


Abstract
Background/Aim: Magnetic resonance imaging is used for staging purposes in cervical cancer (CC). Diffusion-weighted imaging and the apparent diffusion coefficient (ADC) are associated with tumor microstructure. The present analysis sought to compare pre-treatment ADC values to predict treatment outcome of radiochemotherapy for CC based upon a large patient sample. Materials and Methods: MEDLINE library and SCOPUS databases were assessed for suitable articles up to May 2020. The primary endpoint was the mean ADC value of CC according to the treatment response to radiochemotherapy. In total, 16 studies were included in the analysis. Results: For the response group, 416 patients were included in the analysis (72.5%) and for the no-response group 158 patients were included (27.5%). The mean ADC value of patients with CC with treatment response was 0.87×10−3 mm2/s (95% confidence interval=0.81-0.94×10−3 mm2/s), and for the patients with no response was 0.92×10−3 mm2/s (95% confidence interval=0.85-0.98×10−3 mm2/s). Conclusion: Pre-treatment ADC values alone cannot be used to reliably predict treatment response to radiochemotherapy in CC.
Magnetic resonance imaging (MRI) is clinically of great importance for the diagnosis of cervical cancer (CC) (1-4). It has a high sensitivity and can detect tumor infiltration of adjacent structures. Moreover, due to the addition of diffusion-weighted imaging (DWI), information regarding tumor characteristics such as cellularity can be obtained (5-7). DWI is a MRI sequence quantifying the Brownian water movement in tissues, which is inversely correlated with cell density in tumors (5-7).
It has been shown that apparent diffusion coefficient (ADC) values differ significantly between adenocarcinoma and squamous cell carcinoma due to different tumor microstructure (8). In addition, correlations with epidermal growth factor and p53 expression were also reported (7, 9). These data indicate that ADC values can also reflect tumor biology in a more complex way beyond cellularity alone (10).
There is no doubt regarding the benefit of neoadjuvant and definitive chemotherapy in CC (11). A clear survival benefit was shown for treatment responders, which is also shown by the fact that treatment response is an independent prognostic factor in CC (12). However, response rates range from approximately 50% to 92%, whereas the optimal pathological response is lower than 20% (11, 12).
To date, there are no imaging or histopathology modalities which can reliably predict treatment outcome of chemotherapy (11). Yet this approach would be clinically relevant for selecting patients who would benefit from the therapy and those who would not. Thereby, therapy-related toxicity could be reduced if ADC values were able to predict treatment outcome. Previously, preliminary studies indicated that ADC might be used as predictor of therapy response (3, 4).
The present analysis sought to systematically review studies of ADC values in CC according to treatment outcome after radiochemotherapy and to carry out a meta-analysis to elucidate whether ADC values differ significantly according to treatment response.
Materials and Methods
Literature search and inclusion criteria. MEDLINE library and SCOPUS databases were screened for studies investigating ADC values in CC up to May 2020. The following terms for the literature search were used: “Diffusion weighted imaging or diffusion-weighted imaging or DWI or Apparent diffusion coefficient or ADC AND cervical cancer OR cervical carcinoma”. Secondary references were screened and included, when suitable.
The primary endpoint was defined as the ADC values in patients with CC in regard to treatment outcome.
Studies were included when they met the following criteria: (i) Histopathologically confirmed CC, (ii) MRI with DWI before any form of treatment, and (iii) mean ADC values were reported with standard deviation.
The following were exclusion criteria: (i) Case reports, (ii) reviews, (iii) studies without data of pre-treatment DWI, (iv) articles not in English language, and (v) xenograft or animal model experimental study design.
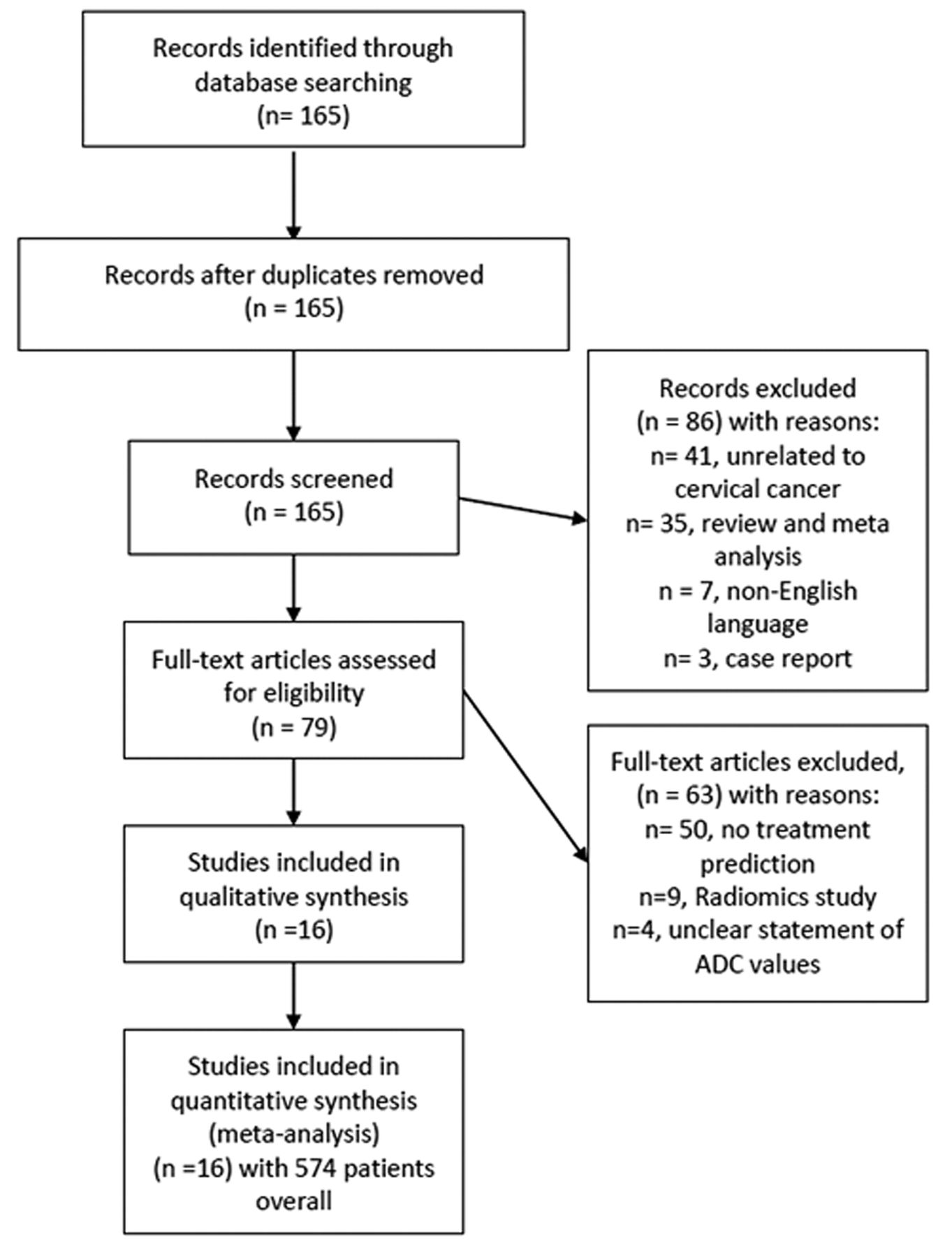
Article acquisition was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (13) (Figure 1). In total, 16 articles met the inclusion criteria and were included in the present analysis (14-29).
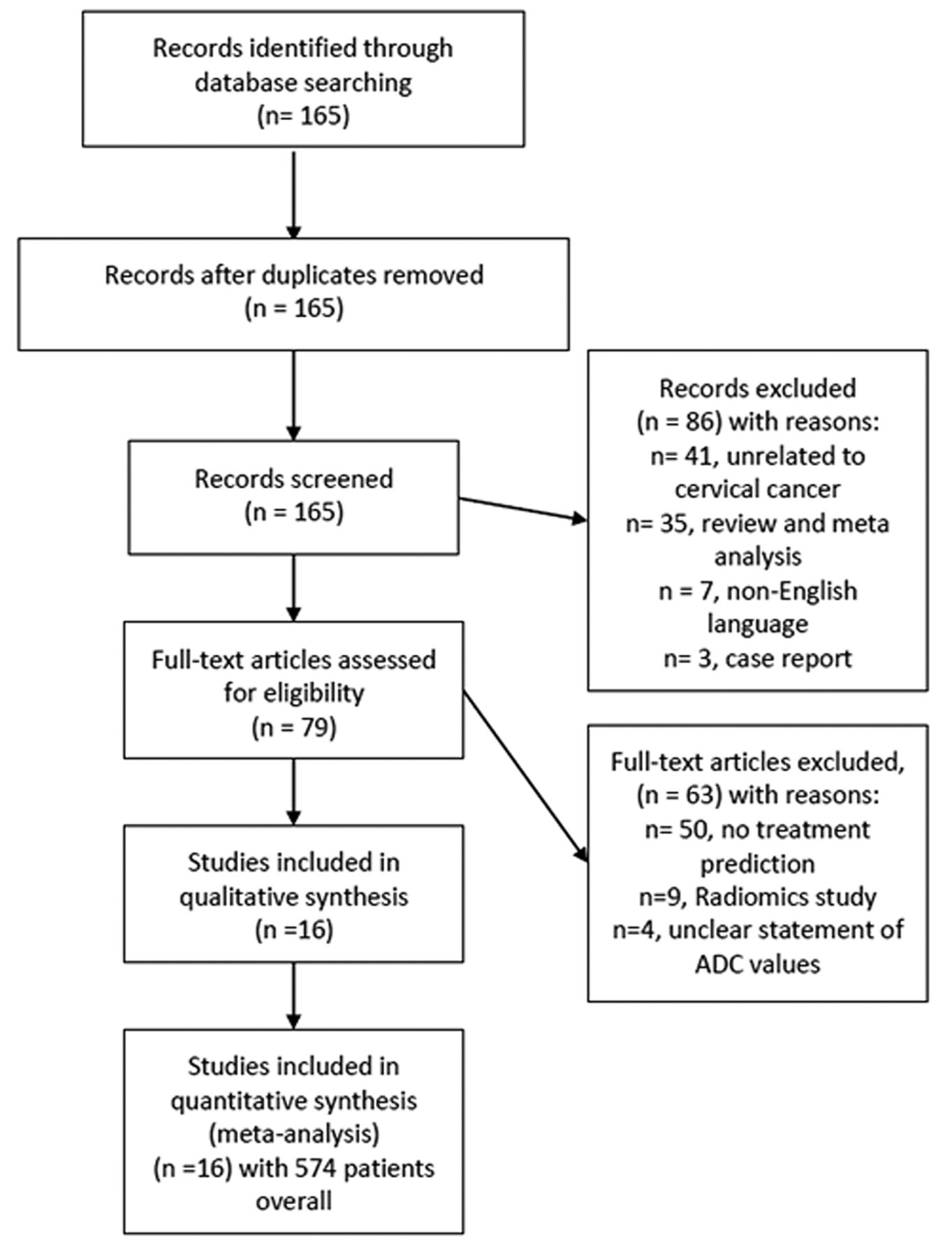
PRISMA flow chart gives an overview of article acquisition. Overall, 16 studies with 574 patients overall were included in the analysis. ADC: Apparent diffusion coefficient.
Quality assessment. The methodological quality of the included studies was independently assessed by two co-authors (A.S. and H.J.M.) using Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) (30).
Statistical analysis. The analysis was carried out with RevMan 5.3 (2014; Cochrane Collaboration, Copenhagen, Denmark). Heterogeneity of the results was estimated by the inconsistency index I2 (31, 32). DerSimonian and Laird random-effect models using inverse-variance weights were calculated without any form of correction (33).
Results
Figure 2 gives an overview of the methodological quality of the included studies. Overall, the risk of bias was considered low. Patient selection was regarded as overall well-defined within the respective methodology; yet some studies did not clearly define the inclusion criteria sufficiently enough, which can result in some form of potential bias. The index test defined as the MRI with DWI was clearly reported within the studies and should not be considered a source of potential bias. The DWI measurement can be considered as reliable throughout the studies. For flow and timing, there were no serious concerns to report, as in most studies no delay between imaging and treatment procedures were noticed.
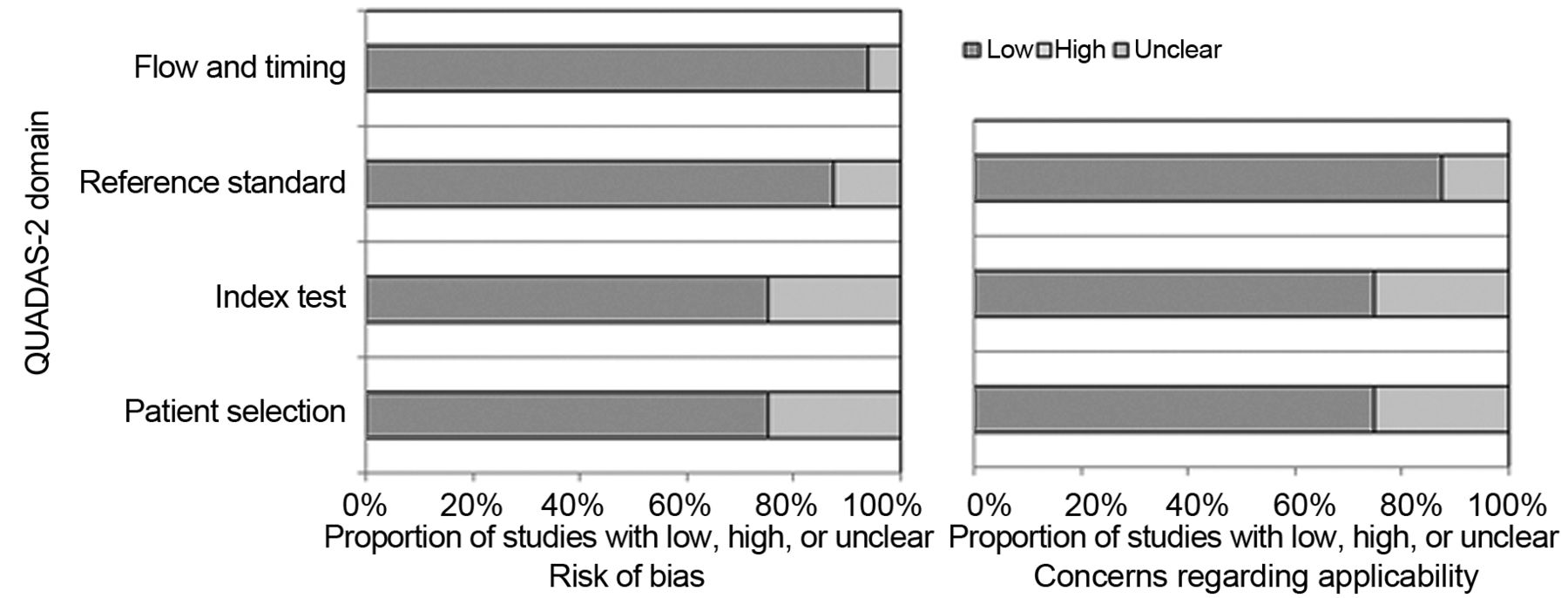
QUADAS-2 quality assessment of the included studies. Most studies showed an overall low potential for sources of bias.
The 16 studies included comprised a total of 574 patients with CC. Table I provides an overview of the included studies.
Data retrieved from the included studies.
Of the included studies, 10 (62.5%) were of prospective and six (37.5%) of retrospective design. Different 1.5T MRI scanners were used in five (31.3%) studies, 3T scanners in 10 (62.5%) studies, and one study (14) had an unclear scanner technique (6.2%). Regarding b-values, most studies used high b-values of 0 and 800 s/mm2 or higher in 14 studies (87.5%). In two studies (12.5%), no statement of b-values used was given (14, 16). In six studies (37.5%), squamous cell carcinomas and other histological entities were investigated, whereas in 10 studies (62.5%), only squamous cell carcinomas were included. Therefore, most patients had squamous cell carcinomas (n=537, 94.6%) and only 37 patients (6.4%) had other histological entities with 17 patients with adenocarcinomas comprising the second most common entity.
For tumor stages, most studies included different tumor stages ranging from International Federation of Obstetrics and Gynecology-stage IB to IV. Only two studies did not report the exact proportion of tumor stages of their patient sample but only the boundaries of included tumor stages (16, 21).
Different treatment regimens were performed in the studies. Concurrent radiochemotherapy was performed in eight studies (50%), neoadjuvant chemotherapy (25%) in four studies, definitive radiochemotherapy in two studies (12.5%), neoadjuvant radiochemotherapy in one study (6.25%), and in one study, concurrent radiochemotherapy as well as radiotherapy alone were used (23).
For the responder group, 416 patients were included in the analysis (72.5%) and 158 patients for the nonresponders (27.5%).
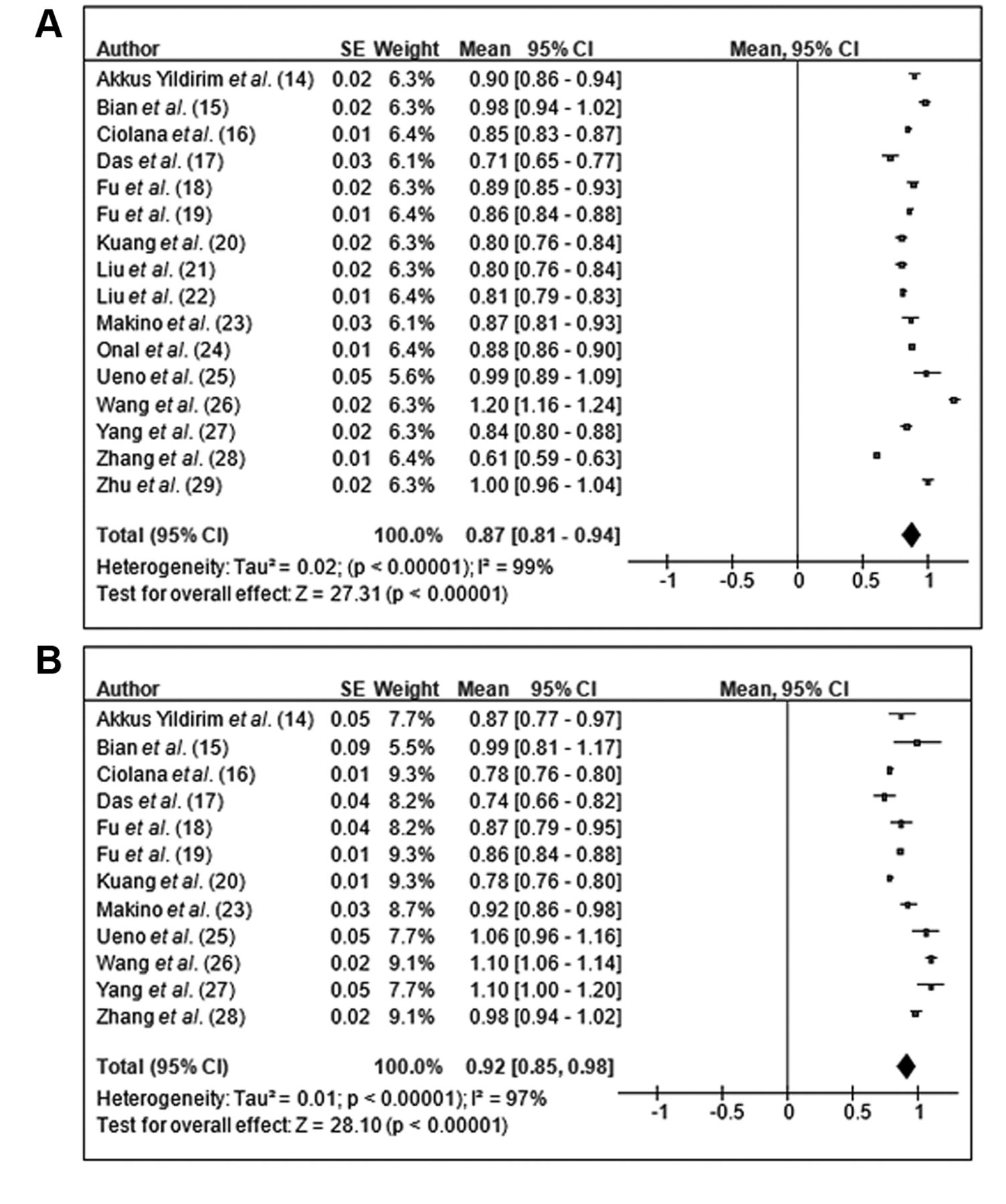
The mean ADC value for patients with treatment response was 0.87×10−3 mm2/s (95% confidence interval=0.81-0.94×10−3 mm2/s; Tau2=0.02, Chi2=1047.32, df=15, I2= 99%), and of the patients with no response was 0.92×10−3 mm2/s (95% confidence interval=0.85-0.98×10−3 mm2/s; Tau2=0.01, Chi2=355.61, df=11, I2=97%) (Figure 3). The high I2 value indicates substantial heterogeneity between the studies. Figure 4 shows these results as a box plot. The ADC values of the groups significantly overlapped with no clear threshold value to distinguish between them.
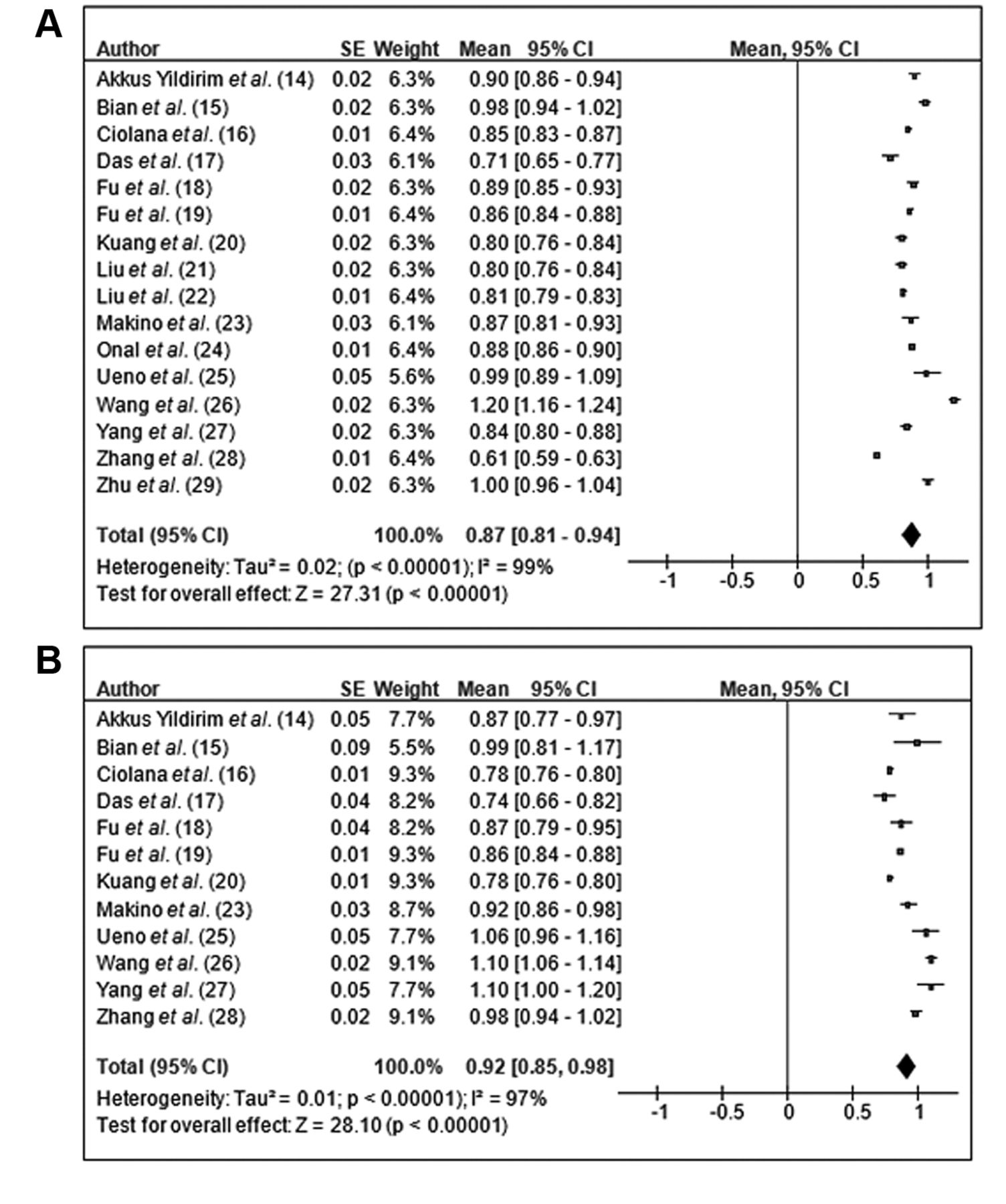
Forrest plots of the mean apparent diffusion coefficient (ADC) values of responders (A) and nonresponders (B) in patients with cervical carcinoma. The mean ADC value of patients with treatment response was 0.87×10−3 mm2/s (95% confidence interval=0.81-0.94×10−3 mm2/s), that of patients with no response was 0.92×10−3 mm2/s (95% confidence interval=0.85-0.98×10−3 mm2/s).

Box plots of the mean apparent diffusion coefficient (ADC) values according to treatment response. The ADC values for groups overlapped significantly, with no clear threshold value to distinguish between them.
Discussion
The present study sought to elucidate whether ADC values of DWI can predict treatment outcome of radiochemotherapy in CC. In short, there were no significant differences between patients with treatment response and those without response according to ADC values.
On the one hand, significantly lower ADC values of patients with treatment response were reported (27, 28), but on the other, ADC values were significantly higher for treatment responders (26). Of note, others did not identify significant differences for ADC values according to treatment response (14, 16, 25). Thus, the present analysis harmonizes the published incongruent results of previous single-centre studies based upon a large sample size.
It is known that radiochemotherapy significantly improves 5-year overall disease-free survival (hazard ratio=0.78) and 5-year overall survival (hazard ratio=0.81) compared to radiotherapy alone (11). There is no doubt that an optimal treatment response is an independent prognostic factor in CC (12). However, the objective response rates range from approximately 50% to 92%, whereas an optimal pathological response is only found in fewer than 20% of patients (11).
In the present analysis, different treatment regimens were included, comprising neoadjuvant chemotherapy and concurrent radiochemotherapy, which might have resulted in the identified heterogeneity of the results. Yet the pre-treatment ADC value was investigated in the present study, which should be predictive for any form of treatment as a valuable biomarker in clinical routine.
It was extensively reported that ADC values are associated with cellularity, cell density and tumor microstructure (5, 7, 9, 10). Moreover, ADC values are also correlated with clinically significant histopathological features, comprising proliferative potential and expression of tumor-suppressor gene TP53 (7, 9, 10). Yet there is still an ongoing debate as to which features of tumor biology are reliably reflected by non-invasive imaging and which not.
Regarding prediction of treatment response by ADC values, there have been promising results for several tumor entities, including head and neck cancer, rectal cancer, and soft-tissue sarcoma (34-36). One can assume that for studies which showed that treatment responders had lower ADC values, a higher cellularity and a higher tumor aggressiveness of the tumor might have resulted in a better treatment response, whereas patients with a higher pre-treatment ADC value might have had lower cellularity and a less aggressive tumor, which resulted in a less effective treatment. On the other hand, there might be the possibility that patients with a more aggressive tumor also have a worse treatment response, as was shown by Wang et al. (26). The relatively high heterogeneity of the underlying data has to be considered. Yet one key finding of this study is that ADC values pooled from the published results indicate that ADC values alone are not able to reliably predict treatment response in CC.
As well as the analysis of pre-treatment ADC values, which might be able to discriminate more aggressive tumors from more benign tumors, the increase of ADC values during treatment seems to be of relevance. This might show tumor regression induced by therapy. Yet in a recent meta-analysis, it was also shown that pre-treatment ADC values were not capable of predicting therapy response in patients with breast cancer in a neoadjuvant setting (37). In short, it is crucial to investigate for which tumor entities DWI and ADC values are useful for treatment prediction and for which ones these cannot be used.
For CC, the treatment response is mainly determined by conventional MRI and morphological measurement of the tumor, considering possible shrinkage (2). Beyond this, a significant T2-weighted signal loss indicates post-treatment fibrosis of the cervix as a result of radiochemotherapy, whereas a decrease in uptake of contrast medium in contrast-enhanced sequences indicates regression of vital tumor tissue, which are both important signs for treatment response (2). However, this assessment can only be made after the treatment and no pre-treatment prediction can be made with conventional imaging.
Notably, there are only few histopathological parameters which were investigated for treatment prediction. Only the proliferative index Ki67 and survivin expression remained statistically significant in a multivariate analysis based on 117 squamous cell cervical carcinomas undergoing neoadjuvant chemotherapy and were associated with treatment response (38).
Presumably, the reported differences in the investigated studies were influenced by different scanner technique, measurement of ADC values, and composition of the patient samples. For example, it is a known fact that adenocarcinoma tends to have different ADC values from squamous cell carcinomas (8).
The present analysis suffers from the following limitations. Firstly, the analysis is based upon results of the literature. There might be some publication bias due to the trend of positive or significant reported results. Secondly, only articles in English language were included. Thirdly, only studies employing clinically DWI sequence using two b-values were included. Yet novel DWI techniques such as intravoxel-incoherent motion and diffusion-kurtosis imaging might perform better for treatment prediction in CC (28, 39, 40). However, no meta-analysis can be performed including these currently with so few articles published. Fourthly, there was substantial inhomogeneity identified in the analysis.
In conclusion, pre-treatment ADC values alone cannot be used to reliably predict treatment response to radiochemo-therapy in CC.
Footnotes
This article is freely accessible online.
↵* All Authors contributed equally to this work
Authors’ Contributions
All Authors contributed equally to this work.
Conflicts of Interest
All Authors confirm that there are no conflicts of interest to be declared.
- Received January 17, 2021.
- Revision received February 13, 2021.
- Accepted February 15, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.