


Abstract
Background/Aim: The present study compared the accuracy of visually analyzed (VA) and automatically analyzed (AA) ColonView (CV) quick test; a new-generation immunochemical test (FIT) for Hb and Hb/Hp (Biohit Oyj, Helsinki, Finland) in subjects participating in colorectal cancer (CRC) detection in Brazil. A traditional gFOBT test (HemoccultSENSA) was used as a reference. Patients and Methods: A cohort of 368 colonoscopy-referral patients were asked to collect 3 consecutive fecal samples, to be analysed by both assays (CV, SENSA). Results: In receiver operating characteristic (ROC) analysis for the AA reading, the optimal cut-off value for CV Hb AA (test AA 3) was ≥117 and that for CV Hb/Hp AA (test AA 4) was ≥48. In the hierarchical summary receiver operating characteristic (HSROC) analysis for pooled accuracy of CV with AA and VA reading, the AUC values for i) VA and ii) AA were as follows: i) AUC=0.859 (95%CI=0.839-0.879), ii) AUC=0.931 (95%CI=0.920-0.942). The difference between these AUC values (Roccomp analysis) was statistically significant (p=0.0024). Conclusion: The present study confirms the previous studies on the applicability of the ColonView quick test (a new-generation FIT) in CRC screening.
- Fecal occult blood
- fecal immunochemical test
- FIT
- colorectal cancer screening
- sensitivity
- specificity
- false negative
- false positive
- ROC
- HSROC
Previous randomized studies suggest that fecal occult blood test (FOBT) screening can reduce mortality from colorectal cancer (CRC) (1-5). Fecal occult blood (FOB) is measured using either the traditional guaiac-based tests or more recently introduced fecal immunochemical tests (FITs) (6-8). FITs have several advantages over guaiac-based FOBTs, including higher sensitivity and specificity, resulting in improved clinical performance and higher efficiency (6-8). According to European guidelines for quality assurance in CRC screening, another advantage in population screening is that FITs can be automated and user can adjust the cutoff at which a positive result is reported (9).
Since the invention of the immunochemical test principle by Suovaniemi et al. (10) in the 1980’s, an increasing number of FITs have been developed, particularly in Japan, the pioneering country of CRC screening, where different FITs have been the principal screening method since the early 1990’s (8, 9). The FIT is based on the detection of the globin moiety of human hemoglobin or its degradation products. Although a plethora of FOBTs is available on the market, relatively few have been extensively tested for clinical sensitivity and specificity in CRC screening. Current data imply that new FITs have superior test characteristics as compared with guaiac-based FOBTs. As shown in our (8) recent meta-analysis, the ColonView quick test (CV; Biohit Oyj, Helsinki, Finland) is superior to the traditional guaiac-based FOB tests (gFOBT, HemoccultSENSA), making CV a perfect fecal immunochemical test (FIT) for organized CRC screening.
Vasilyev et al. (11) and Guimaraes et al. (6) have previously compared the diagnostic accuracy of HemoccultSENSA (SENSA) and CV in a head-to-head comparison study among CRC screening patients. The present study is an extension of these analyses by applying hierarchical summary receiver operating characteristic (HSROC) and area under curve (AUC) analyses to test different cut-offs and to compare the diagnostic accuracy of the two reading modes of CV: Visual analysis (VA) and automatic analysis (AA), using CRC as the endpoint in colonoscopy-referral screening patients.
Patients and Methods
A cohort of 368 colonoscopy-referral patients were evaluated by the new-generation FIT: ColonView quick test (CV; Biohit Oyj, Finland). Three fecal samples were requested and all subjects underwent diagnostic colonoscopy with biopsy confirmation. The study was conducted at Barretos Cancer Hospital (BCH) (Barretos-SP, Brazil) and approved by the Institutional Review Board of the BCH (Registration number 753/2013). The patients attending the Outpatient Department of Endoscopy for an appointment to colonoscopy were enrolled in the study. Every patient was asked to read the patient information sheet, and agree to participate in the study by signing a written consent. Patients consenting to participate were given a box containing all necessary materials of FOB tests for sampling, as well as instructions for sample collection, handling and delivering to the test laboratory analysis at the day of colonoscopy. The study protocol (Figure 1) and inclusion/exclusion criteria of study patients were detailed in a previous report by Guimaraes et al. (6).

Flow-chart of the study.
Sample collection, processing and interpretation of results. The guaiac-based traditional FOBT (hemoccult SENSA, Beckman Coulter Inc., Passadena, CA, USA) was used as the reference in this study. This test needs compliance with certain restrictions in the daily diet and medication. To make the comparison of these two basically different tests as unbiased as possible, the Delivery Box contained detailed instructions for the patient preparation as well as precautions in diet and daily medication. Accordingly, the subjects were instructed to avoid non-steroidal anti-inflammatory drugs (more than one adult aspirin a day) for 7 days before and during the stool collection period. The sample collection protocol was described in more detail recently (6).
A new-generation FIT, ColonView® quick test (subsequently CV) (Biohit Oyj, Helsinki, Finland) does not necessitate any preparatory steps of the patient or compliance with any restrictions in the daily diet or medication. The subjects were instructed to collect 3 fecal samples on 3 consecutive days. For the CV test, the samples were collected into 3 separate tubes, following the manufacturer’s instructions. Test cards and tubes were returned to BCH laboratory at the day of colonoscopy and processed on the very same day.
The CV quick test consists of two components (Hb and Hb/Hp complex), and the test result has four options: both components negative, both components positive, either Hb or Hb/Hp complex positive. For the CV, two optional reading modes are available: VA and AA. The latter is performed by using opTrilyzer Lateral flow reader (Chembio Diagnostics GmbH, Berlin, Germany), as described before (6, 11). In fully compliant patients, 3 stool samples were tested by CV and the result was interpreted positive if any of the 3 samples tested positive. For CV, any sample positive for either Hb or Hb/Hp complex was classified as a positive test. The analytical sensitivity for CV Hb is 15 ng/ml, and for CV Hb/Hp complex, 4 ng/ml (12).
Normal colonoscopy was used as the gold standard indicating a negative result regarding the study endpoints. All colonoscopies were performed by experienced endoscopists with high-definition colonoscope (Olympus GIF 180; Tokyo, Japan), using a targeted dye spraying of the colon with 0.4% indigo carmine solution. Detailed description of all detected lesions was provided, including their number, size and exact locations: proximal (from cecum to splenic flexure) or distal (descending colon to rectum), as described before (6).
Statistical analysis. STATA/SE version 17.0 (StataCorp, College Station, TX, USA) was used for analysis. The statistical tests presented were two-sided, and p-values <0.05 was considered statistically significant. Using 2×2 tables, sensitivity (Se) and specificity (Sp) with 95% confidence intervals (95%CI) for each FOB test was determined. Conventional receiver operating characteristic (ROC) analysis was used to graph for Se and Sp and to find the optimal cut-off values for both Hb and Hb/Hp of the CV test (Figure 2). Meta-analytical technique (metaprop) was used to create separate forest plots for Se and Sp, with each set of data included (i.e., test components Hb, Hb/Hp, cut-offs). We also calculated the summary estimates of Se and Sp, positive (LR+) and negative likelihood ratio (LR–) as well as diagnostic odds ratio, using a random effects bivariate model and fitted the summary hierarchical receiving operating characteristic (HSROC) curves for the CRC as the endpoint. Roccomp test was used to compare the statistical significance between the AUC (area under the curve) values for AA and VA modes.

Receiver operating characteristic (ROC) curve for test optimization and finding optimal cut-off point for the visually analyzed (VA) and automatically analyzed (AA) ColonView (CV) tests.
Results
Patient data of the study. The whole CRC cohort at BCH included 5090 patients, but due to various reasons, 4584 of the subjects had to be excluded (Figure 1). There were 506 eligible patients for the study, of whom, however, 138 patients were excluded due to missing stool samples. The final cohort included 368 colonoscopy-referral patients evaluated by the VA and AA reading modes of the CV tests. Three fecal samples were collected for both assays and all subjects underwent diagnostic colonoscopy with biopsy confirmation.
ROC analysis and optimal cut-off values of the CV. When CV Hb + Hb/Hp VA (test VA 4, Table I) was used as a combined test panel for the CRC endpoint, the panel had 90.7% Se, 50.9% Sp, and 54.9% Efficiency (Eff) (Table I). In the AA mode, the CV Hb (cut-off ≥117) + Hb/Hp (cut-off ≥48) (test AA 5, Table II) combined test panel had 88.1% Se, 86.1% Sp, and 86.3% Eff (Table II). The PV+ of the CV Hb (cut-off ≥117) + Hb/Hp AA (cut-off ≥48) test panel (test AA 5, Table II) was significantly higher than that of CV VA test panel; 41.6% versus 17.1% the latter showing a high proportion of false positive (FP) results.
Visually analyzed screening tests for colorectal cancer endpoint.
Automatically analyzed screening tests for colorectal cancer endpoint.
The ROC analysis showed the optimal cut-off value of ≥117 for CV Hb AA (test AA 3 Table II) and ≥48 for CV Hb/Hp AA (test AA 4, Table II). Using these cut-offs, the Se, Sp and Eff of the CV Hb AA (test AA 3, Table II) and CV Hb/Hp AA (test AA 4, Table II) tests detecting CRC were as follows: 81.0%/87.5%, 92.7%/86.4% and 91.6%/86.5%. The PV+ of test AA 3 (Table II) was significantly higher than that of test AA 4 (Table II); 55.7% versus 42.0%, indicating the proportion of the patients with a positive test result who have the disease.
Figure 2 shows the AUC values in ROC analysis of test AA 3 and test AA 4 for the CRC endpoint: 0.920 and 0.924, respectively. The combination of CV Hb AA and the CV Hb/Hp AA tests (test AA 5, Table II) showed significantly higher diagnostic accuracy than did CV VA and CV AA tests combined (AUC 0.918/0.924 versus 0.900, respectively, p<0.001).
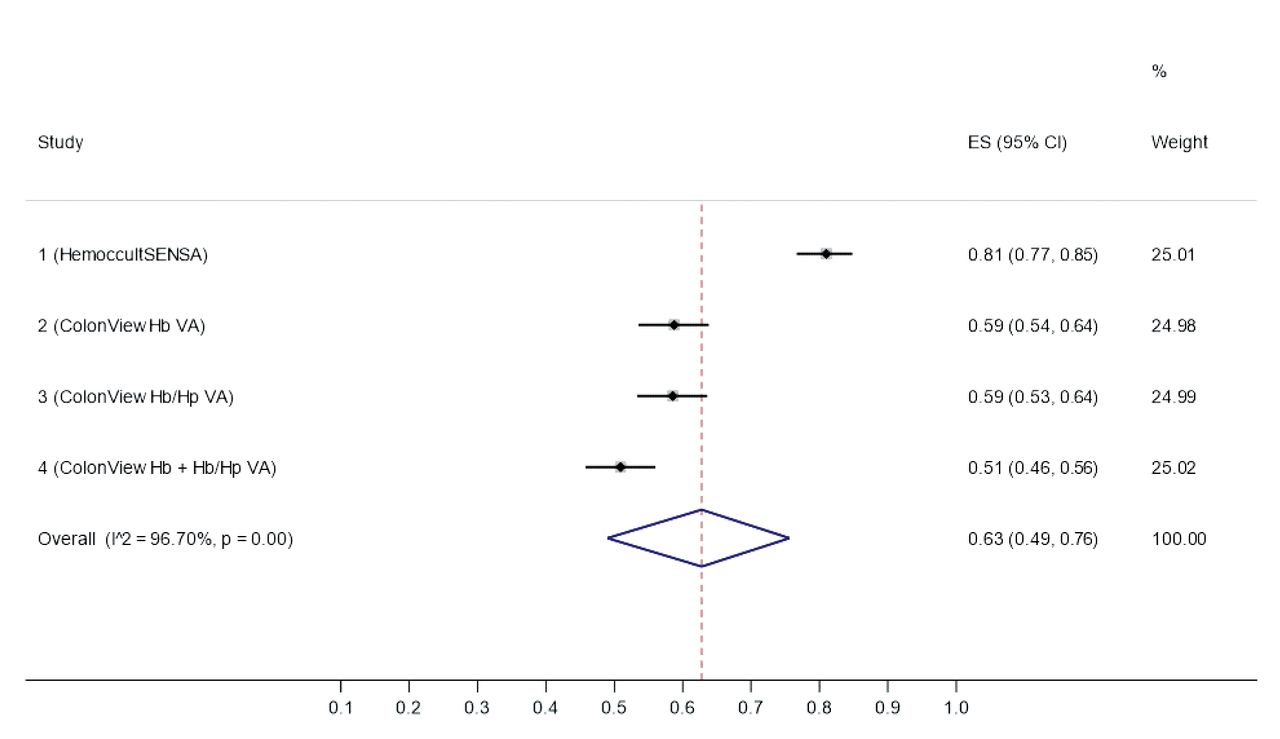
Diagnostic accuracy of the CV test in VA mode. The overall Se of the CV in the VA mode for detecting CRC was 89% (95%CI=81-95%) (Figure 3). The three most sensitive CV test VA panels (Hb VA, Hb/Hp VA, and Hb + Hb/Hp VA) showed 91-93% Se in diagnosis of CRC (Figure 3). The overall Sp of the VA mode was 63% (95%CI=49-76%) (Figure 4). The three most specific VA test modes showed Sp values of 59-81% (Figure 4).

Sensitivity values of visually analyzed (VA) screening tests for colorectal cancer endpoint. ES: Estimated sensitivity; CI: confidence interval.

Specificity values of visually analyzed (VA) screening tests for colorectal cancer endpoint. ES: Estimated specificity; CI: confidence interval.
Diagnostic accuracy of the CV test AA mode. The overall Se of the AA reading mode for detecting CRC was 90% (95%CI=84-95%) (Figure 5). The two most sensitive AA tests (Hb AA at cut-off ≥9.04, and Hb/Hp AA at cut-off ≥6.06) showed 95% Se (Figure 5). The overall Sp of the AA reading mode for the CRC endpoint was 77% (95%CI=59-91%) (Figure 6). The three most specific AA tests (Hb AA at cut-off ≥117, Hb/Hp AA at cut-off ≥48 and Hb + Hb/Hp AA) in CRC diagnosis showed Sp range of 86-93% (Figure 6).

Sensitivity values of automatically analyzed (AA) screening tests for colorectal cancer endpoint. ES: Estimated sensitivity; CI: Confidence interval.
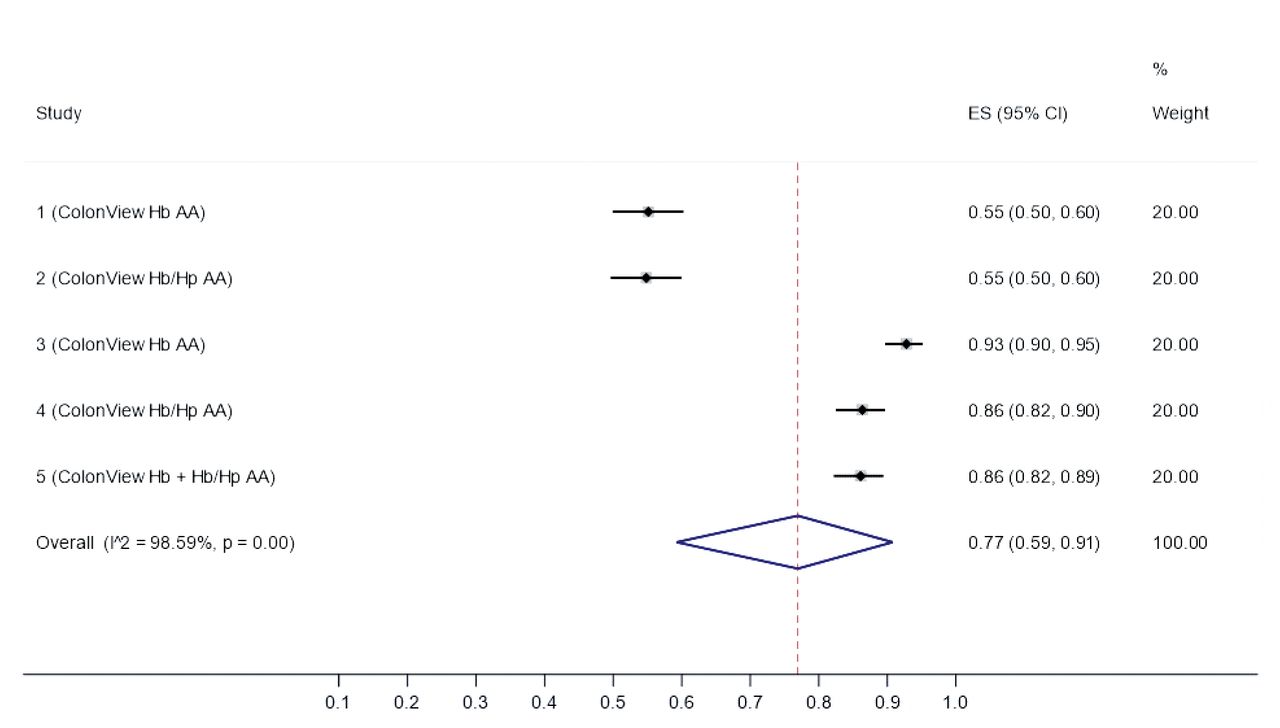
Specificity values of automatically analyzed (AA) screening tests for colorectal cancer endpoint. ES: Estimated specificity; CI: Confidence interval.
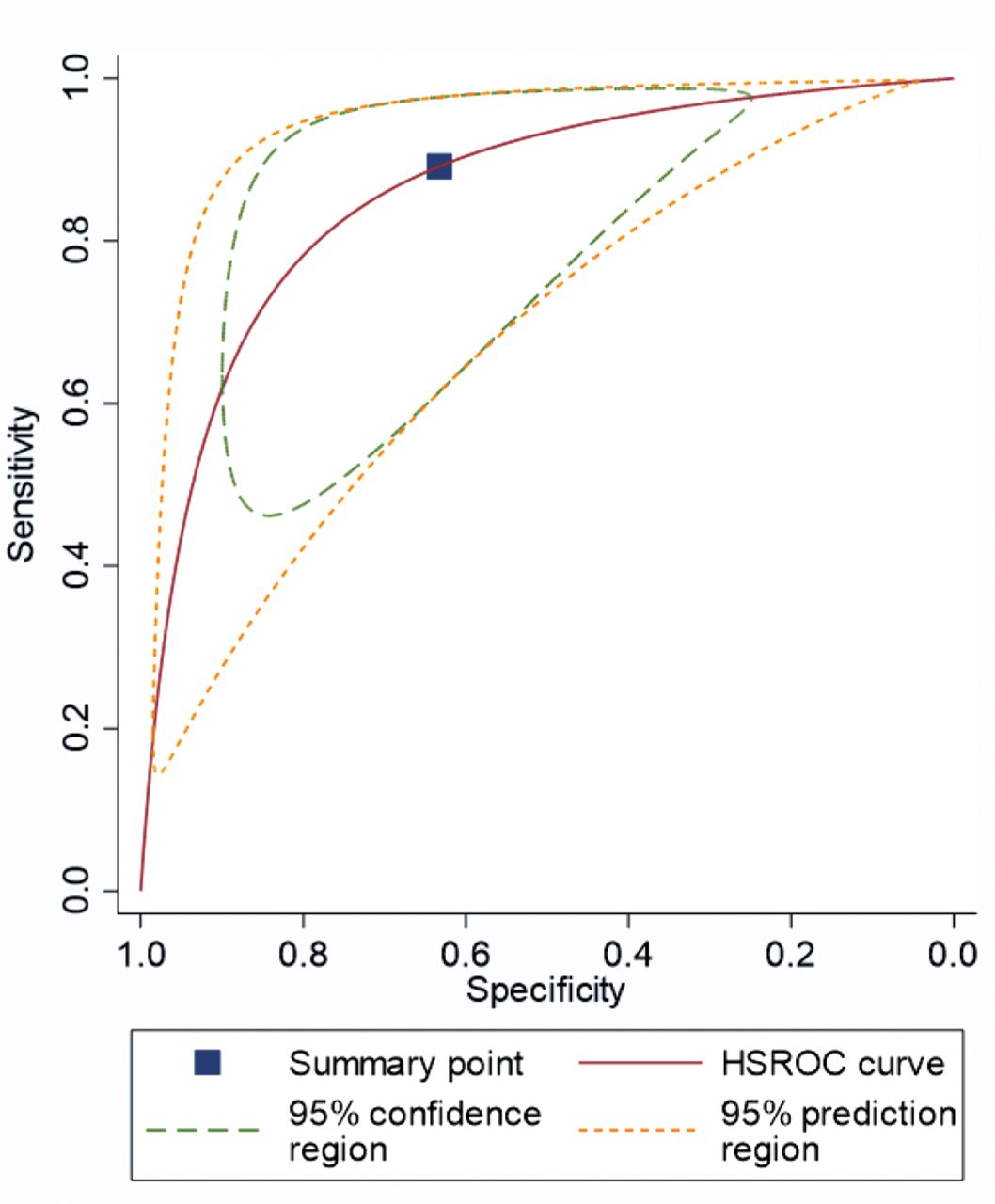
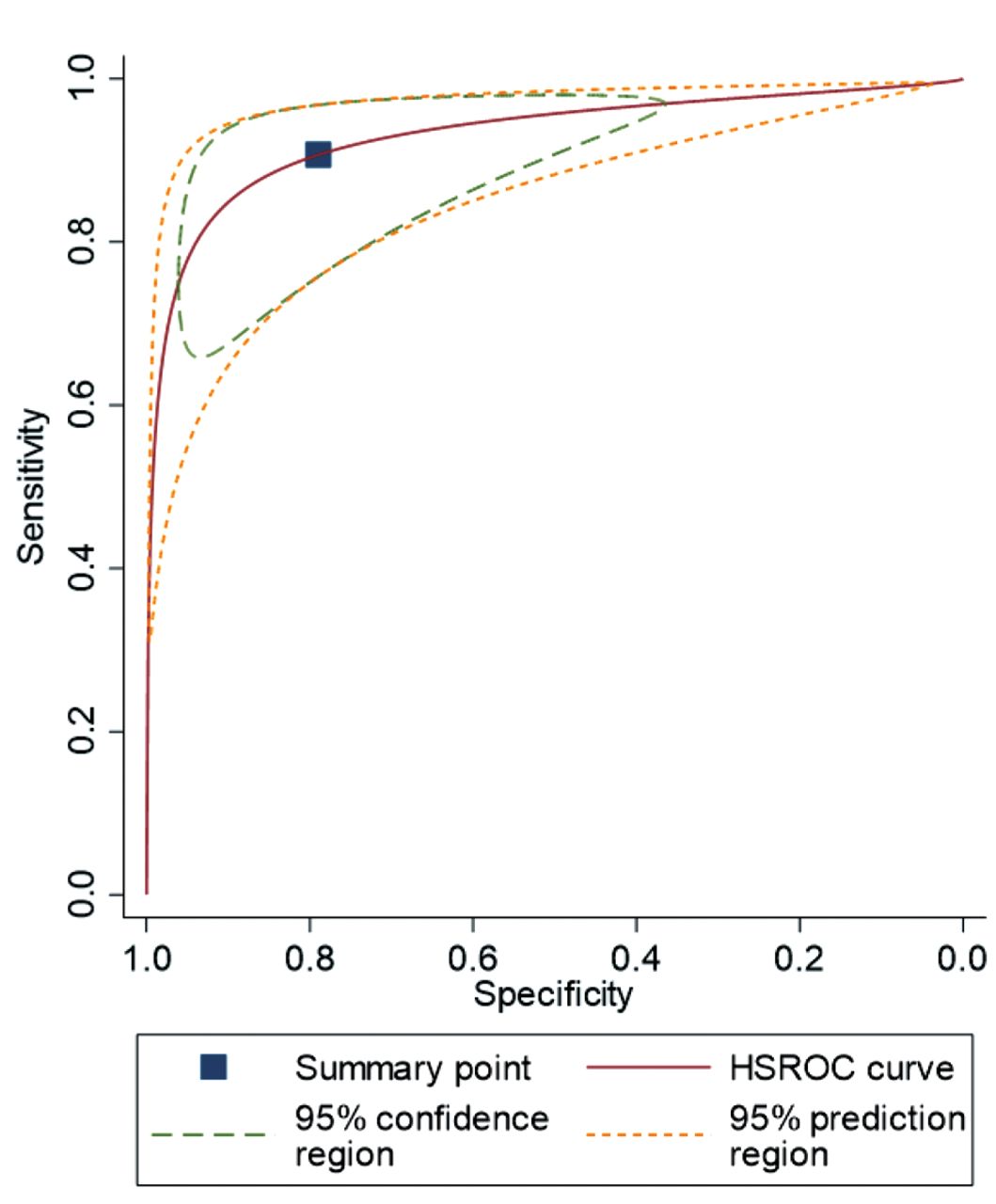
HSROC and AUC values. HSROC curves were used to visualize the pooled overall accuracy of VA (Figure 7) and AA (Figure 8) reading mode in CRC detection. In the HSROC analysis, the AUC values for i) VA and ii) AA modes were as follows: i) AUC=0.859 (95%CI=0.839-0.879) (Figure 7) ii) AUC=0.931 (95%CI=0.920-0.942) (Figure 8). The difference between these AUC values (Roccomp analysis) was statistically significant (p=0.0024).

Hierarchical summary receiver operating characteristic (HSROC) curve of the visually analyzed (VA) screening tests for colorectal cancer endpoint.

Hierarchical summary receiver operating characteristic (HSROC) curve of the automatically analyzed (AA) screening tests for colorectal cancer endpoint.
Discussion
Vasilyev et al. (11) and Guimaraes et al. (6) performed a head-to-head comparison study with SENSA and CV in two independent CRC screening settings. Both studies were concordant in that the characteristics of the iFOBT (CV) are superior to those of gFOBT (SENSA) as a screening tool for CRC (6-9). These results also corroborate with the position adopted by the European Union Guidelines for quality assurance in CRC screening, recommending FIT tests, because of their superior test characteristics as compared with the conventional gFOBTs (9). In brief, i) FITs have higher Se and Sp, ii) FITs can be automated and iii) the end user can adjust the cut-off at which positive result is reported, thus making the trade-off with false negatives, by taking into account the existing capacity for colonoscopies. In conclusion, FITs are currently the test-of-choice for population-based organised CRC screening (9).
The vast majority of FIT on the market are based on the detection of the globin moiety of human Hb, and few detect, in addition, the Hb/Hp complex. The advantages of testing both Hb and Hb/Hp complex are obvious, and have been discussed in detail in two recent communications (6, 11) as well as in our meta-analysis (8). As documented for the CV, the assay testing the Hb/Hp complex is 15% to 8% more sensitive than the detection of Hb alone, pending on the study endpoints used (11). This difference is most significant in the detection of proximal neoplasia, of which almost 60% and 50% are missed by the Hb component of the CV, respectively, as contrasted to 100% detection by the Hb/Hp complex (11). Although a plethora of FITs is currently on the market, relatively few have been extensively tested for clinical sensitivity and specificity in a CRC screening setting (8).
As shown in our recent meta-analysis (8), CV is superior to the traditional guaiac-based FOB tests (e.g. gFOBT, SENSA), making CV a perfect FIT for organized CRC screening. Interestingly, the guidelines of the WHO and World Organization for Digestive Endoscopy do recommend the combination of an initial gFOBT and a subsequent iFOBT (13), with the rational of reducing the number of FP results. One of the aims of the present study was to assess the diagnostic accuracy of SENSA and CV in detecting CRC among the colonoscopy-referral patients in a diagnostic setting. The study was focused, however, on comparing the diagnostic accuracy of the two different reading modes (VA, AA) of the ColonView quick test that has already established its usefulness in two independent CRC diagnostic settings (6, 11).
The results of the present study clearly confirm the conclusions of the Vasilyev et al. (11) and Guimaraes et al. (6) studies, implicating that CV is a highly accurate screening test for CRC. Even with the cancer endpoint, the Hb/Hp complex of the CV test reaches slightly higher diagnostic performance than Hb alone (AUC=0.924 and AUC=0.918, respectively). Using the other endpoints (adenoma, adenoma/carcinoma combined), this difference between Hb/Hp and Hb is much more accentuated (11). Undoubtedly, confirming the superiority of the Hb/Hp complex even for the cancer endpoint, must be considered as the single most important finding of the present study (Figure 2).
When the VA and AA reading modes are combined as a test panel, the accuracy for CRC endpoint is slightly decreased but still outstanding; AUC=0.900. Because of the fact that the AA mode of the CV test gives a quantitative reading, we wanted to find out the optimal cut-off points for Hb and Hb/Hp that give the best Se/Sp balance. This is neatly done by using conventional non-parametric ROC analysis (14, 15), selecting the coordinate points in the ROC curve as indicators of these cut-off values for Hb and Hb/Hp separately. The cut-off values have become increasingly important with the introduction of quantitative iFOBTs tests in which it is possible to adjust the cut-off limit to obtain an acceptable compromise between clinical sensitivity and specificity. This adjustment of the cut-off values can provide an adequate detection rate from an acceptable cohort of subjects invited for colonoscopy. By increasing the positive cut-off limit, the test Se and positivity rate decreases while the Sp and PPV for CRC detection increase (11). However, it is important to keep in mind that in any studies using different commercial products with different analytical characteristics, direct comparisons can be misleading.
The ColonView quick test, originally known as ColonView Hb and Hb/Hp Test (6, 11) is based on an immunochromatographic method, in which both Hb and Hb/Hp complexes are specifically recognized through specific antibody reactions. In brief, the test cassette strip is pre-coated with anti-human Hb and anti-human Hp antibodies on the Test region (T) and goat anti-mouse antibodies on the Control region (C). An anti-human Hb/Hp complex antibody-colloidal gold conjugate pad is placed at the end of the membrane. When human Hb/Hp complexes are present in the stool sample dissolved in buffered saline, the mixture of colloidal gold conjugate and extracted sample moves along the membrane, chromatographically by capillary action (16). In the case of a positive result, the molecules from the stool sample loaded with gold-marked antibodies attach to the test band (T) and are visible by means of a pink/red coloration. In the case of a negative result, there are no Hb molecules that can attach to the test band (T) as complexes and therefore, there is no coloration of the test band (T). If the control strip (C) turns red/pink in color, this shows that the sample has been correctly taken and has migrated properly, indicating that the test is technically valid (16).
For reading the CV test results, two optional modes are available: VA and AA (16). For the automatic reading, the Quick Test Reader (QTR) is needed. QTR is a mobile device for quantitative evaluation of lateral flow assays. The device is initially tested and configured by the original device manufacturer (opTricon GmbH), and subsequently validated and configured by Biohit (Biohit Oyj, Helsinki, Finland) for the use in CV AA reading (16). In this calibration, VA and AA are interlinked in that the weakest band visualised as positive (by several observers) was equivalent to the reader AA value of 20 ng/ml (11, 16).
In the previous studies, VA and AA reading modes were reported separately (6, 11). In this study, we wanted to focus on comparing the diagnostic accuracy of the two reading modes, using CRC endpoint is a screening setting. Different test scenarios were used similar as study IDs while analysing the pooled Se and Sp estimates in meta-analysis. The overall Se of the VA mode 89% (95%CI=81-95%) was quite similar than that of the AA reading mode 90% (95%CI=84-95%). However, the pooled Sp of the AA mode in detecting CRC (77%; 95%CI=59-91%), was significantly higher than that (63%; 95%CI=49-76%) of the VA reading mode.
HSROC analysis has become a convenient approach to evaluate the diagnostic accuracy of various diagnostic tests with different components that can be treated like study IDs in the HSROC analysis (14, 15, 17-21). Figure 7 shows the HSROC curve for the VA reading mode in CRC diagnosis, with a reasonably high AUC value (AUC=0.859; 95%CI=0.839-0.879). However, the diagnostic accuracy of the AA reading mode is clearly superior to the VA mode, with AUC=0.931 (95%CI=0.920-0.942) (Figure 8). These outstanding performance indicators of the CV (both VA and AA) favourably compete with the other FIT tests on the market, shown in a recent meta-analysis of Lee et al. 2014 (22) to exhibit pooled Se of 79% and pooled Sp of 94%. Using the formula AUC=(Se+Sp)/2, these pooled estimates give AUC=0.865, which is similar as here calculated for the VA reading mode (Figure 7), but clearly inferior to the AA reading mode.
Conclusion
The CV quick test interpreted using the automatic reading mode (AA) test showed significantly higher diagnostic accuracy for the CRC endpoint than did the VA reading mode, or the obsolete guaiac-based HemoccultSENSA test. As pointed out, caution should be followed while comparing the results of different quantitative FIT tests, because different commercial products have different analytical characteristics, and direct comparisons might be misleading. The limitation of this study is the colonoscopy-referral setting, because these patients represent a population with markedly higher CRC prevalence as compared with a native screening setting of asymptomatic subjects. These results clearly indicate that CRC screening by the CV quick test in its AA mode has the major benefit of avoiding unnecessary endoscopy or radiological procedures while keeping the false positive results at minimum.
Acknowledgements
The study was funded by the Päivikki and Sakari Sohlberg Foundation, Helsinki, Finland.
Footnotes
↵* These Authors contributed equally to this study.
Authors’ Contributions
All Authors contributed to the collection and analysis of data, drafting and revising the manuscript, read and approved the final article.
Conflicts of Interest
Jenni Inkinen, PhD, and Tapani Tiusanen, PhD, are employees of Biohit Company, Helsinki, Finland. The other Authors report no conflicts of interest or financial ties to disclose.
- Received August 16, 2021.
- Revision received September 1, 2021.
- Accepted September 2, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Colorectal Cancer Screening by Fecal Immunochemical Tests (FIT): Considerations on Sampling and Markers (Hb and Hb/Hp Complex) of Fecal Occult Blood (FOB)
- The Diagnostic Accuracy (DA) of ColonView Fecal Immunochemical Test (FIT) in Detecting Colorectal Adenoma (CRA) Can Be Improved by the Diagnostic Models (DM) that Include Triage and Risk Features of CRA
- Triage Process at Endoscopy With ColonView Fecal Immunochemical Test (FIT) Will Enhance Diagnostic Accuracy (DA) of Colorectal Cancer Screening
- Diagnostic Accuracy of Fecal Immunochemical Test (FIT) in Bleed-positive and Bleed-negative Colorectal Cancer (CRC) Among a Cohort of 5,090 Subjects who Participated in the Colorectal Neoplasia (CRN) Screening in Brazil
- Site-specific Performance of ColonView (CV) Fecal Immunochemical Test (FIT) With Differences Between Proximal and Distal Colorectal Adenoma
- The ColonView (CV) Quick Test for Fecal Occult Blood Shows Significantly Higher Diagnostic Accuracy in Detecting Distal than Proximal Colorectal Cancer
- The Automatically Analyzed (AA) ColonView (CV) Quick Test for Fecal Occult Blood Shows Higher Diagnostic Accuracy in Detection of Colorectal Adenoma than Visually Analyzed Tests