


Abstract
Background/Aim: Definitive radiotherapy for bone and soft tissues sarcomas benefits patients deemed unfit for surgery; poor outcomes have been reported with conventional photons, while interesting preliminary results have been described with particle in single-Institution experiences. The aim of the study was to retrospectively evaluate preliminary results of carbon ion radiotherapy (CIRT) in patients with axial bone and soft tissue sarcomas (BSTS) treated with curative intent at the National Center for Oncological Hadrontherapy (CNAO). Patients and Methods: From January 2013 to September 2018, 54 patients with axial BSTS were treated with CIRT at CNAO. Their median age was 50 years (range=19-79 years), males/females=1.4:1. Tumor site was the pelvis in 50% of cases (n=27), thoracic region in 24% (n=13), cervical spine in 15% (n=8) and lumbar in 11% (n=6). A total of 76% (n=41) of patients had primary disease, while 24% (n=13) had recurrent disease. Before CIRT, surgery was performed in 47% of cases, including positive margins (R1) in 8 patients, and macroscopic residual disease (R2) in 17. Histological subtypes were mainly represented by chondrosarcomas in 39% (n=21) of patients and osteosarcomas in 24% (n=13). Pre-treatment chemotherapy was administered in 40% of cases (n=22); no patient received previous radiotherapy. All treatments were performed with active scanning CIRT for a median total dose of 73.6 Gy (range=70.4-76.8 Gy), in 16 fractions (4 fractions per week). Results: Median follow-up was 24 months (range=4-61 months). Four patients were lost to follow-up. Acute toxicities were mild, no >G2 event was reported and no treatment interruption was required. For late toxicity, only G3 neuropathy was detected in 4% of cases (n=2). With a median time to local progression of 13 months (3-35), 15 local failures were observed, resulting in 2- and 3-year local control rates of 67.4% for both. Distant progression occurred in 12 patients, with 1-year progression-free survival (PFS) rate of 97.5%; 2- and 3-year rates were 92.2%. Fifteen patients died resulting in 1- 2- and 3-years overall survival (OS) rates of 87.1%, 75.4% and 64%, respectively. At log-rank test, gross total volume (GTV) >1,000 ml was found to be predictive of local failure (p=0.04), pre-treatment chemotherapy was found to be significantly related to PFS and OS (p=0.02 and p=0.016); also, recurrent disease and distant progression were significantly related to OS (p=0.019 and p=0.0013). Cox proportional-hazards model confirmed that GTV >1,000 ml was related to worse local control (p=0.0010). Conclusion: CIRT for axial BSTS resulted in mild toxicity, showing promising results in terms of clinical outcomes. A longer follow-up is warranted.
Surgery represents the milestone in the treatment of bone and soft tissue sarcomas (BSTS). When radical, R0 resection is performed local recurrence rate at 5 years has been reported in 6% compared to 38% in R2 patients (1-3). In this scenario, radiotherapy (RT) can be managed both in the pre- or post-surgery setting, and several studies are currently available about the peri-operative role of radiotherapy in the management of sarcomas (4, 5).
On the other hand, the role of RT for macroscopic disease (unresectable or residual after incomplete surgery) is still controversial and literature data are scarce, mainly represented by conventional photons experiences reporting unsatisfactory outcomes: Kepka et al. reported, for inoperable patients treated with doses of 63 Gy or higher, 5-year local control (LC), disease-free survival (DFS), and overall survival (OS) rates of 60%, 36%, and 52%, respectively, while in patients treated with lower doses 5-year LC, DFS, and OS rates of 22%, 10%, and 14% (6-9).
Literature studies of particle therapy for bone and soft tissue sarcomas (* indicates 3-years rates).
BSTS are known for their radio-resistant biological behaviour, requiring for high doses of radiotherapy to gain adequate local control (3). However, despite the advances in technology that allow for a more precise target coverage, in cases of tumors close to more sensitive healthy structures, reaching curative doses with conventional photons is still challenging (10).
During the last years, the role of particle RT has become more attractive due to the physical selectivity of both protons and carbon ions and the possibility to deliver a high curative dose to the target with a minimal exposure of nearby organs at risk (OARs). Deposition of dose in the so called “Bragg peak” region provides a more favourable dose-distribution compared to photons. Moreover, unlike protons, carbon ions combine their peculiar physical properties with a higher biological effect that can be more useful in the treatment of more radio-resistant tumors. Literature data on the use of carbon ions for BSTS are sparse, also due to the low availability of this technology (Table I) (11-22).
Herein, we report our experience of the National Center for Oncological Hadrontherapy (CNAO) of carbon ion radiotherapy (CIRT) for the treatment of unresectable or incompletely resected BSTS of the axial skeleton.
Patients and Methods
This study is a retrospective analysis evaluating preliminary outcomes of 54 patients with axial BSTS who were treated with curative intent from January 2013 to September 2018. Informed consent was obtained from all participants included in the present series. All procedures were performed in agreement with the 1964 declaration of Helsinki.
For axial tumors we considered all the masses located below C2, as also described in previous studies (14). Main inclusion criteria were: histological diagnosis of BSTS, Karnofsky Performance Status ≥70, tumor deemed inoperable or not subject to further surgery, no prior radiotherapy, absence of metal prostheses that could affect treatment planning.
Pre-treatment evaluation included physical examination, magnetic resonance imaging (MRI) of the primary lesion and chest-abdomen contrast computed tomography (CT). Additional imaging was required at the discretion of the radiation oncologist.
Radiotherapy (RT) protocol. For each patient a 2-mm thick slice CT was acquired for treatment planning using a customized thermoplastic mask and a polystyrene pillow in the supine or prone position. The same immobilization protocol was observed for the acquisition of a contrast-enhanced MRI for rigid registration.
For tumors subject to physiological motion, image acquisition was coupled to a pressure sensor (AZ-733V system, Anzai Medical Co. Ltd., Japan) placed between the patient body and the solid mask. 4-D Computed tomography (4DCT) image datasets were retrospectively reconstructed using the external respiratory surrogate signal at the respiratory end-exhale phase (23-25).
Target volume and organ-at-risk delineation was performed using CT-MRI image fusion. Gross tumor volume (GTV) consisted of macroscopic disease; clinical target volume (CTV) was generated by adding an isotropic margin of 10-30 mm depending on the location of the primary tumor and further modified based on the possible anatomical spreading pathway of the primary tumor. Planning target volume (PTV) was defined as CTV plus a 3-5 mm margin. Carbon ion beams were generated using an in-house built synchrotron (26).
Treatment planning was performed using Syngo RT Planning TPS, version C13, and the biological effectiveness of the particle beam was incorporated in the planning software according to the Local Effect Model (LEM) version I, as previously reported, and intensity modulated particle therapy (IMPT) was employed for optimization (27, 28).
CIRT was delivered using active scanning technique adopting a 16-fractions schedule delivered in four weeks, for a total dose ranging from 70.4 Gy(RBE) to 76.8 Gy(RBE). For moving targets, motion mitigation strategy consisted of mild abdominal compression, and beam was delivered by gating at the respiratory end-exhale phase (≈1 s gating window) with layer rescanning (25). In fact, patient respiratory motion introduces uncertainties in the delivered dose distribution. To reduce possible dosimetric variations, respiration amplitude is limited by a mild compression due to the thermoplastic mask. In addition, the treatment is coupled to the patient respiratory signal and delivered only at the specific phase (end-exhale) used for plan optimization. Local target under- and over-dosages due to synchronization between respiratory signal and beam scanning path are avoided by rescanning each slice of the target five times.
Patients characteristics.
Clinical outcomes and toxicity assessment. After the end of CIRT, follow-up was conducted every 3 months with magnetic resonance imaging (MRI) for the first 2 years and then every 6 months. Chest-abdomen CT with contrast was performed at least on a semi-annual basis. Local control (LC) was defined as no evidence of progressive disease in the PTV area, while distant progression-free survival (DPFS) as the absence of any failure outside the PTV area.
Toxicity assessment was based on Common Terminology Criteria for Adverse Events (CTCAE) v4.0 (29), assuming acute toxicity as any event occurring within 90 days from the start of treatment, while late toxicity was considered as any event occurring after 90 days.
Statistical analysis. Descriptive statistics were summarized for baseline patients' characteristics. Medians, means and ranges were collected for continuous variables. Time-to-event data were calculated using the Kaplan–Meier method and log-rank test for individual comparisons, then Cox proportional hazards models were performed. All statistical analyses were carried out using the Medcalc statistical software package v.18.11.3 (Mariakerke, Belgium). A p-value ≤0.05 was deemed statistically significant.
Results
Between January 2013 and September 2018, 54 patients with unresectable or incompletely resected BSTS were treated with CIRT at the National Center of Oncological Hadrontherapy. Four patients were lost at follow-up. Patients' characteristics are summarized in Table II.
Median age was 50 years (range=19-79 years), males: females=1.4:1. The most frequent tumor location was the pelvis in 50% of cases (n=27), followed by the thoracic region in 24% (n=13), the cervical and lumbar spine respectively in 15% (n=8) and 11% (n=6). A total of 76% (n=41) of patients had primary disease, and recurrent disease was observed in 24% (n=13). Histological subtypes were mainly represented by chondrosarcoma in 39% (n=21) and osteosarcoma in 24% (n=13) of cases. Chordomas were excluded from this analysis. Data about histological grading according to the French Federation Nationale des Centers de Lutte Contre le Cancre (FNCLCC) system were unavailable for 8 patients due to insufficient specimen or unknown reasons.
Surgery before CIRT was carried out in 25 cases, including positive margins (R1) in 8 subjects and macroscopic residual disease (R2) in 17. Pre-treatment chemotherapy was administered in 40% of cases (n=22). All patients were treated with CIRT for a median total dose of 73.6 Gy(RBE) (range=70.4-76.8 Gy) delivered in 16 fractions (4 fractions per week); median daily dose was 4.6 Gy(RBE) (range=4.4-4.8 Gy). Median GTV and PTV were 268 ml (range=72-3,200) and 1,178 ml (range=178-6,597), respectively.
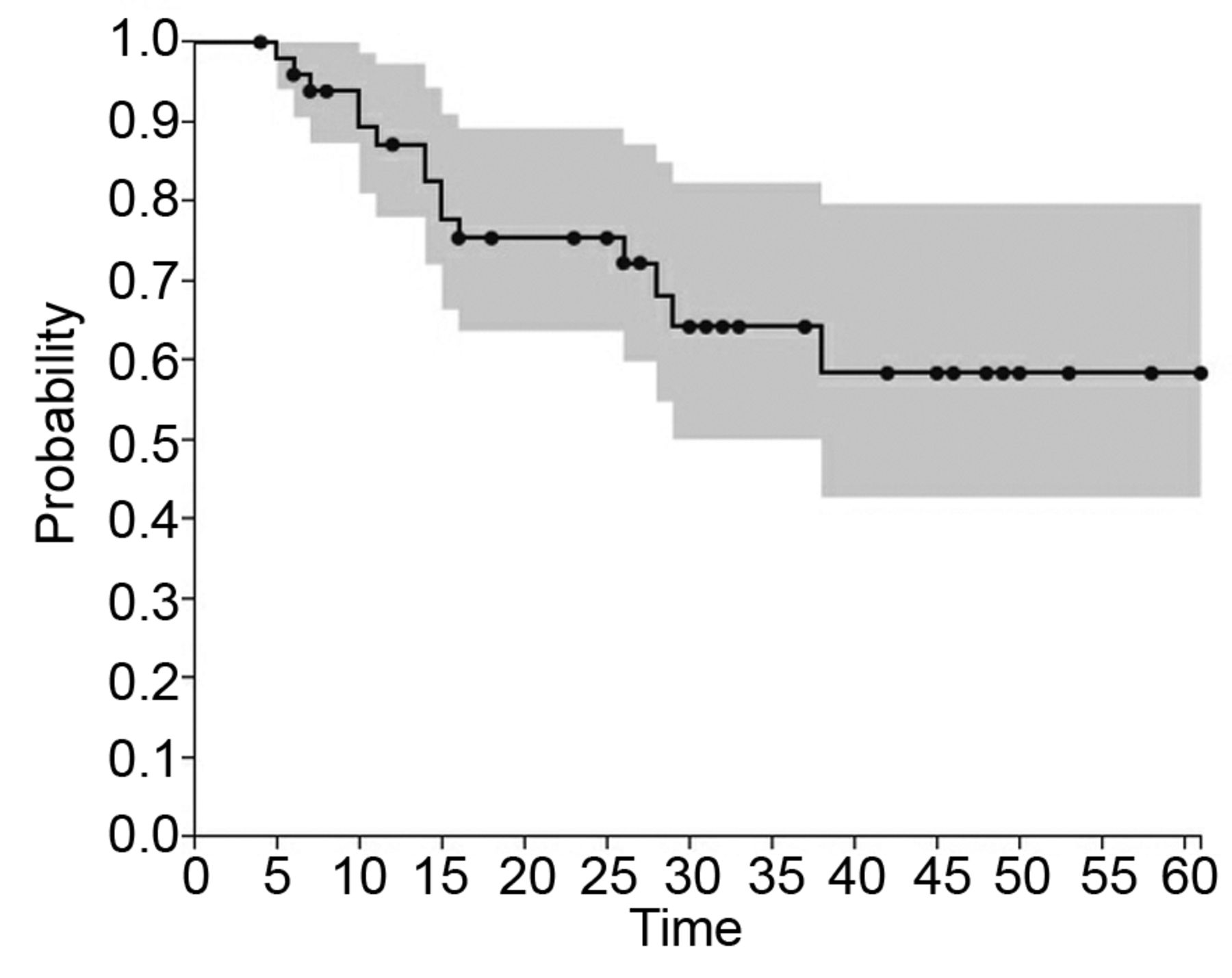
Treatment was well tolerated and conducted with no interruptions; acute toxicities were mild and no higher than G2 events were observed. For late toxicity, only two cases of G3 neuropathy were found. With a median follow-up of 24 months (range=6-61 months), 15 patients experienced a local failure with a median time to progression of 13 months (range=3-35 months), resulting in 1-year LC rate of 84.8%, 2- and 3-year LC were both 67.4% (Figure 1).
Log-rank test (Table III) revealed that GTV >1,000 cc was found to be predictive of local failure (p=0.04). This correlation was also confirmed with Cox regression test (p=0.001) (Table IV).
Distant progression was detected in 12 patients with 1, 2- and 3-year DPFS rates of 97.5% and both 92.2%. Fifteen patients died resulting in 1-, 2- and 3-year overall survival rates of 87.1%, 75.4% and 64%, respectively. Among these 15 patients, 6 died by disease progression (Figures 2 and 3). At log-rank, pre-treatment chemotherapy significantly related to DPFS (p=0.02) and OS (p=0.016); also, recurrent disease and distant progression showed a significant correlation with OS (p=0.019 and p=0.0013).

Kaplan-Meier curve for local control (LC) of the study population.
Discussion
Wide surgical resection still represents the main treatment option for BSTS, since it results in better outcomes. Usually, radiotherapy offers an ancillary function to surgery, by providing with neoadjuvant treatment a lower incidence of positive margins, or with post-operative intent, a complementary therapeutic option in order to improve local control (30). Conventional RT alone concerns a small number of cases deemed unfit for complete resection, due to high morbidity or poor functional outcomes and typically represents a palliative treatment.
In the last years, the role of particle therapy, particularly of carbon ions, has been explored in light of the potential offered by charged particles to combine a higher biological effect with a better sparing of adjacent normal structures and has been described as an effective alternative to surgery for inoperable spinal and paraspinal sarcomas (Table I) (11-22). A recent study aimed to characterize the potency and impact of CIRT in a primary mouse model of soft tissue sarcoma calculated for a tumor growth delay endpoint an RBE of 3 (31).
Our series report preliminary data showing promising results in terms of clinical outcomes with a negligible incidence of adverse events, supporting the use carbon ions for unresectable or incompletely resected BSTS in order to provide a safe and beneficial treatment for this subset of patients.
To the best of our knowledge, the largest experience available in the literature is reported by Imai et al. (14) concerning a retrospective series of 188 sacral chordomas treated with curative CIRT reporting excellent 5-years LC, OS and DPFS rates of 77.2%, 81.1%, and 50.3%, respectively, with minimal toxicity incidence. Unlike the aforementioned experience, chordomas have not been analyzed in our series because of their intrinsic slow-growing features and their peculiar biological characteristics that make them different to other sarcomas. Similarly, promising data have been reported in another study by Imai et al. in a retrospective analysis of 73 patients with unresectable chondrosarcoma treated with CIRT (32). More recently, the same authors published data on 128 patients with axial soft tissue sarcomas showing 5-year LC, OS and DPFS rates of 65%, 46% and 39%, observing a significant correlation between tumor size, local control and OS. Moreover, four cases of ≥G3 events were described, including one case of G4 toxicity (12).
Log-rank results.
Cox proportional hazards model results.

Kaplan-Meier curve for distant progression-free survival (PFS) of the study population.
In our cohort, tumor volume was significantly related to LC with the highest incidence of failures (13 out of 15) occurring within the first two years after RT; particularly, both log-rank and Cox regression reported that a GTV >1,000 ml was associated to a higher incidence of local failure (p=0.04 and p=0.001); no other factors were found to be predictive of LC. The negative impact of tumor volume on LC is reported by several authors, regardless of the RT technique, focusing the complexity of providing curative doses to larger volumes without compromising the nearby healthy structures.
Regarding toxicity, our experience reported mild acute or late adverse events, with only two late G3 cases. On the contrary, in one of the largest experiences of 112 patients treated with curative conventional RT for unresectable soft tissue sarcomas, Kepka et al. reported higher local control rates for higher radiation doses, despite being associated with an increased incidence of adverse events, thus reinforcing the potential role of CIRT in improving the therapeutic ratio for the treatment of these radioresistant tumors (33).
Given their intrinsic dosimetric characteristics, in fact, heavy particles and, especially, carbon ions manage to concentrate their dose to the tumor with a great sparing of the surrounding healthy tissues and this spatial selectivity makes them more advantageous compared to photons. The greater control in the literature ascribed to the particles is probably related to their high biological efficacy, estimated to be 2- to 3-times greater than photons, which makes them more aggressive and therefore more competitive than photons for histologies, such as sarcomas, known to be radio-resistant. Both the DNA damage, difficult to repair by intracellular checkpoint mechanisms, done by CIRT and the action of carbon ions that is independent of the oxygen effect and/or the phase of the cell cycle in which a cell is located, account for the greater cell killing shown in vivo and in vitro (34).
Kaplan-Meier curve for overall survival (OS) of the study population.
Concerning OS rates, unlike other studies, in the present study tumor volume did not reach a statistically significant correlation with OS, despite the fact that a trend toward a negative impact can be observed (p=0.06); nevertheless, our 3-year data are in agreement with previously published reports, similarly reporting that distant progression and recurrent disease were significantly associated with worse OS (13, 18).
Regardless of the type of local treatment, almost 50% of patients with BSTS will face distant progression and die because of systemic disease (35, 36). The role of neoadjuvant chemotherapy has been investigated along to that of surgery for several years with conflicting results reported from several trials, providing insufficient data to produce a definitive recommendation (37). Recently, the ISG-STS 1001 randomized trial showed a significant benefit from conventional neoadjuvant chemotherapy over histology-driven chemotherapy in a cohort of 287 patients with high-risk soft tissue sarcomas (STS), supporting a potential prognostic advantage in terms of DPFS and OS given by neoadjuvant chemotherapy, particularly for patients with high malignancy grading and tumor size >5 cm (38).
In agreement with these data, in our series pre-RT chemotherapy was associated with better distant metastases and overall survival rates. Of course, the small sample size must be kept into account; nevertheless, further prospective trials will clarify the role of neoadjuvant chemotherapy for BSTS.
The present study had several limitations: the retrospective nature of this analysis limits its statistical power, the relatively small size of our cohort and the follow-up time must be considered, despite being comparable to other experiences in literature.
Conclusion
Preliminary results of definitive CIRT for BSTS support the use of particle therapy as a safe and effective treatment option for patients unfit for surgery. In our experience, a larger GTV was related to a higher incidence of local failure, while pre-RT chemotherapy showed a significant relation with DPFS and OS. Recurrent disease and distant metastases were significantly related with a worse OS. A longer follow-up is warranted for a complete evaluation of the present series.
Acknowledgements
None of the Authors involved in this study received financial support.
Footnotes
Authors' Contributions
VV: Conceived the study, methodology and editing; FC: wrote the original draft; AB: data curation, methodology and editing; AF: data collection; AV: treatment planning, editing. MRF, AI, BV, SR, GR, LP, FV: review. All Authors approved the final version of the manuscript.
Conflicts of Interest
The Authors declare that they have no conflicts of interest.
- Received March 12, 2020.
- Revision received March 25, 2020.
- Accepted March 28, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}
{kind=link}
{kind=link}