


Abstract
Background/Aim: This comparative plan study examines a range of boost-radiation methods in adjuvant radiotherapy of breast cancer using helical intensity-modulated radiotherapy with TomoEdge-technique. Impact of hypofractionated radiation with simultaneous-integrated boost (SIB) and influence of differing assumed α/β-values were examined. Patients and Methods: For 10 patients with left-sided breast cancer each four helical IMRT-plans with TomoEdge-technique were created: hypofractionated+SIB (H-SIB) (42.4/54.4 Gy, 16 fractions), normofractionated+SIB (N-SIB) (50.4/64.4 Gy, 28 fractions), hypofractionated+sequential-boost (H-SB) (42.4 Gy/16 fractions+16 Gy/8 fractions), normofractionated+ sequential-boost (N-SB) (50.4 Gy/28 fractions+16 Gy/8 fractions). Equivalent doses (EQD2) to organs-at-risk (OAR) and irradiated mammary-gland were analysed for different assumed α/β-values. Results: The mean EQD2 to OAR was significantly lower using hypofractionated radiation-techniques. H-SIB and H-SB were not significantly different. H-SIB and N-SIB conformed significantly better to the breast planning-target volume (PTV) and boost-volume (BV) than H-SB and N-SB. Regarding BV, mean EQD2 was significantly higher for all α/β-values investigated when using H-SIB and N-SIB. Regarding PTV, there were no clinically relevant differences. Conclusion: Relating to dosimetry, H-SIB is effective compared to standard-boost-techniques.
- Hypofractionated radiotherapy
- simultaneous integrated boost
- SIB
- breast cancer
- helical tomotherapy
- TomoEdge
- IMRT
Globally, breast cancer is the most common form of cancer in women (1). Surgery and adjuvant radiation therapy are the central pillars of curative therapy when treating localised breast cancer. Screening programs enable tumours to be discovered earlier, meaning that breast-conserving surgery alongside adjuvant radiotherapy achieves high cure rates. Additional radiotherapy significantly increases local control and prolongs overall survival (2, 3). As part of adjuvant radiation therapy, a radiation boost to the tumour bed results in significantly improved local control rates in the case of risk factor constellations, such as T2 tumours, positive lymph nodes, premenopausal patients, poorly differentiated G3 tumours, human-epidermal-growth-factor-receptor2 (HER2/neu) positivity, and narrow resection margins (4, 5). The radiation boost can be applied in several ways: teletherapy using photons or electrons, intra-operative radiotherapy, or interstitial brachytherapy (6-9). Thus far, the radiation boost is generally delivered sequentially, i.e., once whole breast radiation therapy is complete. Simultaneous integrated boost (SIB) radiation therapy is a recent approach to delivering radiation boosts (6). SIB can be administered using different percutaneous photon therapy radiation techniques, including 3D conformal radiation therapy (3D-CRT) and intensity-modulated radiation therapy (IMRT). Step-and-shoot IMRT and rotational IMRT, also known as volumetric arc therapy (VMAT), are commonly reported in the literature (6, 10, 11). The advantages of SIB in comparison to sequential boost (SB) include the reduced total treatment period and the steep dose drop-off between the edge of the planning target volume (PTV) and the remaining breast tissue, which is treated with a lower dose. Thus far, disadvantages include the relatively poor dose homogeneity when using 3D-CRT or IMRT (12). There have also been concerns about the potentially inferior cosmetic results in the long term since SIB supplies higher single doses to the PTV for the boost relative to the PTV for the whole breast (13).
Apart from the issue of radiation boosts, new discoveries relating to fractionation, total dose, and treatment length will bring about significant changes to the real-world practice of whole-breast irradiation. In normofractionated breast irradiation, the conventional practice is to administer 25 or 28 daily fractions of 2 Gy or 1.8 Gy, resulting in a total treatment dose of 50 Gy or 50.4 Gy (12). Large prospective phase III studies have shown that moderate hypofractionation using fractions of 2.5-2.65 Gy and a total dose (TD) of 40-42.4 Gy produces equivalent local control and overall survival results to those with normofractionation. Furthermore, hypofractionation significantly reduced treatment time (14-16 fractions) and showed a tendency towards improved cosmetic results. These studies used 3D conformal radiation techniques (14, 15).
However, these studies did not apply a radiation boost to the tumour bed in addition to hypofractionated whole breast radiation. Real-world clinical application is based on current indications for a radiation boost following hypofractionated whole breast radiation: sequential normofractionated boost (SB) at 2 Gy per fraction up to a TD of 10-16 Gy. This can be applied using a 3D conformal or IMRT technique (12).
Similar to using SIB alongside normofractionated whole breast radiation, there is discussion around the option to use simultaneous integrated boost alongside hypofractionated whole breast radiation with further increased single doses in the boost PTV (H-SIB). The additional radiation boost in this case would not increase the total treatment period. Concerns about increased fraction doses are related to the potential increase in the risk of late-onset side effects. New data on hypofractionated radiotherapy for whole breast radiation without boost radiation have shown no increase in side effect rates (16-19).
The linear quadratic model can be used to compare radiation exposure in each treatment scheme (20). This shows the difference in doses per fraction and their different biological effects. Doses can be expressed as the equivalent dose in 2 Gy fractions (EQD2). A tissue-specific α/β factor was used to calculate the equivalent dose. The α/β factor itself is determined using radiobiological testing and clinical experience. The precise α/β value for breast cancer tissue has not yet been determined; different values have been reported in the literature ranging from 2 to 5 (20). This range of values should be considered in studies of hypofractionated breast radiation, including H-SIB. In this context, there is also interest in radiation techniques that facilitate steep dose gradients between the boost PTV and whole breast PTV or between the whole breast PTV and surrounding normal tissue, where excessively high maximum doses should be avoided to minimise the probability of radiation-induced side effects (21-23).
A relatively new development in percutaneous photon radiation therapy is helical intensity modulated radiotherapy (IMRT), called tomotherapy. In most cases, this technique achieves the steepest dose gradient (conformity index close to 1), lowest values of dose maxima, and best dose homogeneity within the target volume compared to other IMRT and rotational techniques (24, 25).
The technical details of helical tomotherapy have been described previously (22). Briefly, a tomotherapy unit is a hybrid comprising a 6-MV linear accelerator and a helical CT scanner. Treatment is applied using a rotating fan beam; as the patient moves through the gantry bore, the treatment beam forms a helix (26, 27). The beam is modulated by a very fast-moving, pneumatically driven, binary multileaf collimator (MLC). In an inverse treatment-planning process, the MLC conformation is optimised to obtain highly conformal radiation doses at the target (28). The TomoEdge technique was recently introduced in tomotherapy as a technological development that minimises the dose penumbra at cranial and caudal field borders by modulating the primary collimators. In many cases, this tool shortens treatment duration by factor two with no compromise on plan quality (29).
This comparative plan study examined a range of methods for applying an additional boost in percutaneous breast radiotherapy using helical IMRT (tomotherapy) with TomoEdge. We compared the radiation does exposure to the mammary gland tissue and surrounding organs at risk (OAR). We focused on the effect of H-SIB and on uncertainty regarding α/β values for breast cancer tissue observed in the literature.
Patients and Methods
Patients. Ten patients with left-sided, nodal negative breast cancer were enrolled in this comparative plan study. All patients underwent breast-conserving surgery and were indicated for adjuvant radiotherapy (RT). The study was conducted according to the World Medical Association Declaration of Helsinki and the ICMJE Recommendations for the Protection of Research Participants and approved by the ethics committee of the Landesärztekammer Baden-Württemberg, Stuttgart, Germany (AZ: F-2015-063).
Imaging and regions of interest (ROIs). Patients were imaged using a CT scanner with a slice thickness of 5 mm. A wing step (breast tilting board) and leg fixation were used for optimal positioning. The scans were performed with the patients breathing freely with lifted arms. The left and right lungs, right breast, whole heart, and left ventricle were all delineated on CT images as OAR.
Target volumes were defined according to the institutional standards; the PTV of the treated breast included the whole mammary gland and chest wall behind it with a safe lateral, cranial, and caudal margin of 2 cm and a safe medial margin of 1 cm. The planning target volume of the boost volume (BV) included a tumour bed defined by surgical clips, architectural distortion, or seroma with a safe margin of 8 mm in all directions. The BV was always inside the PTV. A 1-cm-thick auxiliary structure (shell) was created around the BV to evaluate the dose gradients.
Treatment schemes. Five different treatment plans were generated for each patient. A normal-fractionated plan (N) and a hypofractionated plan (H) for PTV irradiation, a normal fractionated plan for SB, as well as a normal fractionated and hypofractionated plan for SIB. These five plans resulted in four different treatment schemes:
a) H-SIB: cumulative dose of 42.4 Gy (PTV) or 54.4 Gy (BV) in 16 fractions of 2.65 Gy or 3.4 Gy single doses, respectively.
b) normofractionated radiotherapy with simultaneous integrated boost application (N-SIB): cumulative dose of 50.4 Gy (PTV) or 64.4 Gy (BV) in 28 fractions of 1.8 Gy or 2.3 Gy single doses, respectively.
c) hypofractionated radiotherapy with sequential boost application (H-SB): cumulative dose of 42.4 Gy (PTV and BV) in 16 fractions of 2.65-Gy single doses plus 16 Gy (BV) in eight fractions of 2 Gy single doses.
d) normofractionated radiotherapy with sequential boost application (N-SB): cumulative dose of 50.4 Gy (PTV and BV) in 28 fractions of 1.8 Gy single doses plus 16 Gy (BV) in eight fractions of 2 Gy single doses.
Plan creation. All plans were generated for a tomotherapy planning system using TomoEdge (Version 5.1.1.6). This is a helical IMRT system with a 6-MV photon beam and an integrated planning software for inverse planning. A beam field width of 2.5 cm was applied for all plans, and the calculations were performed using a fine dose grid. The pitch was set to 0.282 (30) and a modulation factor between 2.4 and 3 was applied. The optimisation of each plan aimed to reduce the dose in all OAR (especially the left lung and heart), while covering the PTV and BV with at least 95% of the prescribed dose. All plans were created by the same person with high expertise to avoid inter-individual factors. The created plans were checked by a second expert according to the four-eye principle.
Plan evaluation. To evaluate the SB plans, tomotherapy planning software was used to calculate the cumulative dose-volume histogram (DVH) for each of the N-SB and H-SB schemes in each patient. All seven plans (H, N, SB, N-SB, H-SB, N-SIB, H-SIB) were exported to R-Studio (R-based analysis software) for further analysis and statistics.
The mean DVH was calculated across all patients for each treatment scheme. The conformity index (CI) was determined for the BV and PTV, including the BV (PTVIB). Where the term ‘PTV’ is used in further description of the methods and results, it excludes the BV. The CI was calculated as CI=V95(T)2/(V(T)•V95(tot)) (31), where V95 represents the 95% isodose of the prescribed dose in the target [V(T)=BV or V(T)=PTVIB] and the isodose in the total volume V(tot). The CI can reach a maximum of one, which means perfect conformity, when V95(T) is equivalent to V(T). The homogeneity of the PTV and BV is described using the homogeneity index HI=(D2-D98)/D50, where D2, D50, and D98 represent the doses covering 2%, 50%, and 98% of the region under consideration, respectively. The optimum HI is zero, with higher values representing poorer homogeneity.
The linear quadratic model was used to compare the radiation exposure of each treatment scheme. This shows the difference in dose per fraction and their different biological effects. Doses are expressed as equivalent doses in 2 Gy fractions (EQD2). The calculation used is as follows: EQD2=d•n•{(d+[α/β])/(d2+[α/β])}, where n is the number of fractions, d is the dose per fraction, d2 is the reference dose per fraction of 2 Gy, and α/β is the radiation response of different tissue types (32). Throughout our analysis, α/β=3 Gy was used for all OARs, while for the PTV, BV, and shell, different values were used ranging from 2.2 Gy to 4.6 Gy in 0.8-Gy increments to reflect the spread of α/β values in breast cancer as reported in the literature (20).
The mean dose values for the SB schemes were calculated separately for the main and SB plan, and then summed up afterwards. This meant that the EQD2 could be calculated properly considering the differences in radiation exposure per fraction between the main and SB plans. Boxplots were created to compare different treatment schemes. Averaged absolute values were presented with standard deviation (+/–). Two different schemes were compared directly using paired t-tests. All t-test results presented are calculated assuming a null hypothesis and a confidence interval of 0.95. We assumed a statistical significance for results with p≤0.05.
Results
Patients. The mean absolute planning target volume (PTV) in the left breast across enrolled patients was 1068 cm3, ranging 427-2332 cm3. The mean absolute BV was 154 cm3 (range=41-458 cm3). An example of the dose distribution for all four treatment schemes is shown in Figure 1.

An example of the dose distribution of four different boost application schemes in adjuvant radiotherapy of a female patient with left-sided breast cancer after breast-conserving surgery using helical tomotherapy with TomoEdge technique is shown. In the computer-tomography slice, the planning target volume (PTV) of the whole left breast is marked with red outlines and the boost volume (BV)/tumour bed is marked with violet outlines. A) H-SIB: hypofractionated radiotherapy with simultaneous integrated boost (SIB) (42.4/54.4 Gy in 16 fractions). B) N-SIB: normofractionated radiotherapy with SIB (50.4/64.4 Gy in 28 fractions). C) H-SB: hypofractionated radiotherapy with sequential-boost (SB) (42.4 Gy in 16 fractions + 16 Gy in 8 fractions). D) N-SB: normofractionated radiotherapy with SB (50.4 Gy in 28 fractions + 16 Gy in 8 fractions). The relative isodoses of the described PTV and BV doses are shown.
OAR. Figure 2 shows a statistical comparison of the mean dose in terms of EQD2 for all OARs and each treatment scheme. The radiation exposure was similar, and only small differences were observed. The minimal mean dose values for the left lung for each treatment scheme were associated with one patient, which seems to be because she had the smallest PTV and BV of all subjects. The high dose outliers, i.e., the maximum values for H-SIB and H-SB for the heart and left ventricle also belong to one patient. This patient is notable because of the relatively small distance between the BV and the heart.

Box plot (the small square within the boxes indicates the average value, the line within the boxes indicates the median value, the box the range from 25th to 75th percentile, the whiskers the range from minimum to maximum and the rhombs the outliers) comparing the planned mean dose (EQD2) of the left (L) and right (R) lung, the heart, the left ventricle and the ipsilateral breast over all patients for all regarded treatment schemes for left-sided breast irradiation. H-SIB: Ηypofractionated radiotherapy with simultaneous integrated boost (SIB); N-SIB: normofractionated radiotherapy with SIB; H-SB: hypofractionated radiotherapy with sequential boost (SB); N-SB: normofractionated radiotherapy with SB.
Table I shows the mean value in terms of EQD2 for each OAR across all patients and results of the t-test comparison of each treatment scheme with H-SIB plans. The lowest values were achieved using hypofractionated treatments [e.g. H-SIB left lung: 7.64±0.97 Gy (standard deviation); heart: 3.25±0.62 Gy]. While both normofractionated schemes applied a significantly higher mean dose to all OAR, no significant differences were found between the H-SIB and H-SB plans, except with regard to the left ventricle (2.74±0.46 Gy vs. 3.02±0.74 Gy, respectively, p=0.034).
Averaged mean dose (EQD2, calculated with α/β=3 Gy) of organs at risk with standard deviation of all patients and all examined treatment schemes and the p-value of the paired t-test comparison with the H-SIB scheme.
DVH, CI, and HI. The raw mean DVH (no EQD2 used) for the PTV including the BV (PTVIB) across all patients and for each treatment scheme are illustrated in Figure 3. Independent of the differences in the prescribed dose, a difference in the shape was observed between the SIB and SB plans. The less pronounced edge between the prescribed PTV and BV dose indicates a worse dose gradient for SB schemes.

Comparison of the dose-volume histogram (DVH). Averaged physical doses for the planning target volume of the treated breast including the boost volume (PTVIB) of all patients for all examined treatment schemes. H-SIB: Hypofractionated radiotherapy with simultaneous integrated boost (SIB), N-SIB: normofractionated radiotherapy with SIB, H-SB: hypofractionated radiotherapy with sequential boost (SB), N-SB: normofractionated radiotherapy with SB.
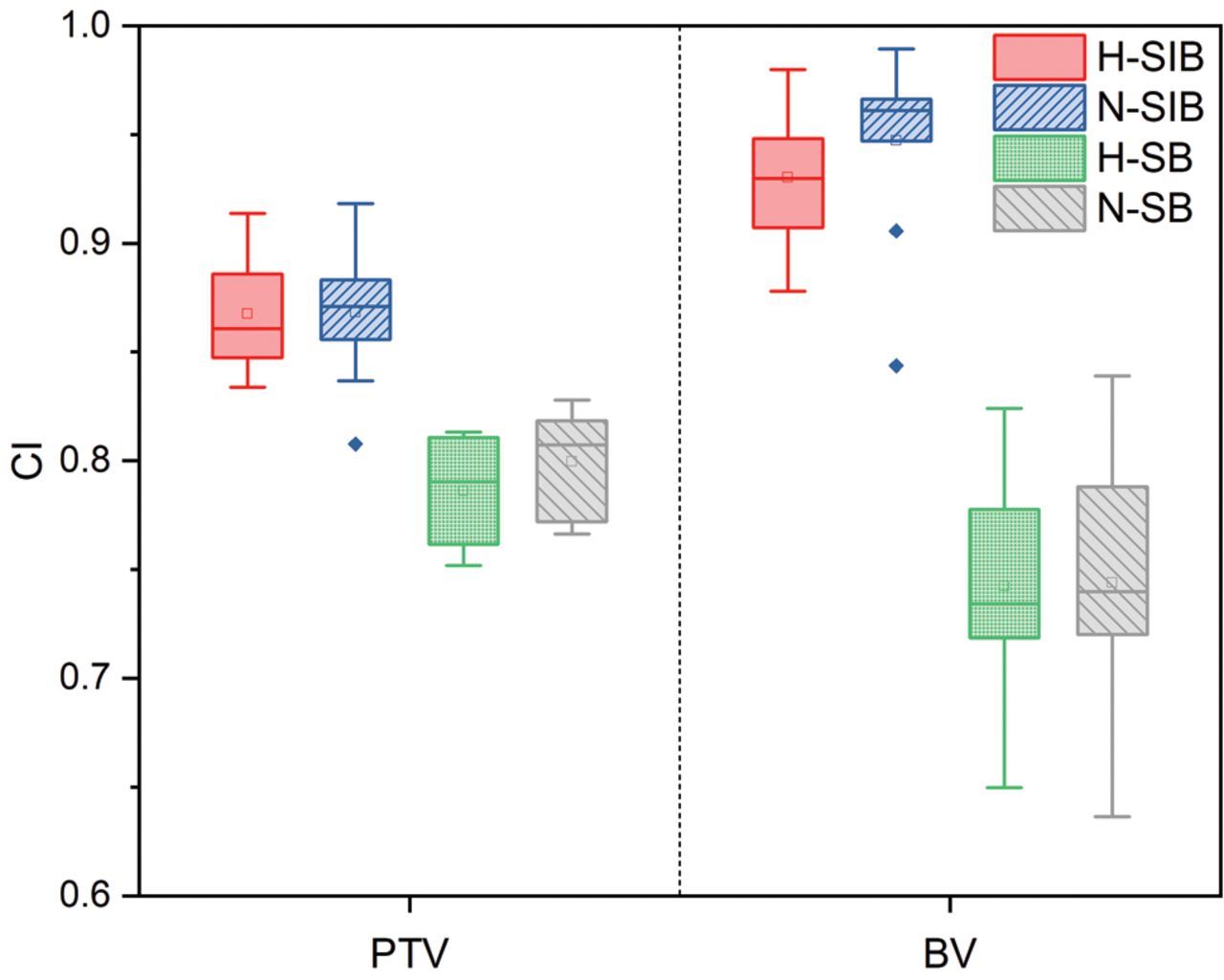
The conformity of dose distribution in the PTV and BV was also significantly higher for SIB treatment schemes than for SB schemes, as shown in Figure 4. In particular, the SIB techniques had very high CIs in the BV. The N-SIB plans offered the best conformity (averaged CI=0.947±0.043), but the CI from the H-SIB plans was not significantly different (0.93±0.032) (Table II).

Box plot (the small square within the boxes indicates the average value, the line within the boxes indicates the median value, the box the range from 25th to 75th percentile, the whiskers the range from minimum to maximum and the rhombs the outliers) comparing the conformity index (CI) of the planning target volume (PTV) of the treated breast (left part) and boost volume (BV) (right part) of all patients for all examined treatment schemes. H-SIB: Hypofractionated radiotherapy with simultaneous integrated boost (SIB), N-SIB: normofractionated radiotherapy with SIB, H-SB: hypofractionated radiotherapy with sequential boost (SB), N-SB: normofractionated radiotherapy with SB.
Averaged conformity index and homogeneity index with standard deviation for both, the planning target volume of the treated breast and boost volume, of all patients and all examined treatment schemes and the p-value of the paired t-test comparison with the H-SIB scheme.
The analysis of homogeneity, shown in Figure 5 and Table II, yielded significantly lower averaged HIs in the PTV for SIB plans (N-SIB: 0.205±0.022 (standard deviation); H-SIB: 0.225±0.008) than for SB plans (N-SB: 0.288±0.010; H-SB: 0.336±0.012; p<0.001). For the BV, the SB technique resulted in significantly better homogeneity of dose distribution. Comparing the HIs of the PTV and BV with each other, distinctly lower averaged values were found for the BV in all plans (e.g. N-SB PTV: 0.288±0.01 vs. BV: 0.0251±0.0051, p<0.001). N-SIB and H-SIB showed slight but not significant, differences in homogeneity for both PTV and BV.

Box plot (the small square within the boxes indicates the average value, the line within the boxes indicates the median value, the box the range from 25th to 75th percentile, the whiskers the range from minimum to maximum and the rhombs the outliers) comparing the homogeneity index (HI) of the planning target volume (PTV) of the treated breast (left part) and boost volume (BV) (right part) of all patients for all examined treatment schemes. H-SIB: Hypofractionated radiotherapy with simultaneous integrated boost (SIB), N-SIB: normofractionated radiotherapy with SIB, H-SB: hypofractionated radiotherapy with sequential boost (SB), N-SB: normofractionated radiotherapy with SB.
PTV, BV, and shell. The data presented in Figure 6 and Table III show the effect of different α/β values on the mean dose to the PTV. For the H-SIB and H-SB plans, the mean EQD2 dose increased with decreasing α/β; the opposite pattern was observed in the N-SIB and N-SB plans. This correlation arises from the reference fraction dose of 2 Gy (EQD2). All regions with a fraction dose below this show an increase, while all regions with a fraction dose above it show a decrease when α/β increases. Depending on the difference between the original and reference fraction doses, this effect is more or less pronounced. Comparing the normofractionated plans with one another and hypofractionated plans with one another, the SIB plans generally resulted in a significantly lower averaged mean dose. The dependence on α/β was balanced for α/β=3 Gy; no significant differences were obtained using hypofractionated versus normofractionated plans [e.g. N-SIB: 48.83±0.32 Gy (standard deviation); H-SIB: 48.84±0.36 Gy, p>0.05].

Box plot (the small square within the boxes indicates the average value, the line within the boxes indicates the median value, the box the range from 25th to 75th percentile, the whiskers the range from minimum to maximum and the rhombs the outliers) comparing the mean dose (EQD2) of the planning target volume (PTV) of the treated breast of all patients for all examined treatment schemes assuming four different values of α/β. The α/β values are arranged and start with the lowest assumed value on the left and end with the highest on the right. H-SIB: Hypofractionated radiotherapy with simultaneous integrated boost (SIB), N-SIB: normofractionated radiotherapy with SIB, H-SB: hypofractionated radiotherapy with sequential boost (SB), N-SB: normofractionated radiotherapy with SB.
Averaged mean dose (EQD2, calculated with different α/β values) with standard deviation of the planning target volume, boost volume, and shell of all patients and all examined treatment schemes and the p-value of the paired t-test comparison with the H-SIB scheme.
Evaluation of the BV (Figure 7 and Table III) clearly shows higher mean doses (EQD2) for SIB plans across all α/β values. Notably, at α/β=2.2 Gy, there was a difference of 11.3% (H-SIB vs. H-SB) and 8% (N-SIB vs. N-SB) in the mean dose. A direct comparison of all schemes against the H-SIB scheme shows a significantly lower averaged mean dose for both SB schemes (e.g. H-SIB: 66.94±0.21 Gy vs. H-SB: 62.78±0.26 Gy, α/β=3.8 Gy, p<0.001). Compared with that for H-SIB, the N-SIB scheme also produced significantly lower results for α/β=2.2 Gy and α/β=3 Gy but showed similar results for α/β=3.8 Gy and significantly higher results for α/β=4.6 Gy (H-SIB: 65.38±0.2 Gy vs. N-SIB: 66.63±0.18 Gy, p<0.001).

Box plot (the small square within the boxes indicates the average value, the line within the boxes indicates the median value, the box the range from 25th to 75th percentile, the whiskers the range from minimum to maximum and the rhombs the outliers) comparing the mean dose (EQD2) of the boost volume (BV) of all patients and all examined treatment schemes assuming four different values of α/β. The α/β values are arranged and start with the lowest assumed value on the left and end with the highest on the right. H-SIB: Hypofractionated radiotherapy with simultaneous integrated boost (SIB), N-SIB: normofractionated radiotherapy with SIB, H-SB: hypofractionated radiotherapy with sequential boost (SB), N-SB: normofractionated radiotherapy with SB.
Figure 8 and Table III show the analysed data for the shell (1-cm-thick auxiliary structure around the BV to evaluate dose gradients). For α/β=2.2 Gy, the H-SIB scheme had significantly higher averaged mean EQD2 values (58.3±0.69 Gy) than all other schemes (all p<0.05). The N-SIB plans resulted in the lowest mean dose and were still significantly lower for α/β=3 Gy, while the H-SIB and both SB schemes produced comparable values. Higher α/β values led to significantly lower averaged mean doses in the H-SIB plans than in the other schemes, with a drop to a significantly lower point than in either SB scheme (e.g. H-SIB: 54.35±0.57 Gy vs. H-SB: 55.60±1.04 Gy, α/β=4.6 Gy, p<0.001). For α/β=3.8 Gy and 4.6 Gy, the N-SIB plans were similar to the H-SIB plans and no significant difference in averaged mean dose was observed (e.g. N-SIB: 54.93±1.58 Gy vs. H-SIB: 55.3±0.6 Gy, α/β=3.8 Gy).

Box plot (the small square within the boxes indicates the average value, the line within the boxes indicates the median value, the box the range from 25th to 75th percentile, the whiskers the range from minimum to maximum and the rhombs the outliers) comparing the mean dose (EQD2) of the shell (a 1-cm thick auxiliary structure around the boost volume) of all patients and all examined treatment schemes assuming four different values of α/β. The α/β values are arranged and start with the lowest assumed value on the left and end with the highest on the right. H-SIB: Hypofractionated radiotherapy with simultaneous integrated boost (SIB), N-SIB: normofractionated radiotherapy with SIB, H-SB: hypofractionated radiotherapy with sequential boost (SB), N-SB: normofractionated radiotherapy with SB.
Discussion
This is a comparative plan study of different radiation techniques using helical tomotherapy with TomoEdge technology (H-SIB, N-SIB, H-SB, and N-SB) used to irradiate the left breast and include an indication for a radiation boost following breast-conserving surgery for breast cancer. Ten patients were included, and the results of interest are outlined below. First, we were able to show that radiation exposure of surrounding OAR, such as the contralateral breast, heart, and lungs, can be significantly reduced by implementing a hypofractionated radiation method at mid-EQD2. No significant difference was observed between the two hypofractionated groups (H-SIB and H-SB).
Further, the data produced by this study show that using a simultaneous integrated boost, whether normo- or hypofractionated, always produces greater conformity in both the PTV and the boost volume (BV). No significant difference was observed between the two SIB groups (H-SIB and N-SIB) in this regard. The improvement in conformity achieved by using a simultaneous integrated boost also induces a steep dose gradient within the PTV moving to the BV. This greatly reduces the excess dose burden to the PTV. On the other hand, both hypofractionated techniques produced more inhomogeneous dosing within both the PTV and BV.
In the literature, analyses of mean equivalent dose (EQD2) to breast cancer tissue have not produced a consensus regarding the precise α/β value, with acceptable options ranging from 2.2 to 4.6 Gy (20). One main explanation for the reported heterogeneity of reported α/β values is the different histological types and subtypes of breast cancer tissue. For this reason, calculations were carried out using different α/β values across the accepted range (2.2 Gy, 3 Gy, 3.8 Gy, and 4.6 Gy). This applies to the analysis of the mean equivalent dose to the PTV, BV, and shell (1-cm border around the BV). For the PTV, dose application using simultaneous integrated boost, both normo- and hypofractionated, showed mean EQD2 close to 50 Gy and below for all assumed α/β values tested. In contrast, techniques using sequential boost application tended to result in a mean EQD2 above 50 Gy. For the H-SIB and H-SB plans, the mean EQD2 dose increased parallel to decreasing α/β; the opposite behaviour was observed in the N-SIB and N-SB plans. Overall, the EQD2 in the PTV in all cases dropped within a range in which adequate local control and no increase in clinical side effects would be expected (2, 3). In the 1cm-border around the boost volume (the shell), which falls within the PTV, we observed that sequential boost radiation produced almost identical mean EQD2 values, i.e. between 55 and 57.5 Gy, for a range of assumed α/β values, regardless of whether the radiation was normo- or hypofractionated. The normofractionated SIB group consistently had low EQD2 values in the shell, lower than 56 Gy, across all assumed α/β values. The H-SIB method showed strong dependence on the mean EQD2 in the shell volume. At an α/β value of 2.2, the median EQD2 was over 58 Gy. This decreased continuously as the value of α/β increased. At an α/β value of 4.6 Gy, the median EQD2 was only 54 Gy. The optimum goal would be a median EQD2 as close as possible to 50 Gy in the PTV and shell volume (2, 3). This would provide sufficient cancer control whilst minimising the risks of fibrosis and fat necrosis in the shell. Even independently of the different assumed α/β values, all investigated radiation methods produced comparable exposure doses in the PTV and shell. Therefore, similar rates of tumour control and side effects would be expected here.
An analysis of the BV showed that both the normo- and hypofractionated SB groups achieved relatively stable median EQD2 values of 63-65 Gy regardless of the assumed α/β value. Compared to the SB groups, the SIB groups had significantly higher mean EQD2 values but a proportional inverse relationship to increasing assumed α/β values (from 2.2 to 4.6 Gy) (20). One may postulate that SIB, particularly H-SIB, may achieve improved local control in the BV. However, the risk of late-onset side effects, such as fibrosis or fat necrosis, may also increase (10, 13). Confirmation of long-term results in clinical, prospective, randomised trials is required to evaluate these issues.
Among the different methods for intensity-modulated radiotherapy (IMRT), helical tomotherapy stands out for its highly conformal and homogeneous dose distribution (24, 25). Therefore, helical tomotherapy often results in better conformity and homogeneity index scores than other IMRT techniques, such as step-and-shoot IMRT and volume-modulated arc therapy (VMAT) IMRT (33, 34). These indices are important in protecting normal tissue and achieving optimum dose application in the tumour region (11, 31). Moving onto dose coverage in the PTV and BV, helical tomotherapy with the TomoEdge technique generally complies with the specification for every volume fraction to receive at least 95% and less than 107% of the prescribed dose (29). According to the ICRU guidelines, compliance with this specification is a prerequisite for achieving the primary goal of optimal cancer control while also minimising toxicity rates. These specifications could be met using all plans calculated in this study, regardless of the boost application type and fractionation. The results of this study show that applying a simultaneous integrated boost using helical IMRT, whether hypofractionated or normofractionated, achieved significantly higher CI values than sequential boost application techniques. This was the case for both the PTV and BV. Regarding the shell region within the PTV, i.e. the 1-cm-thick volume surrounding the BV, we showed that N-SIB always produced the lowest median EQD2 values in the range of assumed α/β values, although the EQD2 always exceeded 50 Gy. At low α/β values, the H-SIB was not significantly worse than H-SB. With increasing α/β values, the H-SIB was improving, as N-SIB did. Comparing H-SIB to the other boost techniques for mean EQD2 in the PTV (excluding the BV), we found that this method produces doses of 50 Gy (α/β=2.2 Gy), with lower doses at increasing α/β values. As far as we are aware, there are no equivalent analyses of boost application procedures in adjuvant breast radiation using other IMRT techniques, such as standard IMRT or VMAT, alongside their dependence on different assumed α/β values.
Based on our results, we would not expect that the use of H-SIB using helical IMRT with the TomoEdge technique results in different tumour control rates or in an increase of late-onset toxicity risks in the PTV (excluding the BV) compared with that observed in other treatment schemes.
Regarding the BV, SIB generally led to significantly higher EQD2 for all tested α/β values. This was highest using H-SIB at an assumed α/β value of 2.2 Gy and reduced as α/β values increased. Clinically, this could mean that improved long-term local control in the BV would be more likely when using H-SIB and N-SIB than employing sequential boost techniques. However, increased rates of late-onset toxicities, such as fibrosis or fat necrosis, are also possible. No long-term results are available for the phase I and II studies published thus far.
Currently, clinical data are available from individual phase I and II studies investigating the acute toxicity of hypofractionated adjuvant breast radiotherapy using simultaneous integrated boost (H-SIB) following breast-conserving surgery. These studies used conventional tangential beam 3D techniques (3D-CRT), step-and-shoot IMRT techniques, and VMAT and reported only mild early onset toxicities (35-38). Long-term results of randomised prospective phase III studies are needed before a clinical statement can be made regarding whether H-SIB produces higher toxicity rates than the gold standard, N-SB or H-SB, or in comparison to N-SIB, which is also well established in routine clinical use.
A study by van Parjis et al. investigated a total of 70 patients and compared side effect rates from N-SB using 3D-CRT to that from H-SIB using helical IMRT (tomotherapy) (39). The shortest follow-up period was 1 year and the longest was 3 years. H-SIB use showed a significant reduction in skin and lung toxicity after 2 years when compared to N-SB. The left ventricular ejection fraction was not significantly different. One limitation of this study is that the conventional 3D radiation method was compared with the highly conformal IMRT method, which facilitates very steep dose gradients. This means that the better results could be explained simply by the difference in quality between the two radiation methods rather than the type of fractionation. It should also be noted that the helical IMRT method used at the time was not the TomoEdge method, which was only developed later. The TomoEdge technique reduces the longitudinal dose exposure in normal tissue and can significantly reduce the treatment duration (29).
Paelinck et al. published a prospective randomised study comparing the early onset toxicities of H-SIB and H-SB using the same IMRT technique (VMAT). No significant difference was found in the primary endpoint of moist epitheliolysis. H-SIB produced significantly better results regarding the secondary endpoints of dermatitis and itching (40). For this study, patients were irradiated in the non-standard prone position, which makes the data difficult to compare with other datasets.
Currently, clinically sufficient data from randomised, prospective, phase III studies on late-onset toxicity comparing H-SIB to N-SB, H-SB, or N-SIB are not available. The aim should be to use a period of 5-10 years to draw conclusions that could change therapy standards.
Only two investigations on this topic are available, and both have limited informative value. De Rose et al. carried out a retrospective analysis of H-SIB in 831 patients, describing a relatively high rate of skin reactions after 2 years; however, these results were not confirmed after 5 years. The IMRT technique used was VMAT (41). Another study compared N-SIB to H-SIB using tangential beam 3D-CRT in both cases. After an average follow-up period of 7.2 years, patients were asked about their satisfaction with the cosmetic results. This study found a positive tendency toward H-SIB. No objective data on toxicity rates were collected (42).
H-SIB is currently an experimental technique in adjuvant radiotherapy for breast cancer and is under review in a large phase III study (HYPOSIB; NCT02474641). Valid clinical data on late-onset toxicities are therefore awaited. The data from our plan study do not show any obvious indications that would lead us to expect an increase in late-onset toxicities after H-SIB compared to currently used boost application methods. This statement is valid when radiation is applied using helical tomotherapy with TomoEdge technology. We can assume that this may also apply in principle to other IMRT techniques, although this should be confirmed by appropriate studies.
Further investigations are also needed to reduce the uncertainty regarding α/β values of breast cancer tissue in the literature and thus improve estimates of the radiation effect.
Conclusion
This study was the first to use a plan comparison to contrast hypofractionated radiotherapy with simultaneous-integrated boost, currently an experimental technique, with other common non-invasive methods for boost application (H-SB, N-SB, and N-SIB) in adjuvant radiotherapy using cutting-edge helical tomotherapy with TomoEdge technology following breast-conserving surgery. The dosimetric results provided no evidence that H-SIB would lead to different results regarding tumour control or late-onset side effects compared to other clinically standard treatment schemes when using helical tomotherapy with TomoEdge technology. Uncertainty still exists regarding the α/β values of breast cancer tissue, which was taken into account for our analysis. Long-term clinical results are awaited from randomised trials.
Footnotes
Authors’ Contributions
F.Z., M.S. and S.H. initiated and supervised the project. F.Z. and M.S. collected the data. M.S., F.Z., and C.K. performed the data analysis. M.S., F.Z., P.H., J.D. and S.H. interpreted the experimental data and were responsible for creating figures. F.Z. and M.S. wrote the manuscript with input from all Authors. All Authors have been involved in manuscript revisions.
This article is freely accessible online.
Conflicts of Interest
The Authors declare that there are no conflicts of interest in relation to this study.
- Received February 15, 2021.
- Revision received February 27, 2021.
- Accepted March 1, 2021.
This is an open access article distributed under the CC BY license (https://creativecommons.org/licenses/by/4.0/).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}