


Abstract
Background/Aim: To retrospectively evaluate the efficacy and safety of modified TPEx (docetaxel 60 mg/m2 on day 1, cisplatin 60 mg/m2 on day 1, and weekly cetuximab 250 mg/m2 with loading dose of 400 mg/m2) followed by maintenance cetuximab as first-line treatment for inoperable recurrent and/or metastatic squamous cell carcinoma of the head and neck. Patients and Methods: We analyzed 22 Japanese patients receiving modified TPEx every 21 days for four cycles with or without prophylactic granulocyte colony-stimulating factor (G-CSF). Results: The best overall response rate was 55% [95% confidence interval (CI)=35-73]. The median progression-free survival and overall survival were 8.9 months (95%CI=3.9-10.2) and 14.3 months (95%CI=10.1-28.2), respectively. Without prophylactic G-CSF, Grade 3/4 neutropenia and febrile neutropenia was common (94% versus 20%; p=0.003 and 41% versus 0%; p=0.11, respectively). Conclusion: The modified TPEx is effective, while prophylactic G-CSF is essential.
- Drug therapy
- cisplatin
- docetaxel
- cetuximab
- granulocyte colony-stimulating factor
- squamous cell carcinoma of the head and neck
A phase III trial established six cycles of cisplatin and 5-fluorouracil (5-FU) in combination with cetuximab (EXTREME regimen: cisplatin 100 mg/m2 on day 1, 5-FU 1000 mg/m2/day on days 1-4, and weekly cetuximab 250 mg/m2 with loading dose of 400 mg/m2) followed by maintenance weekly cetuximab 250 mg/m2 as the standard of first-line treatment for patients with inoperable recurrent and/or metastatic squamous cell carcinoma of the head and neck (HNSCC), although the survival still remains unsatisfactory (1). The GORTEC phase II study evaluated the efficacy and safety of four cycles of docetaxel and cisplatin in combination with cetuximab (TPEx regimen: docetaxel 75 mg/m2 on day 1, cisplatin 75 mg/m2 on day 1, and weekly cetuximab 250 mg/m2 with loading dose of 400 mg/m2) followed by maintenance bi-weekly cetuximab 500 mg/m2 (2). The best overall response rate was 52%; the median progression-free survival (PFS) and median overall survival (OS) were 6.2 and 14.0 months, respectively. Under prophylactic use of granulocyte colony-stimulating factor (G-CSF), grade 3/4 neutropenia was observed in 20% of the patients, and 7% of the patients developed grade 3 febrile neutropenia (FN). Given these promising results, the phase III trial, termed as TPExtreme, was conducted to compare the efficacy between EXTREME and TPEx regimens (3). Median OS was 13.4 months for the EXTREME arm and 14.5 months for the TPEx arm, while time on chemotherapy was shorter and toxicity was lower in the TPEx arm than in the EXTREME arm, suggesting TPEx regimen as a new option in first-line treatment of recurrent/metastatic HNSCC. Of note, lower toxicity of TPEx regimen was most probably secured by prophylactic use of G-CSF. In other words, TPEx regimen would have been highly toxic without prophylactic use of G-CSF. In Japan, it was not until pegfilgrastim was released at the end of 2014 that prophylactic G-CSF was approved for patients with HNSCC receiving systemic chemotherapy. Moreover, weekly cetuximab 250 mg/m2 is approved in Japan, but bi-weekly cetuximab 500 mg/m2 is not. Accordingly, we modified the original TPEx regimen so that the dose of the cytotoxic drugs was reduced by 20%, such as docetaxel 60 mg/m2 and cisplatin 60 mg/m2, with the dose of cetuximab being unchanged. Maintenance cetuximab was also modified from bi-weekly 500 mg/m2 to weekly 250 mg/m2. We started using this modified TPEx regimen as first-line treatment for Japanese patients with recurrent/metastatic HNSCC without prophylactic G-CSF in 2014, while prophylactic G-CSF was added in 2016. Here, we retrospectively evaluated the efficacy and safety of modified TPEx with respect to prophylactic G-CSF.
Patients and Methods
Patients. Patients with recurrent/metastatic HNSCC who received modified TPEx as first-line treatment at Osaka University Hospital and Osaka Rosai Hospital between 2014 and 2017 were eligible. To receive modified TPEx, patients were required to be >20 years of age, with an Eastern Cooperative Oncology Group performance status of 0-1, to have adequate bone marrow, liver and renal function, and to have pathologically proven non-nasopharyngeal HNSCC with a recurrence and/or metastasis not relevant for locoregional treatment. The tumor had to be measurable by computed tomography (CT) or magnetic resonance imaging (MRI) according to the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1 (4). Exclusion criteria included prior chemotherapy for HNSCC (except if administered as part of multimodal treatment for locally advanced disease more than 3 months prior), previous treatment with antibody therapy, including cetuximab, a past history of surgery (excluding diagnostic biopsy) or radiotherapy for the index cancer less than 4 weeks prior, a past history of secondary primary cancer diagnosis (excluding superficial disease) less than 2 years prior, or another active cancer. We also excluded patients who received nivolumab, an immune checkpoint inhibitor, as second-line treatment. Nivolumab, which confers survival benefit on patients with platinum-refractory recurrent/metastatic HNSCC (5), was approved in Japan in 2017 to treat such patients. We sought to assess the clinical outcome of modified TPEx in the absence of the effect of nivolumab, which might allow us to make indirect comparison of efficacy between modified TPEx and original TPEx (3). Human papilloma virus (HPV) status of oropharyngeal cancer was determined by p16 immunohistochemistry and PCR followed by direct sequencing, as reported previously (6). Both p16-positive and HPV DNA-positive tumor was defined as HPV-related. The Institutional Review Board approved the protocol of the present study, and waived the requirement of an informed consent of patients due to the retrospective nature of the study.
Treatment. Modified TPEx regimen consisted of four cycles of docetaxel and cisplatin both at 60 mg/m2 on day 1, and cetuximab on days 1, 8, and 15 (400 mg/m2 on day 1 of the first cycle and 250 mg/m2 weekly thereafter), repeated every 21 days. The dose of the cytotoxic agents and/or cetuximab was reduced as necessary, while a switch from cisplatin to carboplatin was not considered. Prophylactic administration of G-CSF was not made until after 2015. Patients with complete response (CR), partial response (PR), or stable disease (SD) after modified TPEx were encouraged to continue weekly cetuximab 250 mg/m2 as maintenance therapy until progressive disease (PD) or unacceptable toxicity.
Statistical analysis. Tumor response was assessed by CT and/or MRI after every 2 cycles of modified TPEx and/or after the discontinuation of modified TPEx, and thereafter every 2 months until PD. The best overall response was defined as CR or PR persisting for at least 6 weeks from the start of treatment. Overall survival (OS), progression-free survival (PFS), and the response rate after the completion/discontinuation of four cycles of modified TPEx were also evaluated. Tumor response was assessed according to the RECIST, version 1.1 (4). All events were measured from date of treatment start to date of their occurrence. The OS and PFS rates were estimated using the Kaplan–Meier method. Toxicity was assessed weekly according to Common Terminology Criteria for Adverse Events (CTCAE) version 4.0. The JMP® Pro version 14.0.0. system (SAS Institute, Inc., Cary, NC, USA) was used for all statistical analyses.
Results
Patient characteristics. We identified 22 patients who met the criteria. Baseline characteristics of the patients are shown in Table I. Five (23%) patients received prophylactic G-CSF, while 17 (77%) patients did not. Three of the six oropharyngeal cancers were HPV-related. Seventeen (77%) patients had previously received chemotherapy in a variety of settings; 4 received super-selective intra-arterial cisplatin infusion chemoradiotherapy (RADPLAT), 7 received concurrent chemoradiotherapy (CCRT), and 6 received adjuvant chemotherapy. The RADPLAT regimen consisted of rapid, targeted super-selective intra-arterial infusions of cisplatin, 100 mg/m2 every week for 4 weeks, with concurrent 70 Gy of radiotherapy (2 Gy/fraction) (7). Cisplatin was neutralized immediately after intra-arterial administration with a simultaneous intravenous infusion of sodium thiosulfate. The CCRT regimen consisted of six cycles of 10 mg/m2 docetaxel and 20 mg/m2 cisplatin concurrent with 66 Gy of radiotherapy (2 Gy/fraction) (8). Adjuvant chemotherapy consisted of two cycles of modified TPF (docetaxel and cisplatin both at 60 mg/m2 on day 1, and 5-FU 600 mg/m2/day on days 1-5). Median cumulative doses of the cytotoxic agents in previous treatments were 120 mg/m2 (range=0-520 mg/m2) for cisplatin, 60 mg/m2 (range=0-170 mg/m2) for docetaxel, and 0 mg/m2 (range=0-6,000 mg/m2) for 5-FU. In patients receiving intravenous administration of cisplatin in previous treatments, the median cumulative dose of cisplatin was 120 mg/m2 (range=0-220 mg/m2). In patients receiving cisplatin in previous treatments, the median interval between the final infusion of cisplatin as prior therapy and the start of modified TPEx was 13.4 months (range=3.0-37.0 months). Three patients started modified TPEx less than 6 months after the final infusion of cisplatin as prior therapy.
Patient characteristics.
Treatment and adherence. During the modified TPEx phase, a total of 72 cycles were administered (median 4 cycles; mean 3.3±1.0 cycles/patient; Table II). The median duration of the modified TPEx phase was 95 days (range=7-132 days). A dose reduction of cisplatin and docetaxel was required for four patients. One patient needed a dose reduction of cetuximab. The median cumulative doses of the cytotoxic agents and cetuximab were 195 mg/m2 (range=60-240 mg/m2) and 3,150 mg/m2 (range=400-3,150 mg/m2), respectively. The relative dose intensities (RDI) of cisplatin, docetaxel and cetuximab were 80.0±14.3% (mean±SD), 80.6±13.0%, and 82.5±12.3% respectively. The RDI of the modified TPEx regimen was ≥80.0% in eleven (50%) patients.
No. of cycles and relative dose intensity of modified TPEx (N=22) and cetuximab maintenance (N=8).
Fourteen (64%) patients completed four cycles of modified TPEx. Due to PD, five and one patients discontinued modified TPEx after two and three cycles, respectively. One patient refused to continue in the middle of the first cycle, soon after the initial administrated dose of cetuximab. One patient discontinued after two cycles because of an adverse event; infectious endocarditis followed by brain infarction. Of 14 patients completing four cycles, 8 (57%) patients were able to start maintenance cetuximab therapy. Four patients were unable to start maintenance cetuximab; two due to PD, one due to death of aspiration pneumoniae shortly after the completion of modified TPEx, and one due to grade 3 skin reaction. The remaining two patients had CR at distant site and thereafter received radiotherapy for locoregional residual disease instead of maintenance cetuximab. During the maintenance phase, the median dose of cetuximab was 12 (range=3-44). Ten (45%) patients received second-line treatment: six patients received paclitaxel and cetuximab, two patients received S-1 chemotherapy and two patients received radiotherapy. No patient was lost to follow-up.
Tumor response. An objective response, after the completion or discontinuation of the modified TPEx, was not evaluated in one patient who discontinued in the middle of the first cycle. Two patients with lung metastasis achieved CR, while ten patients showed PR, indicating that the response rate was 57% (95%CI=37-76; Table III). For the best overall response, two and 10 patients showed CR and PR, respectively, indicating that the best overall response rate was 55% (95%CI=35-73). Four patients had SD, indicating that a total of 73% of patients had some form of disease control. Of note, all of six patients who completed four cycles of modified TPEx and subsequently started maintenance cetuximab showed CR or PR as the best overall response.
Response after modified TPEx (N=21) and best overall response during modified TPEx and maintenance (N=22).
Toxicity. Grade 3/4 hematologic and non-hematologic adverse events with respect to prophylactic G-CSF are shown in Table IV. No patient died due to adverse events from modified TPEx or maintenance cetuximab. The most common grade 3/4 hematological event was lymphopenia, which all patients experienced. Incidence of grade 3/4 leukopenia and neutropenia was significantly higher in patients not receiving prophylactic G-CSF than in patients receiving prophylactic G-CSF (94% versus 20%, p=0.003; 94% versus 20%, p=0.003, respectively). There was a trend that grade 3/4 FN was more prevalent in patients not receiving prophylactic G-CSF (41% versus 0%, p=0.11). One patient who had grade 3 FN developed infective endocarditis leading to multiple brain infarctions with neurological disorders (grade 4 infection). The most common grade 3 non-hematologic event was rash acneiform observed in five (23%) patients. No patient experienced a grade 3/4 infusion reaction.
Grade 3/4 adverse events during modified TPEx according to prophylactic G-CSF.
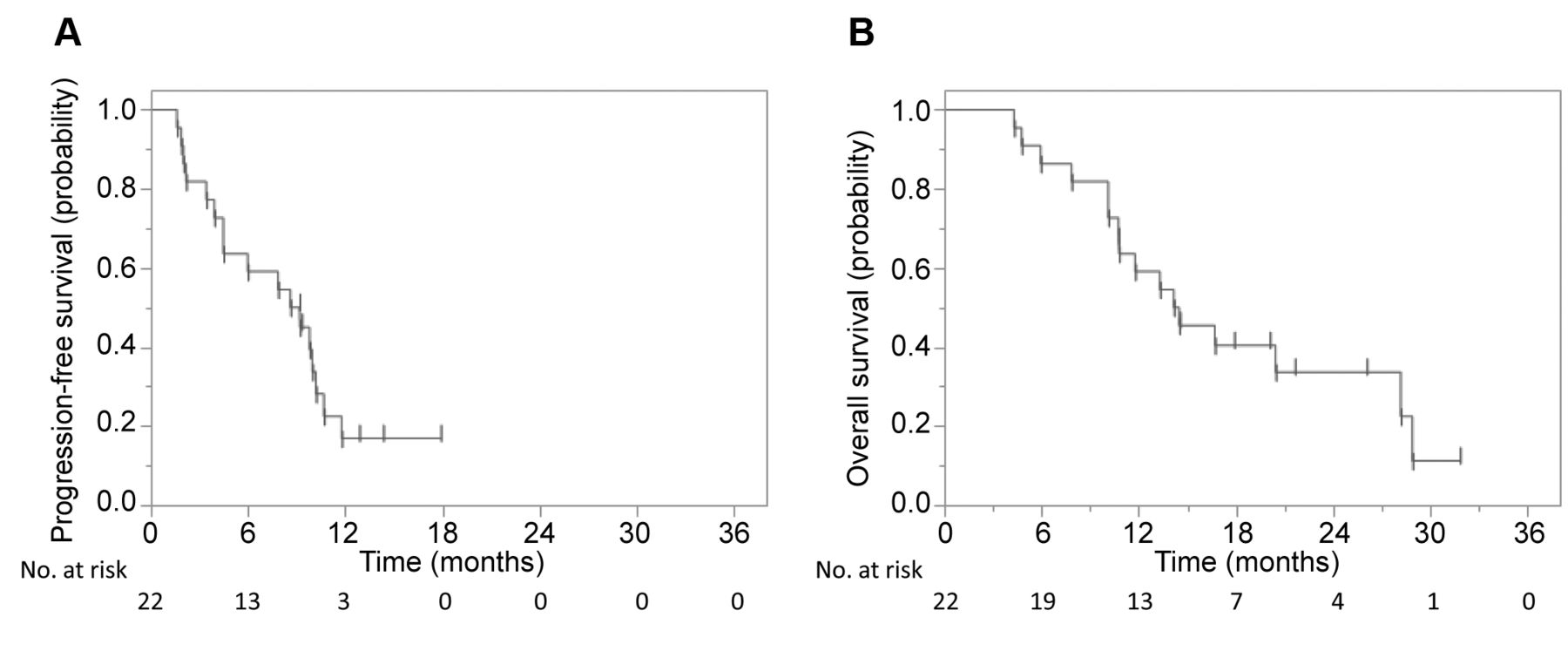
Survival. At the time of analysis, there were sixteen deaths, while four (18%) and two (9.1%) patients were alive with and without disease, respectively. Fifteen deaths were index cancer-related, and one death was caused by FN during second-line treatment. The median follow-up of surviving patients was 21.0 months (range=14.5-31.8 months). Median OS and PFS were 14.3 months (95%CI=10.1-28.2) and 8.9 months (95%CI=3.9-10.2), respectively. The estimated 1-year OS rate was 59.1% (38.2-77.2), while the estimated 1-year PFS rate was 16.9% (5.7-40.6) (Figure 1). There was no difference in median PFS (8.6 months; 95%CI=3.9-10.0) versus 10.2 months (95%CI=1.6-not reached, p=0.35) and median OS (14.2 months; 95%CI=10.1-28.2) versus 20.4 months (95%CI=4.7-20.4; p=0.90) between patients not receiving prophylactic G-CSF and patients receiving it.

Kaplan–Meier estimates of progression-free survival (A) and overall survival (B). Median progression-free survival (PFS) and overall survival (OS) were 8.9 months (95%CI=3.9-10.2) and 14.3 months (95%CI=10.1-28.2), respectively, while the 1-year rates of PFS and OS were 16.9% (95%CI=5.7-40.6) and 59.1% (95%CI=38.2-77.2), respectively.
Discussion
In the present study, we evaluated the efficacy of modified TPEx regimen as first-line treatment for patients with recurrent/metastatic HNSCC, and found that median OS was 14.3 months. Given that median OS for original TPEx regimen was 14.0-14.5 months (2, 3), the modified TPEx regimen seems comparable with the original TPEx regimen in efficacy, although it is difficult to draw a firm conclusion from comparison across studies.
Grade 3/4 neutropenia was observed in 94% of the patients not receiving prophylactic G-CSF and in 20% of the patients receiving it. Forty-one % of the patients not receiving prophylactic G-CSF developed grade 3 FN, while no patient receiving it did. These results strongly indicate that prophylactic G-CSF is essential when treating patients with modified TPEx regimen. Some might argue that prophylactic G-CSF would make original TPEx regimen feasible in the treatment of Japanese patients with recurrent/metastatic HNSCC. We favor modified TPEx rather than original TPEx because the incidence of grade 3/4 neutropenia was equivalent under prophylactic G-CSF support between Japanese patients receiving modified TPEx (20%) and European patients receiving original TPEx (20%) (2). It is likely that the incidence of severe hematological adverse events will be increased in Japanese patients receiving original TPEx even with prophylactic G-CSF. Moreover, the reduction of the accumulating dose of cisplatin would decrease cisplatin-related toxicities, such as hearing impairment.
Of interest is the efficacy of the EXTREME regimen as first-line treatment for Asian patients with recurrent/metastatic HNSCC. When Japanese patients were treated with the original EXTREME regimen, median OS was 14.1 months (9). On the other hand, when Chinese and Korean patients were treated with modified the EXTREME regimen in which the dose of the cytotoxic agents was reduced by 25% with the dose of cetuximab being unchanged (cisplatin 75 mg/m2 on day 1, 5-FU 750 mg/m2/day on days 1-5, and weekly cetuximab 250 mg/m2 with loading dose of 400 mg/m2), median OS was 12.6 months (10). These results suggest that the dose reduction of the cytotoxic agents did not affect the efficacy of the EXTREME regimen. Given that original TPEx regimen yielded equivalent survival with a shorter time on chemotherapy and significantly lower toxicity compared with the original EXTREME regimen (3), it is of interest to make a head-to-head comparison between modified PFE and modified TPEx regimens as a first-line treatment for Asian patients with recurrent/metastatic HNSCC. We are currently performing a clinical trial to address this issue (UMIN000025436) and the enrollment of patients has already been completed. Clinical outcomes that will be disclosed in near future are crucial because the participants commonly receive nivolumab as second-line treatment. KEYNOTE-048 showed significant survival advantage of pembrolizumab plus platinum and 5-FU over the EXTREME regimen (median OS 13.0 months versus 10.7 months) (11). However, patients in the EXTREME arm who received immunotherapy as second-line treatment were very limited, implying that the sequential efficacy of cetuximab with chemotherapy followed by immunotherapy remains unknown. Of note, survival according to second-line treatment in the TPExtreme randomized trial was very recently reported. Median OS in subgroups receiving immunotherapy as second-line was 19.4 months in the EXTREME arm and 21.9 months in the TPEx arm (12), suggesting that the replacement of 5-FU with docetaxel worked in favor of survival in the setting of sequential treatment. Sequential treatment of modified TPEx as first-line followed by nivolumab as second-line might be an attractive treatment option for patients with recurrent/metastatic HNSCC. The results of UMIN000025436 are awaited.
In conclusion, the modified TPEx regimen showed promising effectiveness as first-line treatment of patients with recurrent/metastatic HNSCC, while severe hematological toxicity was common without prophylactic G-CSF. Further studies are warranted.
Footnotes
Authors’ Contributions
Motoyuki Suzuki: Formal analysis, Visualization. Yukinori Takenaka, Toshihiro Kishikawa, Yoshifumi Yamamoto, Atsushi Hanamoto, Yoichiro Tomiyama, Takahito Fukusumi, Takahiro Michiba, Norihiko Takemoto, Susumu Nakahara: Investigation, Resources. Hidenori Inohara: Conceptualization, Methodology, Writing – Original draft.
This article is freely accessible online.
Conflicts of Interest
The Authors have no conflicts of interest to declare in relation to this study.
- Received January 22, 2021.
- Revision received February 23, 2021.
- Accepted February 24, 2021.
This is an open access article distributed under the CC BY license (https://creativecommons.org/licenses/by/4.0/).
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.