarchical summary receiver operating curve was created for MT. Results: Following full-text screening, 15 studies were included. MT studies had a high risk of bias and low applicability concern; however, hierarchical summary receiver operating curve revealed that MT had a high sensitivity. Conclusion: MT might be a useful rule-in test for guiding the use of more invasive diagnostic procedures.
- Malignant pleural mesothelioma
- pleural effusion
- medical thoracoscopy
- computed tomography-guided biopsy
- ultrasound-guided biopsy
- review
Malignant pleural mesothelioma (MPM) is a rare malignancy, although its global incidence has increased during the 21st century (1). Approximately 70% of MPM patients present with pleural effusion (2); however, diagnosing MPM is difficult and the definitive diagnosis should not be based on cytology alone, given its very low sensitivity (3). Thus, in cases of suspected MPM, pleural biopsy is recommended to collect large samples from the area of concern (4-6). There are six techniques for pleural biopsy: i) open biopsy, ii) surgical thoracoscopy, iii) medical thoracoscopy (MT), iv) computed tomography (CT)-guided biopsy, v) ultrasound (US)-guided biopsy, and vi) blind biopsy. Although various national guidelines prefer surgical thoracoscopic biopsy, this procedure is highly invasive and must be performed under general anaesthesia (4-6). To this end, it would be useful to have a sensitive and less invasive rule-in test that could guide the use of more invasive diagnostic procedures.
Metintus et al., have performed head-to-head comparisons between CT-guided biopsy, MT, and US-guided biopsy for evaluating the cause of pleural effusion, and have recommended CT-guided biopsy based on its less invasive nature and high diagnostic accuracy (7, 8). Unfortunately, the sample size of these studies are small and non-significant results from other superiority trials were not optimal for selecting the most appropriate alternative to surgical thoracoscopy (9). Furthermore, the small proportion of MPM cases (27%) indicates that the results regarding diagnostic accuracy are not specific to MPM (7, 8). For these reasons, this systematic review aimed to evaluate the diagnostic accuracy of three different biopsy procedures: i) MT, ii) CT-guided biopsy, and iii) US-guided biopsy, in an attempt to identify the ideal rule-in procedure to guide the use of subsequent surgical thoracoscopy in cases with suspected MPM.
Materials and Methods
Study registration. This systematic review was pre-registered in the International Prospective Register of Systematic Reviews (CRD42020 163686). Although, we had initially planned a network meta-analysis of diagnostic test accuracy, the protocol was simplified to a systematic review of each procedure, given the small number of head-to-head studies. The systematic review was based on the Preferred Reporting Items for Systematic Review and Meta-Analyses guidelines (10). The details of the study protocol are uploaded elsewhere (https://github.com/AkihiroShiroshita/Malignant-mesothelioma-Supplement).
Study design. We performed a comprehensive search of the MEDLINE, Embase, Central, and International Clinical Trials Registry Platform databases for studies published until January 30, 2020. There were no restrictions regarding the language or earliest publication year. The search strategy included the terms related to the index tests: i) MT, ii) CT-guided biopsy, and iii) US-guided biopsy, and iv) the target condition (MPM). Potentially relevant articles were also selected via the Web of Science and reference lists of the identified reports. Title and abstract screening were performed independently by AS and MK. The inclusion criteria were: i) prospective and ii) retrospective observational studies, iii) case-control studies, and iv) case series that evaluated the diagnostic accuracies of the three biopsy procedures for detecting MPM among patients with pleural effusion of unknown aetiology, who had undergone thoracentesis and/or blind biopsy. Although fluid accumulation is not required for CT- and US-guided biopsies, it is usually required for MT (9). Thus, we restricted the analyses to patients with pleural effusion to ensure that diagnostic accuracies were evaluated in comparable patient populations. The reference standard was the final diagnosis based on follow-up and/or additional biopsies, including surgical thoracoscopy or other procedures. The exclusion criteria were as follows: i) case reports, reviews, and other studies that used animal models, ii) studies that only included biopsies that did not involve the pleura, iii) studies that did not assess the MPM-specific diagnostic accuracy, and iv) studies that only evaluated the diagnostic yield and did not require further assessment for undiagnosed patients.
Data extraction and statistical analysis. Following title and abstract screening, full-text screening was independently performed by AS and MK to identify eligible studies. Data were extracted from the eligible studies regarding i) patient demographic characteristics, ii) study protocol, and iii) the numbers of true positive, false positive, false negative, and true negative results. AS and MK assessed the methodological quality of the included articles using the Quality Assessment of Diagnostic Accuracy Studies-2 tool (11). A forest plot was created for each biopsy procedure and a hierarchical summary receiver operating characteristic curve was generated for medical thoracoscopy. Since the number of false positive cases was zero, we added one to each false positive number to calculate the bivariate model parameters. Finally, we summarized our systematic review in Table I (12).
Summary of the findings. Sensitivity and specificity values were reported as the point estimates and 95% confidence intervals.
All statistical analyses were performed by AS using the STATA 15 software (STATA Corp. College Station, TX, USA) and RevMan v5.4.1 software (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). The results were double-checked by KY. During the whole review process, any disagreements between AS and MK were resolved via discussion or consultation with YK.
Results
Our search identified 3,206 studies, and a thorough review of the reference lists identified 49 additional studies. Following the removal of duplicates, the titles and abstracts were screened for 2,523 studies, and 133 studies were selected for full-text screening. Of these, 15 studies were ultimately included in the systematic review, with 13 studies regarding MT (7, 13-24), 2 studies regarding CT-guided biopsy (7, 25), and 1 study regarding US-guided biopsy (26). Figure 1 illustrates the study selection process. Reasons of exclusion are summarized in the supplementary file (https://github.com/AkihiroShiroshita/Malignant-mesothelioma-Supplement).
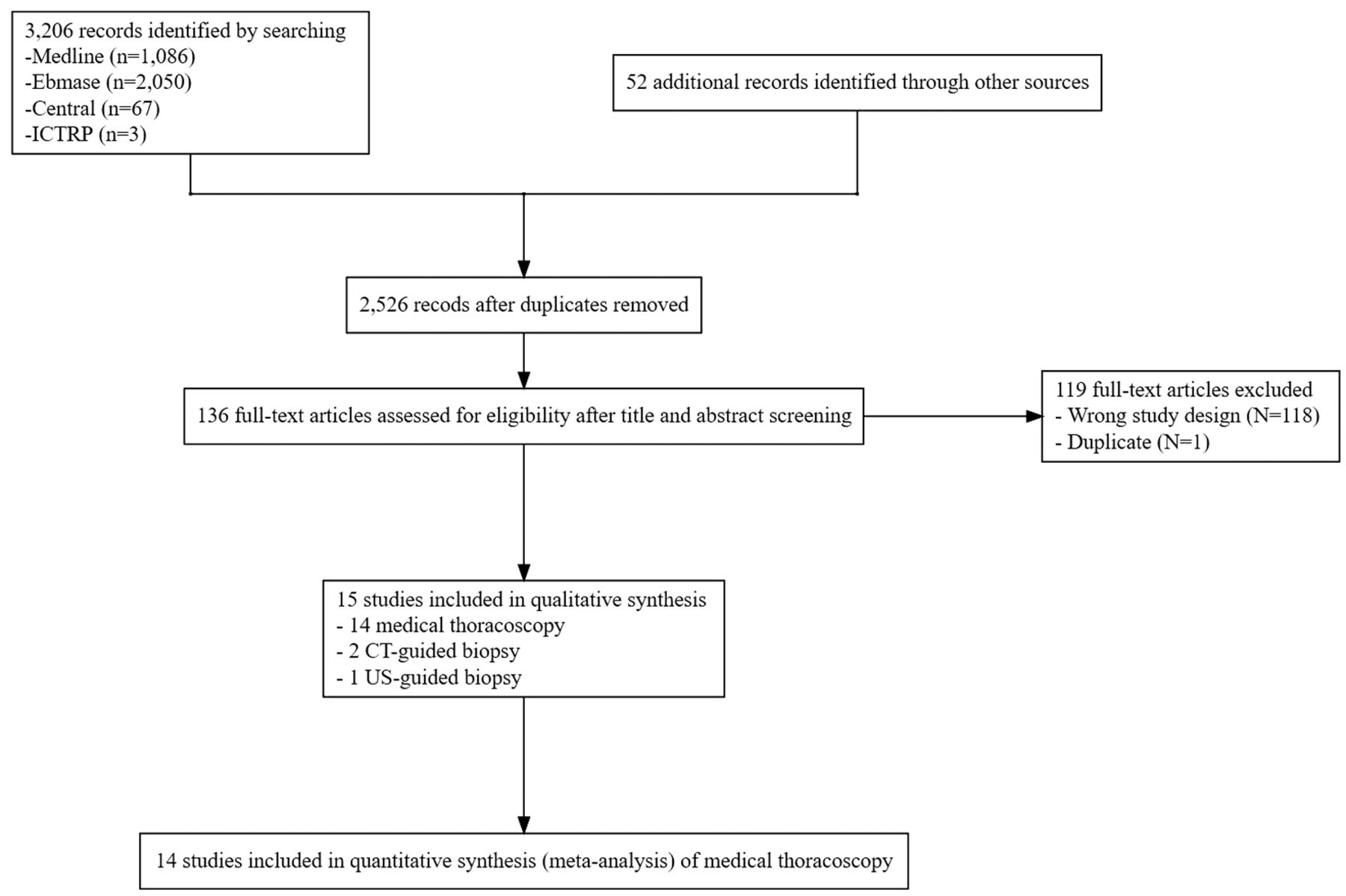
Study selection flow chart. The flow chart shows the inclusion and exclusion criteria and is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. ICTRP: International Clinical Trials Registry Platform; CT: computed tomography, US: ultrasound.
The characteristics of the studies are summarized in Table II, while Table III shows the detailed information regarding the index tests and reference standards. All the included studies were conducted at a single center and targeted patients with pleural effusion of unknown aetiology who underwent at least thoracentesis or blind biopsy, regardless of pleural nodularity or asbestos exposure. The report by Lee et al., is a meeting abstract and only Metintas et al., have performed a head-to-head comparison of the different modalities (7, 26). In addition, only Maskell et al., have followed up the patients after the index test (CT-guided biopsy) to reach a final diagnosis (25). The modified Quality Assessment of Diagnostic Accuracy Studies-2 tool revealed a high risk of bias regarding the index test and reference standard for the studies involving medical thoracoscopy and CT-guided biopsy due to unblinded histological evaluation of the biopsy samples and non-predefined pathological criteria for diagnosing MPM. The risk of bias is unclear for the study regarding the US-guided biopsy by Lee et al., (26) as we were unable to collect the relevant data about the various domains. The detailed information about the quality assessment is summarized in the supplementary file (https://github.com/AkihiroShiroshita/Malignant-mesothelioma-Supplement).
Study characteristics.
Index tests and reference standard.
The forest plot for MT revealed a low amount of heterogeneity in the sensitivity findings and all reports revealed 100% specificity (Figure 2). Given that most included studies focused on MT, we constructed a hierarchical summary receiver operating characteristic curve, which revealed a high sensitivity of this particular procedure (Figure 3). CT- and US-guided biopsies had insufficient information to evaluate. Table III summarizes the findings of our systematic review.

Forest plots of sensitivity and specificity in each study. Studies about medical thoracoscopy presented a high sensitivity for the diagnosis of malignant pleural mesothelioma. Although the number of studies about computed tomography-guided biopsy and ultrasound-guided biopsy was small, they reported low sensitivity. TP: True positive; FP: false positive; FN: false negative; TN: true negative; CI: confidence interval.

Hierarchical summary of the receiver operating characteristics curve for medical thoracoscopy. Studies using medical thoracoscopy report a high sensitivity for detecting malignant pleural mesothelioma.
Discussion
This systematic review revealed that MT has a high sensitivity for detecting MPM among patients with pleural effusion of unknown aetiology. However, the small number of included studies made it difficult to precisely evaluate the diagnostic accuracies of CT- and US-guided biopsies. Additionally, there are concerns regarding a high risk of bias due to unblinded histological evaluations and a lack of predefined pathological diagnostic criteria.
Our results indicate that MT could be a useful rule-in test for guiding the use of surgical thoracoscopy among patients with suspected MPM with pleural effusion of unclear aetiology. Most of the included studies indicate that MT provides >90% sensitivity, which is comparable to the reported sensitivity of surgical biopsy (Point Estimate=94%, 95% Confidence Interval=73-100 %) (7). A previous systematic review has also indicated that MT provides high sensitivity for determining the aetiology of exudative pleural effusion (27); however, lung and breast cancers are the major causes of malignant pleural effusion (28, 29). Thus, the diagnosis of MPM remains challenging and should be based on an adequate tissue specimen (30). In this context, medical thoracoscopy allows direct visualization and biopsy of the pleura under local anaesthesia, which could explain its high sensitivity.
Even though we were unable to clarify the diagnostic accuracies of CT- or US-guided biopsies, these tend to be selected for patients with little or no pleural effusion, as they reduce the risk of organ damage related to trocar insertion (9). Furthermore, sedation is not required for any of these procedures, and they are considered more accessible compared to MT. Nevertheless, these techniques might have a low sensitivity for detecting MPM among patients with pleural effusion. Further head-to-head trials are needed to address this issue, as we were unable to perform a network meta-analysis to compare the diagnostic accuracies.
Our findings should be interpreted with caution considering the high risk of bias due to the index tests and reference standards. Pathological diagnosis of MPM is complicated due to the lack of a single specific diagnostic marker (31). The diagnosis should be based on immunohistochemistry rather than electron microscopy and gross pathological findings (30). Physicians usually start treatment for MPM based on a single pathological result and rarely perform a second biopsy. This might lead to overestimation or underestimation of the diagnostic accuracy, depending on the interpretation of the pathological findings. Although MT may be less efficient for defining the histological subtype of MPM, only one study by Maskell et al. has followed up the diagnosed patients based on the index test (25, 32). Thus, it is important to consider the process of diagnosing MPM based on the biopsy sample, while future studies should use a predefined diagnostic process to help address this issue.
This systematic review has several limitations. First, unidentified but relevant studies might exist, as we used search terms related to the three biopsy procedures and MPM, which would miss studies that did not include MPM in the title and abstract. For example, we might have likely missed studies in which patients with pleural effusion underwent pleural biopsy but were not diagnosed with MPM. We aimed to minimize this issue by performing a manual search of the reference lists, although this cannot not guarantee the inclusion of all the otherwise missed studies. Second, we could not differentiate between the efficiency of the three procedures depending on the MPM subtype (e.g., the epithelioid, biphasic, and sarcomatoid subtypes), which is important for guiding treatment selection. Third, we did not consider pleural nodularity and instead focused on patients with pleural effusion. The diagnostic accuracy can be influenced by the target region (8). Fourth, we did not consider the presence of risk factors for MPM, including asbestos exposure, and it is important to note that all patients were only suspected of malignant pleural effusion at their presentation.
In conclusion, our study demonstrated that MT might be a useful rule-in test for guiding the subsequent use of thoracoscopic surgery in cases of suspected MPM. Unfortunately, given the small number of included studies, we were unable to precisely evaluate the diagnostic accuracies of CT- and US-guided biopsies. Further trials are needed to perform head-to-head comparisons of the different biopsy procedures.
Acknowledgements
Funding for English-language editing was obtained from the Systematic Review Workshop Peer Support Group (SRWS-PSG: https://community.camp-fire.jp/projects/view/187310). The funder played no role in the study design, study execution, data analyses, data interpretation, or decision to submit the results.
Footnotes
This article is freely accessible online.
Conflicts of Interest
The Authors have no relevant financial or non-financial interests to disclose.
Authors’ Contributions
AS, MK, MT, and YK contributed to the conception and design of the work. AS and MK contributed to the acquisition of data. AS and YK wrote a draft, and all authors revised it, then approved the final version of the manuscript. AS, MK, MT, and YK agreed to be accountable for all aspects of any part of the work.
- Received February 11, 2021.
- Revision received March 21, 2021.
- Accepted March 29, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.